You might also like
- Diminished Ovarian Reserve and Assisted Reproductive Technologies: Current Research and Clinical ManagementFrom EverandDiminished Ovarian Reserve and Assisted Reproductive Technologies: Current Research and Clinical ManagementOrhan BukulmezNo ratings yet
- Pi Is 0002937818302497Document8 pagesPi Is 0002937818302497Jody AndreanNo ratings yet
- The Natural Estrogen Diet and Recipe Book: Delicious Recipes for a Healthy LifestyleFrom EverandThe Natural Estrogen Diet and Recipe Book: Delicious Recipes for a Healthy LifestyleNo ratings yet
- Cervical RipeningDocument7 pagesCervical RipeningBagus WicaksonoNo ratings yet
- Impact of Polycystic Ovary, Metabolic Syndrome and Obesity on Women Health: Volume 8: Frontiers in Gynecological EndocrinologyFrom EverandImpact of Polycystic Ovary, Metabolic Syndrome and Obesity on Women Health: Volume 8: Frontiers in Gynecological EndocrinologyNo ratings yet
- Facchinetti 2005Document5 pagesFacchinetti 2005Sri HariNo ratings yet
- Induction of Labor With Misoprostol For Premature Rupture of Membranes Beyond Thirty-Six Weeks' GestationDocument6 pagesInduction of Labor With Misoprostol For Premature Rupture of Membranes Beyond Thirty-Six Weeks' GestationFebrinata MahadikaNo ratings yet
- Review: Expert Committee Member MISOPROSTOL (Low Dose For Labour Induction at Term) Author: Lenita WannmacherDocument13 pagesReview: Expert Committee Member MISOPROSTOL (Low Dose For Labour Induction at Term) Author: Lenita WannmacherTri YuliasihNo ratings yet
- Jurnal 2 MisoprostolDocument17 pagesJurnal 2 MisoprostolaldoNo ratings yet
- A Study Comparing Vaginal Misoprostol Alone With VDocument4 pagesA Study Comparing Vaginal Misoprostol Alone With VKamal AnshariNo ratings yet
- Safety and Efficacy of Misoprostol in Induction of Labour in Prelabour Rupture of Fetal Membrane in Nigerian Women: A Multicenter StudyDocument6 pagesSafety and Efficacy of Misoprostol in Induction of Labour in Prelabour Rupture of Fetal Membrane in Nigerian Women: A Multicenter StudyAnonymous GssdN5No ratings yet
- Effect of Delayed Misoprostol Dosing Interval For Induction of Labor: A Retrospective StudyDocument5 pagesEffect of Delayed Misoprostol Dosing Interval For Induction of Labor: A Retrospective StudyenggarNo ratings yet
- Thesis PaperDocument5 pagesThesis PaperbhalNo ratings yet
- Harmancrowell2019 1Document6 pagesHarmancrowell2019 1enggarNo ratings yet
- ComparisonDocument7 pagesComparisonpurnoor abidNo ratings yet
- W 3 e WDDocument6 pagesW 3 e WDsupaidi97No ratings yet
- 4037 14447 2 PBDocument5 pages4037 14447 2 PBleslin rajNo ratings yet
- Ruptur Cervix - DR ArifDocument23 pagesRuptur Cervix - DR ArifHans Natanael PosoNo ratings yet
- Effect of Delayed Misoprostol Dosing Interval For Induction of LaborDocument4 pagesEffect of Delayed Misoprostol Dosing Interval For Induction of LaborMicah Salapio BasisterNo ratings yet
- Journal Reading: Advisor: Dr. Ariawan Ditya, SP - OG Arranged byDocument18 pagesJournal Reading: Advisor: Dr. Ariawan Ditya, SP - OG Arranged bydesti cahyantiNo ratings yet
- Ijpr 13 299Document6 pagesIjpr 13 299Iene Dhiitta PramudNo ratings yet
- Early Amniotomy After Vaginal Misoprostol For Induction of Labor: A Randomized Clinical TrialDocument5 pagesEarly Amniotomy After Vaginal Misoprostol For Induction of Labor: A Randomized Clinical Trialbidan22No ratings yet
- Synopsis For Foley Plus Miso Vs Miso Alone in Induction of LabourDocument5 pagesSynopsis For Foley Plus Miso Vs Miso Alone in Induction of LabourAshish TomarNo ratings yet
- Misoprostol For Induction of Labor With A Live FetusDocument4 pagesMisoprostol For Induction of Labor With A Live FetusUlfaa MutiaaNo ratings yet
- Clinical Uses of Misoprostol in Obstetrics and Gynaecology: MedicalDocument4 pagesClinical Uses of Misoprostol in Obstetrics and Gynaecology: MedicalRobertus HajaiNo ratings yet
- MisoprostolDocument6 pagesMisoprostolMaría PradoNo ratings yet
- Misoprostol Vaginal Insert and Time To Vaginal.4Document9 pagesMisoprostol Vaginal Insert and Time To Vaginal.4Afiqah So JasmiNo ratings yet
- Comparison Between Vaginal and Sublingual Misoprostol 50 UgDocument6 pagesComparison Between Vaginal and Sublingual Misoprostol 50 Ugidris setyadi lubisNo ratings yet
- Suppression of Puerperal Lactation Using Jasmine Flowers (Jasminum Sambac)Document4 pagesSuppression of Puerperal Lactation Using Jasmine Flowers (Jasminum Sambac)Iara PachêcoNo ratings yet
- A RCT of Foley Bulb For Labor Induction in PROMDocument7 pagesA RCT of Foley Bulb For Labor Induction in PROMNailul RosyidaNo ratings yet
- A Randomized Trial of Synthetic Osmotic Cervical D - 2022 - American Journal ofDocument20 pagesA Randomized Trial of Synthetic Osmotic Cervical D - 2022 - American Journal ofLuis GómezNo ratings yet
- Partus LamaDocument4 pagesPartus LamaIntan PermataNo ratings yet
- MisoprostolDocument6 pagesMisoprostolmichelle1945No ratings yet
- p2123 PDFDocument6 pagesp2123 PDFwe sagara dewiNo ratings yet
- International Journal of Gynecology and ObstetricsDocument6 pagesInternational Journal of Gynecology and ObstetricsmerawatidyahsepitaNo ratings yet
- Comparison of Two DosesDocument7 pagesComparison of Two DosesFelix BoamahNo ratings yet
- Chen 2015Document9 pagesChen 2015noor hyNo ratings yet
- Made Ayu AsnggrainiDocument5 pagesMade Ayu AsnggrainiMoh RamliNo ratings yet
- Comparison of Vaginal and Oral Doses of Misoprostol For Labour Induction in Post-Term PregnanciesDocument4 pagesComparison of Vaginal and Oral Doses of Misoprostol For Labour Induction in Post-Term Pregnanciesnur ulfahNo ratings yet
- INDUKSIDocument17 pagesINDUKSIKukuh PrasetyoNo ratings yet
- ACOG 2009 Induction of LaborDocument12 pagesACOG 2009 Induction of LaborRiantiara PutrizaNo ratings yet
- Alfirevic Et Al-2014-Cochrane Database of Systematic Reviews - Sup-1Document4 pagesAlfirevic Et Al-2014-Cochrane Database of Systematic Reviews - Sup-1Ulfaa MutiaaNo ratings yet
- Aborto Manejo Medico Primer Trimestre ACOG'14Document18 pagesAborto Manejo Medico Primer Trimestre ACOG'14CIRUGIA GENERAL HRAEZNo ratings yet
- Misoprostol SL Vs VAGDocument5 pagesMisoprostol SL Vs VAGAgus WijayaNo ratings yet
- Antenatal Betamethasone For WomenDocument10 pagesAntenatal Betamethasone For WomenMarcela Garzon O VelezNo ratings yet
- 10.1111@jog.13193 2 PDFDocument5 pages10.1111@jog.13193 2 PDFgandongmiziNo ratings yet
- Progesterone and The Risk of Preterm Birth Among Women With A Short CervixDocument8 pagesProgesterone and The Risk of Preterm Birth Among Women With A Short Cervixangela_karenina_1No ratings yet
- Oxytocin Use in Labor: Legal ImplicationsDocument9 pagesOxytocin Use in Labor: Legal ImplicationsGustavo flores quispeNo ratings yet
- Acog Practice Bulletin No 107 Induction of Labor 2009Document12 pagesAcog Practice Bulletin No 107 Induction of Labor 2009Esme Tecuanhuehue PaulinoNo ratings yet
- Can Serum Progesterone Concentration Direct A FresDocument7 pagesCan Serum Progesterone Concentration Direct A FresashrafmogyNo ratings yet
- Can Serum Progesterone Concentration Direct A FresDocument8 pagesCan Serum Progesterone Concentration Direct A FresashrafmogyNo ratings yet
- Treatment With Piroxicam Before Embryo Transfer Increases The Pregnancy Rate After in Vitro Fertilization and Embryo TransferDocument5 pagesTreatment With Piroxicam Before Embryo Transfer Increases The Pregnancy Rate After in Vitro Fertilization and Embryo TransferVasantham HospitalNo ratings yet
- Ajacm 2009 4 (1) Acup Improve EndometrDocument7 pagesAjacm 2009 4 (1) Acup Improve EndometrdirkvandeweyerNo ratings yet
- The Effect of Hyoscine Butylbromide On The First Stage of Labour in Term PregnanciesDocument5 pagesThe Effect of Hyoscine Butylbromide On The First Stage of Labour in Term PregnanciesnephylymNo ratings yet
- Randomized Clinical Trial Between Hourly Titrated Oral Misoprostol and Vaginal Dinoprostone For Induction of LaborDocument6 pagesRandomized Clinical Trial Between Hourly Titrated Oral Misoprostol and Vaginal Dinoprostone For Induction of LabormerawatidyahsepitaNo ratings yet
- Induction and Augmentation of LaborDocument45 pagesInduction and Augmentation of LaborarongeremewNo ratings yet
- Prolonged LaborDocument8 pagesProlonged LaborMisnariahIdrusNo ratings yet
- Oxytocin MassaseDocument8 pagesOxytocin MassaseJery PradilaNo ratings yet
- Effect of Progestin Compared With Combined Oral.3Document9 pagesEffect of Progestin Compared With Combined Oral.3Dedi SaputraNo ratings yet
- Literarture ReviewDocument10 pagesLiterarture ReviewRiany Jade SabrinaNo ratings yet
- Complete Guide To Communication Problems After StrokeDocument22 pagesComplete Guide To Communication Problems After Strokeapi-215453798100% (1)
- Readers Digest Asia Feburary 2021Document134 pagesReaders Digest Asia Feburary 2021FURY FURIONNo ratings yet
- Rajiv Gandhi University of Health Sciences, Bangalore, KarnatakaDocument18 pagesRajiv Gandhi University of Health Sciences, Bangalore, KarnatakaprashantghodkeNo ratings yet
- DIY Mineral MakeupDocument1 pageDIY Mineral MakeupDirek JP NinalgaNo ratings yet
- BioassayDocument38 pagesBioassayMuhammad Masoom AkhtarNo ratings yet
- Uts Ganjil Bahasa Inggris Kelas 9Document11 pagesUts Ganjil Bahasa Inggris Kelas 9Ketua EE 2021 AndrianoNo ratings yet
- Minimizing The Risk of Alzheimer S DiseaseDocument328 pagesMinimizing The Risk of Alzheimer S DiseaseLuis Raudales100% (1)
- New Text DocumentDocument2 pagesNew Text DocumenteqweNo ratings yet
- Prevalence of High Risk Pregnancy in Rural DharwadDocument4 pagesPrevalence of High Risk Pregnancy in Rural DharwadIOSRjournalNo ratings yet
- The Peat WhispererDocument85 pagesThe Peat Whispererzarrin77100% (6)
- Levels of PreventionDocument23 pagesLevels of Preventionkuruvagadda sagar100% (1)
- Peduc 01 PATH-Fit (Physical Activities Towards Health and Fitness) First Semester - School Year 2021 - 2022Document11 pagesPeduc 01 PATH-Fit (Physical Activities Towards Health and Fitness) First Semester - School Year 2021 - 2022Grace BrigondoNo ratings yet
- Curriculum Vitae - Aditya Pratama PutraDocument3 pagesCurriculum Vitae - Aditya Pratama PutraIan SeptiantoNo ratings yet
- Dental Informatics PlusDocument1 pageDental Informatics PlusNagendra TyagiNo ratings yet
- Health and Wellbeing: AT WORK 2021Document37 pagesHealth and Wellbeing: AT WORK 2021Constantin CiacaruNo ratings yet
- Jonsen 4 Box MethodDocument5 pagesJonsen 4 Box MethodsawsanNo ratings yet
- Indian Research Funding AgenciesDocument6 pagesIndian Research Funding AgencieskcchtphdNo ratings yet
- Étude de La Prévalence Et de L'incidence Du Cancer de La Prostate Dans Le Nord Cameroun: Coût Et Prise en ChargeDocument8 pagesÉtude de La Prévalence Et de L'incidence Du Cancer de La Prostate Dans Le Nord Cameroun: Coût Et Prise en ChargeHerve KadaNo ratings yet
- Transdiagnostic TreatmentDocument9 pagesTransdiagnostic Treatmentvalentina chistrugaNo ratings yet
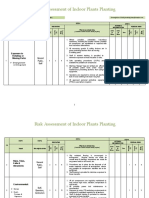
- Risk Assessment of Indoor Plants PlantingDocument5 pagesRisk Assessment of Indoor Plants Plantingطارق رضوانNo ratings yet
- ZR53 MSDSDocument5 pagesZR53 MSDSAnonymous PinM7iNo ratings yet
- Foundation of Professional Nursing PracticeDocument5 pagesFoundation of Professional Nursing PracticeIvan LouiseNo ratings yet
- Department of Education: Catherine B. Operaña, EddDocument5 pagesDepartment of Education: Catherine B. Operaña, EddMarica PangilinanNo ratings yet
- Q - A Random 8Document5 pagesQ - A Random 8Yuuki Chitose (tai-kun)No ratings yet
- Cannabis-Infused Food and Canadian Consumers' Willingness To Consider "Recreational" Cannabis As A Food IngredientDocument7 pagesCannabis-Infused Food and Canadian Consumers' Willingness To Consider "Recreational" Cannabis As A Food IngredientCTV CalgaryNo ratings yet
- MAPEH Activity Sheet Q2-Week1Document7 pagesMAPEH Activity Sheet Q2-Week1John King johnking.monderinNo ratings yet
- (Ebook) SuperBrain Yoga by Master Choa Kok Sui PDFDocument81 pages(Ebook) SuperBrain Yoga by Master Choa Kok Sui PDFBoonyarit Huang100% (5)
- Stacey Wilson-Web V-Sept 2014Document6 pagesStacey Wilson-Web V-Sept 2014api-247917310No ratings yet
- Microbial Limits Tests: The Difference Between "Absence of Objectionable Microorganisms" and "Absence of Specified Microorganisms"Document7 pagesMicrobial Limits Tests: The Difference Between "Absence of Objectionable Microorganisms" and "Absence of Specified Microorganisms"Jai MurugeshNo ratings yet
- What to Expect When You’re Expecting (5th Edition)From EverandWhat to Expect When You’re Expecting (5th Edition)Rating: 5 out of 5 stars5/5 (1)
- The Pain Gap: How Sexism and Racism in Healthcare Kill WomenFrom EverandThe Pain Gap: How Sexism and Racism in Healthcare Kill WomenRating: 4 out of 5 stars4/5 (153)
- The Menopause Manifesto: Own Your Health With Facts and FeminismFrom EverandThe Menopause Manifesto: Own Your Health With Facts and FeminismRating: 4 out of 5 stars4/5 (18)
- ADHD Women: A Holistic Approach To ADHD ManagementFrom EverandADHD Women: A Holistic Approach To ADHD ManagementRating: 5 out of 5 stars5/5 (4)
- All in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayFrom EverandAll in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayRating: 5 out of 5 stars5/5 (2)
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeFrom EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeRating: 3.5 out of 5 stars3.5/5 (13)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisFrom EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisRating: 3 out of 5 stars3/5 (2)
- Healing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeFrom EverandHealing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeNo ratings yet
- Brain Body Diet: 40 Days to a Lean, Calm, Energized, and Happy SelfFrom EverandBrain Body Diet: 40 Days to a Lean, Calm, Energized, and Happy SelfRating: 5 out of 5 stars5/5 (2)
- Labor with Hope: Gospel Meditations on Pregnancy, Childbirth, and MotherhoodFrom EverandLabor with Hope: Gospel Meditations on Pregnancy, Childbirth, and MotherhoodRating: 4.5 out of 5 stars4.5/5 (28)
- The Path of the Priestess: A Guidebook for Awakening the Divine FeminineFrom EverandThe Path of the Priestess: A Guidebook for Awakening the Divine FeminineRating: 4 out of 5 stars4/5 (2)
- What No One Tells You: A Guide to Your Emotions from Pregnancy to MotherhoodFrom EverandWhat No One Tells You: A Guide to Your Emotions from Pregnancy to MotherhoodRating: 4.5 out of 5 stars4.5/5 (30)
- Younger Next Year, 2nd Edition: Live Strong, Fit, Sexy, and Smart-Until You're 80 and BeyondFrom EverandYounger Next Year, 2nd Edition: Live Strong, Fit, Sexy, and Smart-Until You're 80 and BeyondRating: 4 out of 5 stars4/5 (110)
- Breaking Free from Body Shame: Dare to Reclaim What God Has Named GoodFrom EverandBreaking Free from Body Shame: Dare to Reclaim What God Has Named GoodRating: 5 out of 5 stars5/5 (33)
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouFrom EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouNo ratings yet
- I'll Start Again Monday: Break the Cycle of Unhealthy Eating Habits with Lasting Spiritual SatisfactionFrom EverandI'll Start Again Monday: Break the Cycle of Unhealthy Eating Habits with Lasting Spiritual SatisfactionRating: 4.5 out of 5 stars4.5/5 (124)
- 9 Months Is Not Enough: The Ultimate Pre-Pregnancy Checklist to Create a Baby-Ready Body and Build Generational HealthFrom Everand9 Months Is Not Enough: The Ultimate Pre-Pregnancy Checklist to Create a Baby-Ready Body and Build Generational HealthNo ratings yet
- Bumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondFrom EverandBumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondRating: 4.5 out of 5 stars4.5/5 (38)
- Period Power: Harness Your Hormones and Get Your Cycle Working For YouFrom EverandPeriod Power: Harness Your Hormones and Get Your Cycle Working For YouRating: 4 out of 5 stars4/5 (25)
- Sacred Womb Healing Meditation Divine feminine alignment: heal ancestral traumas deep wounds, release blocked sexual energies, flow to creativity, overcome the energies of birthing, joy love happyFrom EverandSacred Womb Healing Meditation Divine feminine alignment: heal ancestral traumas deep wounds, release blocked sexual energies, flow to creativity, overcome the energies of birthing, joy love happyRating: 5 out of 5 stars5/5 (1)
- Spirit Baby: Communicate with Your Unborn Baby. Ease Your BirthFrom EverandSpirit Baby: Communicate with Your Unborn Baby. Ease Your BirthRating: 5 out of 5 stars5/5 (1)
- I'm So Effing Hungry: Why We Crave What We Crave – and What to Do About ItFrom EverandI'm So Effing Hungry: Why We Crave What We Crave – and What to Do About ItNo ratings yet
- Call of the Wild: How We Heal Trauma, Awaken Our Own Power, and Use It For GoodFrom EverandCall of the Wild: How We Heal Trauma, Awaken Our Own Power, and Use It For GoodNo ratings yet
- The Better Period Food Solution: Eat Your Way to a Lifetime of Healthier CyclesFrom EverandThe Better Period Food Solution: Eat Your Way to a Lifetime of Healthier CyclesNo ratings yet
- The First Forty Days: The Essential Art of Nourishing the New MotherFrom EverandThe First Forty Days: The Essential Art of Nourishing the New MotherRating: 5 out of 5 stars5/5 (5)
- A Radical Guide for Women with ADHD: Embrace Neurodiversity, Live Boldly, and Break Through BarriersFrom EverandA Radical Guide for Women with ADHD: Embrace Neurodiversity, Live Boldly, and Break Through BarriersRating: 4.5 out of 5 stars4.5/5 (71)