You might also like
- Depression As An Evolutionary Strategy For Defense Against InfectionDocument14 pagesDepression As An Evolutionary Strategy For Defense Against InfectionOscar Alejandro Cardenas Quintero100% (2)
- Roy Byrne2006Document10 pagesRoy Byrne2006rj6cv4tdfrNo ratings yet
- Coping With Covid-19: Resilience and Psychological Well-Being in The Midst of A PandemicDocument11 pagesCoping With Covid-19: Resilience and Psychological Well-Being in The Midst of A PandemicMáthé AdriennNo ratings yet
- The Impact of September 11 On Psychologists: Roy J. Eidelson and Gerard R. D'Alessio Judy I. EidelsonDocument7 pagesThe Impact of September 11 On Psychologists: Roy J. Eidelson and Gerard R. D'Alessio Judy I. EidelsonGonzalo ParedesNo ratings yet
- 2021 Gutiérrez-Hernández COVID-19 Lockdown and Mental Health in A Sample PopulationDocument15 pages2021 Gutiérrez-Hernández COVID-19 Lockdown and Mental Health in A Sample PopulationElena Gutiérrez HernándezNo ratings yet
- Mental Health Is Biological Health. Why Tackling Diseases of The Mind Is An Imperative For Biological Anthropology in The 21st CenturyDocument31 pagesMental Health Is Biological Health. Why Tackling Diseases of The Mind Is An Imperative For Biological Anthropology in The 21st CenturyWalter VillalobosNo ratings yet
- Applied Psy Unit 3Document13 pagesApplied Psy Unit 3Thant AungNo ratings yet
- SARS Control and Psychological Effects of QuarentineDocument2 pagesSARS Control and Psychological Effects of QuarentineCarolina ValenciaNo ratings yet
- A Systematic Review of The Impact of Disaster On The Mental Health of Medical RespondersDocument12 pagesA Systematic Review of The Impact of Disaster On The Mental Health of Medical RespondersGustavo LimachiNo ratings yet
- Anxiety Disordes Lancet 2016Document12 pagesAnxiety Disordes Lancet 2016sOniEh pALNo ratings yet
- Ugay - Impact of Disasters On Mental HealthDocument2 pagesUgay - Impact of Disasters On Mental HealthNicoleNo ratings yet
- Holmes2021 Article ImpactOfCOVID-19PandemicOnPostDocument10 pagesHolmes2021 Article ImpactOfCOVID-19PandemicOnPostSyarifahNo ratings yet
- Journal of A Ffective Disorders: Christian Jasper C. Nicomedes, Ronn Mikhael A. Avila TDocument9 pagesJournal of A Ffective Disorders: Christian Jasper C. Nicomedes, Ronn Mikhael A. Avila TArgonne Robert AblanqueNo ratings yet
- Morbid Anxiety As A Risk Factor in Patients With Somatic Diseases A Review of Recent FindingsDocument9 pagesMorbid Anxiety As A Risk Factor in Patients With Somatic Diseases A Review of Recent FindingsAdelina AndritoiNo ratings yet
- Implementation of COVID 19 ProtocolsDocument10 pagesImplementation of COVID 19 ProtocolsJHON DERIC BATANG100% (1)
- Fussell and LoweDocument8 pagesFussell and LoweSUVAM BANERJEENo ratings yet
- The Social Construction of Contested Illness Legitimacy: A Grounded Theory AnalysisDocument21 pagesThe Social Construction of Contested Illness Legitimacy: A Grounded Theory AnalysisPelículasVeladasNo ratings yet
- 1 s2.0 S0163834309000814 MainDocument2 pages1 s2.0 S0163834309000814 MainHelenaNo ratings yet
- Minihan - COVID-19, Mental Health and Psychological First Aid - 2020Document5 pagesMinihan - COVID-19, Mental Health and Psychological First Aid - 2020Donald CabreraNo ratings yet
- Stress Management in A Working EnvironmentDocument21 pagesStress Management in A Working EnvironmentmtwlzeroNo ratings yet
- Schizophrenia PaperDocument21 pagesSchizophrenia PaperBagoes Ario BimoNo ratings yet
- JURSW v7 05 DriskillDocument14 pagesJURSW v7 05 DriskillLibrary ZNo ratings yet
- HHS Public Access: Developmental Vitamin D Deficiency and Schizophrenia: The Role of Animal ModelsDocument30 pagesHHS Public Access: Developmental Vitamin D Deficiency and Schizophrenia: The Role of Animal ModelsIqbal AbdillahNo ratings yet
- Evidence of Mental Health Risks Climate Warm 2018Document6 pagesEvidence of Mental Health Risks Climate Warm 2018Paula GutierrezNo ratings yet
- 2020 Article 728Document10 pages2020 Article 728Ory LarasNo ratings yet
- PTSD Outcome, Adjustment Disorder and Methods of TreatmentDocument7 pagesPTSD Outcome, Adjustment Disorder and Methods of TreatmentSabrina JonesNo ratings yet
- Post-Traumatic Stress Disorder and Coping Among CaDocument11 pagesPost-Traumatic Stress Disorder and Coping Among Caearl salcedoNo ratings yet
- In Uence of Psychological Stress On Upper Respiratory Infection-A Meta-Analysis of Prospective StudiesDocument11 pagesIn Uence of Psychological Stress On Upper Respiratory Infection-A Meta-Analysis of Prospective StudiesThang LaNo ratings yet
- Anxiety RabuDocument5 pagesAnxiety RabuharioNo ratings yet
- Original 2Document15 pagesOriginal 2tafazzal.eduNo ratings yet
- Identifying Resilience Factors of Distress and Paranoia During The COVID-19 Outbreak in Five CountriesDocument16 pagesIdentifying Resilience Factors of Distress and Paranoia During The COVID-19 Outbreak in Five Countriesdimasfathah1295No ratings yet
- Music Therapy For Preoperative Anxiety in Surgical Patients - An IDocument136 pagesMusic Therapy For Preoperative Anxiety in Surgical Patients - An IsantiNo ratings yet
- Searching For and Finding Meaning in Collective TRDocument27 pagesSearching For and Finding Meaning in Collective TRhushsNo ratings yet
- 5 Western Models For Mental Health BentallDocument4 pages5 Western Models For Mental Health BentallimanuelcNo ratings yet
- The Epidemiology of Post-Traumatic Stress Disorder After DisastersDocument14 pagesThe Epidemiology of Post-Traumatic Stress Disorder After Disastersrose anne SeballoNo ratings yet
- Thesis "At What Cost"Document14 pagesThesis "At What Cost"Maria Victoria A. Praxides100% (1)
- Prediction ZoonosisDocument10 pagesPrediction ZoonosisPaul WallNo ratings yet
- Depression As A Systemic Syndrome Mapping The Feedback Loops of Major Depressive DisorderDocument12 pagesDepression As A Systemic Syndrome Mapping The Feedback Loops of Major Depressive DisordersahojjatNo ratings yet
- A Meta-Analysis of Neuropsychological Markers of Vulnerability To Suicidal Behavior in Mood DisordersDocument12 pagesA Meta-Analysis of Neuropsychological Markers of Vulnerability To Suicidal Behavior in Mood DisordersWALTER DE PAZNo ratings yet
- Social Science QuestionDocument7 pagesSocial Science QuestionJanetNo ratings yet
- Depression Discussion PaperDocument14 pagesDepression Discussion Paperpinky giradoNo ratings yet
- Psychology Discussion 4+5Document5 pagesPsychology Discussion 4+5Susan SuNo ratings yet
- The Research Essay: "Is Mental Illness Over Diagnosed During These Unprecedented Times?"Document11 pagesThe Research Essay: "Is Mental Illness Over Diagnosed During These Unprecedented Times?"api-583333269No ratings yet
- Can A Pandemic Make People More Socially Conservative? Longitudinal Evidence From COVID-19Document22 pagesCan A Pandemic Make People More Socially Conservative? Longitudinal Evidence From COVID-19P AlexiaNo ratings yet
- H1N1 in Critically IllDocument9 pagesH1N1 in Critically IllmgolobNo ratings yet
- Coping During The COVID-19 Pandemic-Relations With Mental Health and Quality of LifeDocument9 pagesCoping During The COVID-19 Pandemic-Relations With Mental Health and Quality of LifeMariaNo ratings yet
- Death Anxiety, Loss, and Grief in The Time of COVID-19: Rachel E. Menzies, Robert A. Neimeyer and Ross G. MenziesDocument5 pagesDeath Anxiety, Loss, and Grief in The Time of COVID-19: Rachel E. Menzies, Robert A. Neimeyer and Ross G. MenziesLeonor AlmeidaNo ratings yet
- Psycho Neuroin Mun OlogyDocument3 pagesPsycho Neuroin Mun OlogyJoseNo ratings yet
- Why Does The Burden of Disease Persist Relating THDocument10 pagesWhy Does The Burden of Disease Persist Relating THArina CismaruNo ratings yet
- Anxiety, Depression and Stress Among General Population During Covid 19 Outbreak A Comparative StudyDocument4 pagesAnxiety, Depression and Stress Among General Population During Covid 19 Outbreak A Comparative StudyEditor IJTSRDNo ratings yet
- Stres Si AdolescentaDocument8 pagesStres Si AdolescentaMarcel NitanNo ratings yet
- CDC 7168 DS1Document11 pagesCDC 7168 DS1Diana PutriNo ratings yet
- Phobia and Fear of COVID-19: Origins, Complications and Management, A Narrative ReviewDocument11 pagesPhobia and Fear of COVID-19: Origins, Complications and Management, A Narrative ReviewDivs Divination DivinaNo ratings yet
- Shigemura 2020 Public Responses To The Novel CoroDocument2 pagesShigemura 2020 Public Responses To The Novel CoroawkNo ratings yet
- Seekingpro Journal of Neuro Science & Neurophysiology (SJNSN)Document6 pagesSeekingpro Journal of Neuro Science & Neurophysiology (SJNSN)Rupa VijayanNo ratings yet
- Neuropsicologia Conducta SuicidaDocument12 pagesNeuropsicologia Conducta SuicidaFanny FrEgosoNo ratings yet
- Prediction and Prevention of The Next Pandemic ZoonosisDocument10 pagesPrediction and Prevention of The Next Pandemic ZoonosisjavenacostaNo ratings yet
- Variaciobes en El Cuidado Maternal en La Infancia y Reactividad Al Estres Meaney 2000 PDFDocument11 pagesVariaciobes en El Cuidado Maternal en La Infancia y Reactividad Al Estres Meaney 2000 PDFmarielaNo ratings yet
- Epidemiology of Psychological DistressDocument31 pagesEpidemiology of Psychological DistressManuel Guilherme VooghtNo ratings yet
- Sixteenauthors2016Diagnostics Manual English 1.1Document133 pagesSixteenauthors2016Diagnostics Manual English 1.1French Sarah NeraNo ratings yet
- Integrated Management ManualDocument86 pagesIntegrated Management ManualbalajirajasekaranNo ratings yet
- Health, Safety and Environmental Management System ManualDocument92 pagesHealth, Safety and Environmental Management System ManualAlwyn Tauro100% (1)
- Gap Analysis & Risk AssessmentDocument47 pagesGap Analysis & Risk AssessmentKevin Thomas100% (2)
- (WHQ IMS PR009) Non Conformity Management r5 PDFDocument12 pages(WHQ IMS PR009) Non Conformity Management r5 PDFKerima MagatNo ratings yet
- Risk Based Thinking March 4 - FinalDocument38 pagesRisk Based Thinking March 4 - FinalFrench Sarah NeraNo ratings yet
- SRS75 Implementationofa IMSOperating Organizationsof Research ReactorsDocument181 pagesSRS75 Implementationofa IMSOperating Organizationsof Research ReactorsFrench Sarah NeraNo ratings yet
- Certificate of Expert Practice (CEP) in Quality Management: ModulesDocument2 pagesCertificate of Expert Practice (CEP) in Quality Management: ModulesFrench Sarah NeraNo ratings yet
- EMSCULPT For Hernia and LiposuctionDocument3 pagesEMSCULPT For Hernia and LiposuctionFrench Sarah NeraNo ratings yet
- Performance Planning and Review Procedure: 1 PurposeDocument8 pagesPerformance Planning and Review Procedure: 1 PurposeFrench Sarah NeraNo ratings yet
- No. 17 Guidelines For The Acceptance of Manufacturer's Quality Assurance Systems For Welding Consumables No. 17Document9 pagesNo. 17 Guidelines For The Acceptance of Manufacturer's Quality Assurance Systems For Welding Consumables No. 17French Sarah NeraNo ratings yet
- VA88 02 08 KresingerDocument10 pagesVA88 02 08 KresingerFrench Sarah NeraNo ratings yet
- OSH Management System PolicyDocument23 pagesOSH Management System Policyzahidahmed42No ratings yet
- Management Review Programme (Insert Year) : ISO 9001:2015 QMSDocument2 pagesManagement Review Programme (Insert Year) : ISO 9001:2015 QMSFrench Sarah NeraNo ratings yet
- Management Review Presentation - ASQ Granite Section 20110922Document40 pagesManagement Review Presentation - ASQ Granite Section 20110922French Sarah NeraNo ratings yet
- Policy and Procedure Development and Management V4Document22 pagesPolicy and Procedure Development and Management V4French Sarah NeraNo ratings yet
- Jamainternal Galea 2020 VP 200009Document2 pagesJamainternal Galea 2020 VP 200009French Sarah NeraNo ratings yet
- Occupational Safety and Health in Public Health EmergenciesDocument136 pagesOccupational Safety and Health in Public Health EmergenciesFrench Sarah NeraNo ratings yet
- The Leader's NetworkDocument11 pagesThe Leader's NetworkFrench Sarah NeraNo ratings yet
- Annual Management Review: 1. PurposeDocument2 pagesAnnual Management Review: 1. PurposeFrench Sarah NeraNo ratings yet
- Instruction Manual For Environmental Engineering DAVISDocument27 pagesInstruction Manual For Environmental Engineering DAVISimrandpt67% (3)
- OSH Management System PolicyDocument23 pagesOSH Management System Policyzahidahmed42No ratings yet
- Pandemia Influenza ENG 2 PDFDocument25 pagesPandemia Influenza ENG 2 PDFFrench Sarah NeraNo ratings yet
- Ethical LeadershipDocument6 pagesEthical LeadershipFrench Sarah NeraNo ratings yet
- DelegationDocument9 pagesDelegationFrench Sarah NeraNo ratings yet
- Conflict Management TrainingDocument9 pagesConflict Management TrainingFrench Sarah NeraNo ratings yet
- Time and Stress Management TrainingDocument9 pagesTime and Stress Management TrainingFrench Sarah NeraNo ratings yet
- Pandemia Influenza ENG 2 PDFDocument25 pagesPandemia Influenza ENG 2 PDFFrench Sarah NeraNo ratings yet
- Final Thoughts On LeadershipDocument10 pagesFinal Thoughts On LeadershipFrench Sarah NeraNo ratings yet
- Pr2 Grp3 First Revision For Chapter 1 2Document9 pagesPr2 Grp3 First Revision For Chapter 1 2Clarence BautistaNo ratings yet
- Well Being: Striving For Good Health in Tribal CommunitiesDocument39 pagesWell Being: Striving For Good Health in Tribal CommunitiesRose Weeks100% (1)
- Influenza Flow Chart: Homeopathic Remedy GuideDocument5 pagesInfluenza Flow Chart: Homeopathic Remedy GuideAtit Sheth100% (1)
- Health 8 - Module 5Document10 pagesHealth 8 - Module 5Lyka Bactong DICES MNKNo ratings yet
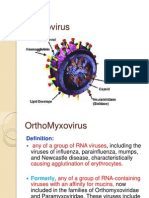
- OrthomyxovirusesDocument39 pagesOrthomyxovirusesማላያላም ማላያላምNo ratings yet
- 美国chemcon公司单抗目录(英文)Document20 pages美国chemcon公司单抗目录(英文)api-3742158No ratings yet
- Cobden Technical SchoolEMP2Document91 pagesCobden Technical SchoolEMP2competition1276No ratings yet
- Soal BHS InggrisDocument17 pagesSoal BHS InggrisMuza FairuzaNo ratings yet
- 5 Sat Practice TestsDocument26 pages5 Sat Practice TestsGand mein DandaNo ratings yet
- Ray Peat - The Bean SyndromeDocument6 pagesRay Peat - The Bean SyndromeMihai Dragomir100% (5)
- Secret Magic Spells of The Romany GypsiesDocument28 pagesSecret Magic Spells of The Romany Gypsiesakenaton4089% (63)
- Oral RevalidaDocument98 pagesOral RevalidaJay ArNo ratings yet
- Communicable Diseases ReviewerDocument13 pagesCommunicable Diseases ReviewerMarivic Salcedo McCreaNo ratings yet
- Antiviral DrugsDocument56 pagesAntiviral DrugsciccianoNo ratings yet
- ĐỀ 5Document5 pagesĐỀ 5Nguyễn HiệpNo ratings yet
- HIRA Ontario Province PDFDocument204 pagesHIRA Ontario Province PDFTri SubaktiNo ratings yet
- Week 3 ENGLISH 10 ACTIVITYDocument12 pagesWeek 3 ENGLISH 10 ACTIVITYNingning DesaculaNo ratings yet
- The Covid Lies UpdatedDocument31 pagesThe Covid Lies UpdatedSabinaNo ratings yet
- ANIMALS Singer MerrillDocument32 pagesANIMALS Singer MerrillBlythe TomNo ratings yet
- 1 Social Administrative and Management Sciences Q&A Content Ver1Document34 pages1 Social Administrative and Management Sciences Q&A Content Ver1bhaveshnidhi64100% (1)
- New Danish MMR Study Shows Autism Rate of 1 in 100-CDC Should Rush To Denmark!Document12 pagesNew Danish MMR Study Shows Autism Rate of 1 in 100-CDC Should Rush To Denmark!DISA01 LAPTOPNo ratings yet
- National Immunization ProgramDocument67 pagesNational Immunization ProgrameezahNo ratings yet
- Unit 3 Kuliah - Integrated ReadingDocument14 pagesUnit 3 Kuliah - Integrated ReadingHandika Firmana100% (1)
- Airborne DeseasesDocument10 pagesAirborne DeseaseswinarsohNo ratings yet
- Deconstructing The 1918 Spanish Flu PandemicDocument151 pagesDeconstructing The 1918 Spanish Flu PandemicFloyd Reynolds100% (2)
- Exerciții Pe TEXT 2Document27 pagesExerciții Pe TEXT 2Balanean TatianaNo ratings yet
- PHCP FinalsDocument43 pagesPHCP FinalsEli ChuaNo ratings yet
- 11 Chapter 1Document58 pages11 Chapter 1AmanNo ratings yet
- Covid - 19 - v4 2Document47 pagesCovid - 19 - v4 2dori aarlevNo ratings yet
- 18 07 2020 PDFDocument60 pages18 07 2020 PDFAlexandru Ionut0% (1)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesFrom EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesRating: 5 out of 5 stars5/5 (70)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeFrom EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeRating: 4.5 out of 5 stars4.5/5 (49)
- BORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONFrom EverandBORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONRating: 4.5 out of 5 stars4.5/5 (24)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (38)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreFrom EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreRating: 5 out of 5 stars5/5 (17)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (140)
- Winning the War in Your Mind: Change Your Thinking, Change Your LifeFrom EverandWinning the War in Your Mind: Change Your Thinking, Change Your LifeRating: 5 out of 5 stars5/5 (558)
- Triggers: How We Can Stop Reacting and Start HealingFrom EverandTriggers: How We Can Stop Reacting and Start HealingRating: 5 out of 5 stars5/5 (58)
- Embrace Your Weird: Face Your Fears and Unleash CreativityFrom EverandEmbrace Your Weird: Face Your Fears and Unleash CreativityRating: 4.5 out of 5 stars4.5/5 (124)
- Don't Panic: Taking Control of Anxiety AttacksFrom EverandDon't Panic: Taking Control of Anxiety AttacksRating: 4 out of 5 stars4/5 (12)
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaFrom EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaRating: 4.5 out of 5 stars4.5/5 (56)
- Summary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisFrom EverandSummary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (5)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionFrom EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNo ratings yet
- When Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionFrom EverandWhen Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionRating: 4 out of 5 stars4/5 (11)
- Are You Really OK?: Getting Real About Who You Are, How You’re Doing, and Why It MattersFrom EverandAre You Really OK?: Getting Real About Who You Are, How You’re Doing, and Why It MattersRating: 5 out of 5 stars5/5 (29)
- The Secrets of Vagus Nerve Stimulation: 18 Proven, Science-Backed Exercises and Methods to Activate Your Vagal Tone and Heal from Inflammation, Chronic Stress, Anxiety, Epilepsy, and Depression.From EverandThe Secrets of Vagus Nerve Stimulation: 18 Proven, Science-Backed Exercises and Methods to Activate Your Vagal Tone and Heal from Inflammation, Chronic Stress, Anxiety, Epilepsy, and Depression.Rating: 5 out of 5 stars5/5 (14)
- Vagus Nerve: A Complete Self Help Guide to Stimulate and Activate Vagal Tone — A Self Healing Exercises to Reduce Chronic Illness, PTSD, Anxiety, Inflammation, Depression, Trauma, and AngerFrom EverandVagus Nerve: A Complete Self Help Guide to Stimulate and Activate Vagal Tone — A Self Healing Exercises to Reduce Chronic Illness, PTSD, Anxiety, Inflammation, Depression, Trauma, and AngerRating: 4.5 out of 5 stars4.5/5 (16)
- Binaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationFrom EverandBinaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationRating: 5 out of 5 stars5/5 (9)
- Anxious for Nothing: Finding Calm in a Chaotic WorldFrom EverandAnxious for Nothing: Finding Calm in a Chaotic WorldRating: 4.5 out of 5 stars4.5/5 (1244)
- The Worry Trick: How Your Brain Tricks You into Expecting the Worst and What You Can Do About ItFrom EverandThe Worry Trick: How Your Brain Tricks You into Expecting the Worst and What You Can Do About ItRating: 4.5 out of 5 stars4.5/5 (107)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveFrom EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveRating: 4 out of 5 stars4/5 (250)