You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Thesis Statement Intro and ConclusionDocument2 pagesThesis Statement Intro and ConclusionamrhkmhNo ratings yet
- Eng1103 Group WorkDocument3 pagesEng1103 Group WorkamrhkmhNo ratings yet
- Activity 1 - Semi Solid Products - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008 (Document12 pagesActivity 1 - Semi Solid Products - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008 (amrhkmhNo ratings yet
- Transitionwordsargue PDFDocument2 pagesTransitionwordsargue PDFamrhkmhNo ratings yet
- KPJ Healthcare University College: Bph1073 Dosage Form Design and Dispensing IiDocument4 pagesKPJ Healthcare University College: Bph1073 Dosage Form Design and Dispensing IiamrhkmhNo ratings yet
- English Script PresentationDocument9 pagesEnglish Script PresentationamrhkmhNo ratings yet
- Argumentative Essay Revision NotesDocument3 pagesArgumentative Essay Revision NotesamrhkmhNo ratings yet
- Experiment #8: Aldehydes and KetonesDocument12 pagesExperiment #8: Aldehydes and Ketonesamrhkmh100% (1)
- Suppositories and Pessaries - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008)Document7 pagesSuppositories and Pessaries - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008)amrhkmhNo ratings yet
- SUPPOSITORIES CBL - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008) BPH7Document4 pagesSUPPOSITORIES CBL - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008) BPH7amrhkmh100% (1)
- CBL Assignment Organic ChemistryDocument11 pagesCBL Assignment Organic ChemistryamrhkmhNo ratings yet
- Surat Sokongan Bi KMJDocument1 pageSurat Sokongan Bi KMJamrhkmhNo ratings yet
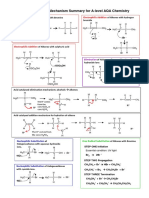
- Mechanism Summary For A-Level AQA Chemistry: BR BRDocument5 pagesMechanism Summary For A-Level AQA Chemistry: BR BRamrhkmhNo ratings yet
- Stereochemistry PDFDocument6 pagesStereochemistry PDFamrhkmhNo ratings yet
- Ointment - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008)Document8 pagesOintment - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008)amrhkmhNo ratings yet
- Substitution Reactions (S 2 Versus S 1) : Chemistry 5.12 Spring 2003, Handout #9Document2 pagesSubstitution Reactions (S 2 Versus S 1) : Chemistry 5.12 Spring 2003, Handout #9amrhkmhNo ratings yet
- Surat Iringan Bi KMJDocument1 pageSurat Iringan Bi KMJamrhkmhNo ratings yet
- Biochemistry Chapter 2Document12 pagesBiochemistry Chapter 2amrhkmhNo ratings yet
- ENG 1103 English For Healthcare ProfessionalsDocument2 pagesENG 1103 English For Healthcare ProfessionalsamrhkmhNo ratings yet
- Ulasan Artikel - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008) PDFDocument5 pagesUlasan Artikel - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008) PDFamrhkmhNo ratings yet
- Tutorial 1-ANSDocument7 pagesTutorial 1-ANSamrhkmhNo ratings yet
- Exercise Ready To PSPM, Matriculation (Science Computer)Document7 pagesExercise Ready To PSPM, Matriculation (Science Computer)amrhkmh100% (1)
- Pharmaceutical IncompatibilitiesDocument7 pagesPharmaceutical IncompatibilitiesamrhkmhNo ratings yet
- Biochemistry Chapter 1Document6 pagesBiochemistry Chapter 1amrhkmhNo ratings yet
- Unit 2 EnzymeDocument73 pagesUnit 2 EnzymeamrhkmhNo ratings yet
- APB Risk & Safety - COVID-19 Resources 16102020Document13 pagesAPB Risk & Safety - COVID-19 Resources 16102020Adam BarnesNo ratings yet
- C40-203 c40-203 Dalmau SyllabiDocument8 pagesC40-203 c40-203 Dalmau SyllabiserftyNo ratings yet
- The Pharmaceutical, Insecticidal and Antioxidant Properties of GingerDocument5 pagesThe Pharmaceutical, Insecticidal and Antioxidant Properties of GingerWenalyn BelloNo ratings yet
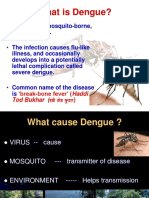
- Dengue PreventionDocument30 pagesDengue PreventionJaneshaNo ratings yet
- Research Essay Final Draft 1Document10 pagesResearch Essay Final Draft 1api-548724051No ratings yet
- Resiliencia: Pautas para FortalecerlaDocument50 pagesResiliencia: Pautas para Fortalecerlaluci saenzNo ratings yet
- Health Problems Common in PRESCHOOLDocument15 pagesHealth Problems Common in PRESCHOOLJanelle Lois EscolanoNo ratings yet
- Name: Olusegun-Obiwusi, Olufunke DATE: - : Subjective: DXDocument4 pagesName: Olusegun-Obiwusi, Olufunke DATE: - : Subjective: DXGrape JuiceNo ratings yet
- Covid 19 Associated Fungal InfectionsDocument14 pagesCovid 19 Associated Fungal InfectionsKarla SuheiNo ratings yet
- Gas Exchange 1 QPDocument11 pagesGas Exchange 1 QPokguserfucker idontgiveashitNo ratings yet
- Principles of Eye Management in Stevens-Johnson Syndrome: Mittanamalli S. SridharDocument5 pagesPrinciples of Eye Management in Stevens-Johnson Syndrome: Mittanamalli S. SridharFarah RNo ratings yet
- Medical Economics Magazine PDFDocument41 pagesMedical Economics Magazine PDFxtineNo ratings yet
- NCM 116 Lect PLP Assessmenteye Disorders IntroductionDocument35 pagesNCM 116 Lect PLP Assessmenteye Disorders IntroductionMariano Marbella100% (1)
- Drug Allergy by Alison ThorpeDocument13 pagesDrug Allergy by Alison ThorpeAlison ThorpeNo ratings yet
- Contractures WPS OfficeDocument14 pagesContractures WPS OfficeMiss KayaniNo ratings yet
- Internship EssayDocument2 pagesInternship EssayMohsinNo ratings yet
- Adrenal Gland DisordersDocument5 pagesAdrenal Gland Disordersdujana rastanawiNo ratings yet
- Ercp - PDFDocument1 pageErcp - PDFAhmad Harissul IbadNo ratings yet
- World First Triple Peptide Japanese Scientific BreakthroughDocument6 pagesWorld First Triple Peptide Japanese Scientific BreakthroughHalter Michael KareniNo ratings yet
- Maeshima y Osawa - 2007 - Stroke Rehabilitation in A Patient With CerebellarDocument8 pagesMaeshima y Osawa - 2007 - Stroke Rehabilitation in A Patient With CerebellarJEREMY RANo ratings yet
- Escivex 10 2Document1 pageEscivex 10 2Havier EsparagueraNo ratings yet
- Severe MalariaDocument52 pagesSevere MalariaEnoch OseiNo ratings yet
- Research Methodology For Business - Healthy LifestyleDocument9 pagesResearch Methodology For Business - Healthy LifestyleRameshwar FundipalleNo ratings yet
- CASTISIMO - Section12 - Final Term Worksheet No. 3 PDFDocument2 pagesCASTISIMO - Section12 - Final Term Worksheet No. 3 PDFcharles lacson castisimoNo ratings yet
- Chapter 54 - Pathogenesis of OsteochondrosisDocument9 pagesChapter 54 - Pathogenesis of OsteochondrosisRam RamNo ratings yet
- FYP - Research ProposalDocument23 pagesFYP - Research Proposalfiz effaNo ratings yet
- Family Nursing Care PlanDocument66 pagesFamily Nursing Care PlanLina Michelle Matheson BrualNo ratings yet
- Child Obesity in SportsDocument10 pagesChild Obesity in SportsSamuel BusuttilNo ratings yet
- Chloramphenicol Treatment For Acute Infective Conjunctivitis in Children in Primary Care: A Randomised Double-Blind Placebo-Controlled TrialDocument8 pagesChloramphenicol Treatment For Acute Infective Conjunctivitis in Children in Primary Care: A Randomised Double-Blind Placebo-Controlled TrialFemi OdeNo ratings yet
- Jospt 2019 8309Document11 pagesJospt 2019 8309VizaNo ratings yet