You might also like
- Fiches AnatomyDocument6 pagesFiches AnatomyAnas Ismail100% (2)
- Anatomy of The Senses QuickStudy Reference Guide - (HEARING)Document2 pagesAnatomy of The Senses QuickStudy Reference Guide - (HEARING)statsoNo ratings yet
- Poisoning of Mankind - The Fallacy of Blood Types & Copper DeficiencyDocument7 pagesPoisoning of Mankind - The Fallacy of Blood Types & Copper DeficiencyAlvin L. Rozier100% (3)
- Trunk Wall: Muscle Charts: Cheat Sheet (English Terminology)Document13 pagesTrunk Wall: Muscle Charts: Cheat Sheet (English Terminology)Galo Pillajo100% (4)
- Poster1 Arrhythmia Recognition e PDFDocument1 pagePoster1 Arrhythmia Recognition e PDFSergio ChangNo ratings yet
- Trunk WallDocument13 pagesTrunk WallMetin Hakkan100% (1)
- Chapter 8 Lab Assignment - Appendicular Skeleton LabelingDocument6 pagesChapter 8 Lab Assignment - Appendicular Skeleton Labelingadriana blanco galianoNo ratings yet
- HIIT Academy Total Body Blast Phase 1 PDFDocument33 pagesHIIT Academy Total Body Blast Phase 1 PDFAndre ChinassoNo ratings yet
- Fractures NoteDocument31 pagesFractures NoteNoor AlblushiNo ratings yet
- Pictorial Atlas of Botulinum Toxin Injection: Dosage Localization ApplicationDocument26 pagesPictorial Atlas of Botulinum Toxin Injection: Dosage Localization ApplicationВаня Немеш100% (1)
- Admission FormDocument4 pagesAdmission FormbharatkumarpadhiNo ratings yet
- Canine Impaction Final PDFDocument136 pagesCanine Impaction Final PDFDr. ShantanuNo ratings yet
- Grief & Loss - pptx-1Document66 pagesGrief & Loss - pptx-1pinkyNo ratings yet
- SpellbindingDocument45 pagesSpellbindingAnuja WairagadeNo ratings yet
- Historical Developments of Community Health Nursing in The WorldDocument75 pagesHistorical Developments of Community Health Nursing in The Worldsoniya naik0% (1)
- Some Answers For ANATOMY RGHUSDocument4 pagesSome Answers For ANATOMY RGHUSIsha RaghuNo ratings yet
- Posterio Approach Subaxial Cervical Spine + Anterior Approach Cervical Spine +aplied Surgical AnatomyDocument28 pagesPosterio Approach Subaxial Cervical Spine + Anterior Approach Cervical Spine +aplied Surgical AnatomywidapnNo ratings yet
- Poster02 Skeletal-System-Posterior Ledger11x17Document1 pagePoster02 Skeletal-System-Posterior Ledger11x17jeffrin alexanderNo ratings yet
- 75631-Anatomy of The Intracranial Vessels and Vascular Territories - JagerDocument10 pages75631-Anatomy of The Intracranial Vessels and Vascular Territories - JagernurlanNo ratings yet
- Activity 1 Anatomical TermsDocument3 pagesActivity 1 Anatomical TermsJerico YoNo ratings yet
- 張凱閔醫 花蓮2023!04!16Shoulder InjectionDocument9 pages張凱閔醫 花蓮2023!04!16Shoulder InjectiontsungyuchiNo ratings yet
- LAB-Manual UpperLimb8 DistalForearmDocument25 pagesLAB-Manual UpperLimb8 DistalForearmivanNo ratings yet
- Anatomy and Physiolology Laboratory ManualDocument7 pagesAnatomy and Physiolology Laboratory ManualJan Edward Abarientos MandaniNo ratings yet
- Chapter 4Document90 pagesChapter 4danieldamite09No ratings yet
- Brachial PlexusDocument7 pagesBrachial PlexusNur NajminaNo ratings yet
- Branches of Axillary ArteryDocument2 pagesBranches of Axillary Arterydivyanshu ranjanNo ratings yet
- Cervicofacial Flaps For Head and Neck ReconstructionDocument15 pagesCervicofacial Flaps For Head and Neck Reconstructionfabian hernandez medinaNo ratings yet
- 5 PDFDocument10 pages5 PDFBarbero JuanNo ratings yet
- Posterior BonesDocument1 pagePosterior BonesRheal P EsmailNo ratings yet
- Block Guru - Ankle: Saphenous Common PeronealDocument1 pageBlock Guru - Ankle: Saphenous Common PeronealCosmin RazvanNo ratings yet
- HerniaDocument13 pagesHerniarmt_01No ratings yet
- Lab 1 Anatomical Description Exs 397Document10 pagesLab 1 Anatomical Description Exs 397api-476937064No ratings yet
- Khalfan Alsh. - The Gluteal RegionDocument27 pagesKhalfan Alsh. - The Gluteal Regionsara fekriNo ratings yet
- Ulnar NerveDocument10 pagesUlnar NerveRiya GuptaNo ratings yet
- Anatomy of The Oculomotor (CN III), Trochlear (CN IV) and Abducens (CN VI) Nerves - OsmosisDocument4 pagesAnatomy of The Oculomotor (CN III), Trochlear (CN IV) and Abducens (CN VI) Nerves - Osmosismarkmuiruri581No ratings yet
- Brachial PlexusDocument61 pagesBrachial PlexusGutu Garemewu BiruNo ratings yet
- Bimbingan DR Mira 4Document4 pagesBimbingan DR Mira 4sean 102018039No ratings yet
- DR Agus Sistem Syaraf Spinal ChordDocument50 pagesDR Agus Sistem Syaraf Spinal ChordRifky Al ThariqNo ratings yet
- PG 0290Document1 pagePG 0290MihaelaNo ratings yet
- Winslow PathwayDocument3 pagesWinslow PathwayMia MadalinaNo ratings yet
- The Temporomandibular Joints, Teeth, and Muscles, and Their FunctionsDocument16 pagesThe Temporomandibular Joints, Teeth, and Muscles, and Their Functionsfalop41797No ratings yet
- معمل upper limb د علي البغدادي الجزء الاولDocument8 pagesمعمل upper limb د علي البغدادي الجزء الاولAbdulaziz MohammedNo ratings yet
- My Fracture NotesDocument20 pagesMy Fracture NotesZai AkmaNo ratings yet
- "Components Separation" Method For Closure of Abdominal-Wall Defects: An Anatomic and Clinical StudyDocument8 pages"Components Separation" Method For Closure of Abdominal-Wall Defects: An Anatomic and Clinical StudyAndric Perez-OrtizNo ratings yet
- Orthomerica Scoli FormDocument1 pageOrthomerica Scoli FormphenixousNo ratings yet
- Chapter 2. Anterior Thoracic WallDocument14 pagesChapter 2. Anterior Thoracic Wallleafyislucky 91No ratings yet
- Resumão, Resumo, Articulações e Ligamentos, Anatomia - Passei DiretoDocument3 pagesResumão, Resumo, Articulações e Ligamentos, Anatomia - Passei DiretoPablo FranzoniNo ratings yet
- VertigoDocument84 pagesVertigoartika mayandaNo ratings yet
- Lower Extremity - Muscle Summary ChartDocument10 pagesLower Extremity - Muscle Summary ChartpoggerNo ratings yet
- 4250 Lec7 15Document8 pages4250 Lec7 15Carlos Enrique Pijo PerezNo ratings yet
- Tibia 2018Document12 pagesTibia 2018Diego MendozaNo ratings yet
- 7-9 Skull From Behind (Norma Occipitalis)Document1 page7-9 Skull From Behind (Norma Occipitalis)Zohaib Ur RahmanNo ratings yet
- Spinal CordDocument82 pagesSpinal CordAfifah Nur KartikasariNo ratings yet
- Kin2222 - Ankle + Foot-1Document27 pagesKin2222 - Ankle + Foot-1AmreenNo ratings yet
- Upper Extremity AnatomyDocument1 pageUpper Extremity AnatomyKristineNo ratings yet
- Injuries of Extracranial, Cranial, Volpe2018Document36 pagesInjuries of Extracranial, Cranial, Volpe2018hermalina sabruNo ratings yet
- Cat AtlasDocument1 pageCat AtlasMitchNo ratings yet
- AnesthesiaDocument24 pagesAnesthesialittle wordsNo ratings yet
- Surgical Approaches To JointsDocument39 pagesSurgical Approaches To JointsJD46No ratings yet
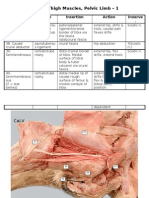
- Muscles-Pelvic Limb 1-Caudal ThighDocument2 pagesMuscles-Pelvic Limb 1-Caudal ThighR1pTid3No ratings yet
- The Shouldice Repair: Robert Bendavid, MDDocument14 pagesThe Shouldice Repair: Robert Bendavid, MDmarquete72No ratings yet
- Iqx-Ft-003 Format For Surgical Planning March 15 2024Document14 pagesIqx-Ft-003 Format For Surgical Planning March 15 2024api-725651063No ratings yet
- Aircraft Structures-II - U1 - L1 - T2 - Problems On Direct Stress Distribution For Symmetrical Bending of BeamsDocument9 pagesAircraft Structures-II - U1 - L1 - T2 - Problems On Direct Stress Distribution For Symmetrical Bending of Beamssarathkumar sebastinNo ratings yet
- Complete SpottersDocument229 pagesComplete Spottersakg200804No ratings yet
- Visual Functional Neuroanatomy Map: © 2000, Dennis P. Swiercinsky, PH.DDocument1 pageVisual Functional Neuroanatomy Map: © 2000, Dennis P. Swiercinsky, PH.DCristi BorceaNo ratings yet
- Bedside Placement of Inferior Vena Cava Filter: David P. Blake and L.D. BrittDocument9 pagesBedside Placement of Inferior Vena Cava Filter: David P. Blake and L.D. BrittandiNo ratings yet
- Core Muscle Injuries (Athletic Pubalgia, Sports Hernia) : PathophysiologyDocument5 pagesCore Muscle Injuries (Athletic Pubalgia, Sports Hernia) : PathophysiologyandiNo ratings yet
- Role of Cardiovascular Imaging For The Diagnosis and Prognosis of Cardiac AmyloidosisDocument7 pagesRole of Cardiovascular Imaging For The Diagnosis and Prognosis of Cardiac AmyloidosisandiNo ratings yet
- Slides 01 CellularAging AgingDocument32 pagesSlides 01 CellularAging AgingandiNo ratings yet
- Mdy 148Document15 pagesMdy 148andiNo ratings yet
- Abdominal Wall Reconstruction: AnatomyDocument6 pagesAbdominal Wall Reconstruction: AnatomyandiNo ratings yet
- Piis1473309918303451 PDFDocument11 pagesPiis1473309918303451 PDFandiNo ratings yet
- Circulationaha 118 034722 PDFDocument10 pagesCirculationaha 118 034722 PDFandiNo ratings yet
- 10 5694mja18 00647 PDFDocument7 pages10 5694mja18 00647 PDFandiNo ratings yet
- KCJ 48 565 PDFDocument26 pagesKCJ 48 565 PDFandiNo ratings yet
- 10 5694mja18 00647 PDFDocument7 pages10 5694mja18 00647 PDFandiNo ratings yet
- Prospective Randomized Evaluation of Preoperative Angiotensin-Converting Enzyme Inhibition (PREOP-ACEI)Document7 pagesProspective Randomized Evaluation of Preoperative Angiotensin-Converting Enzyme Inhibition (PREOP-ACEI)andiNo ratings yet
- Mdy 148Document15 pagesMdy 148andiNo ratings yet
- Machine Learning of Toxicological Big Data Enables Read-Across Structure Activity Relationships (RASAR) Outperforming Animal Test ReproducibilityDocument15 pagesMachine Learning of Toxicological Big Data Enables Read-Across Structure Activity Relationships (RASAR) Outperforming Animal Test ReproducibilityGina SmithNo ratings yet
- 10 5694mja18 00647 PDFDocument7 pages10 5694mja18 00647 PDFandiNo ratings yet
- Tuberculosis Latente en Adultos: 9 Meses de Isoniazida vs. 4 Meses de RifampicinaDocument14 pagesTuberculosis Latente en Adultos: 9 Meses de Isoniazida vs. 4 Meses de RifampicinaSMIBA MedicinaNo ratings yet
- Auscultation For Bowel Sounds in Patients With Ileus: An Outdated Practice in The ICU?Document5 pagesAuscultation For Bowel Sounds in Patients With Ileus: An Outdated Practice in The ICU?andiNo ratings yet
- The American Association For Thoracic Surgery Consensus Guidelines On Bicuspid Aortic Valve-Related Aortopathy: Executive SummaryDocument8 pagesThe American Association For Thoracic Surgery Consensus Guidelines On Bicuspid Aortic Valve-Related Aortopathy: Executive SummaryandiNo ratings yet
- Management of Cancer Pain in Adult Patients: ESMO Clinical Practice GuidelinesDocument26 pagesManagement of Cancer Pain in Adult Patients: ESMO Clinical Practice GuidelinesandiNo ratings yet
- Circulationaha 118 034722 PDFDocument10 pagesCirculationaha 118 034722 PDFandiNo ratings yet
- Timing of Intervention in Aortic Stenosis: A Review of Current and Future StrategiesDocument11 pagesTiming of Intervention in Aortic Stenosis: A Review of Current and Future StrategiesandiNo ratings yet
- Gout Guide: Lifelong Transformation, One Healthy Habit at A Time®Document9 pagesGout Guide: Lifelong Transformation, One Healthy Habit at A Time®Rocco McWhitebeardNo ratings yet
- Genetic Testing For Autism, Explained: Spectrum - Autism Research NewsDocument3 pagesGenetic Testing For Autism, Explained: Spectrum - Autism Research NewsTimothyNo ratings yet
- MSDS-Irganox 1010Document10 pagesMSDS-Irganox 1010Seshagiri KalyanasundaramNo ratings yet
- Anaphylaxis - 2Document8 pagesAnaphylaxis - 2Ronald WiradirnataNo ratings yet
- Chapter 1 AnswersDocument3 pagesChapter 1 AnswersMarisa VetterNo ratings yet
- Bechara and Damasio, 2005Document37 pagesBechara and Damasio, 2005Sumer VaidNo ratings yet
- Gn-31 Qms Cad (Dec 2012) FinalDocument19 pagesGn-31 Qms Cad (Dec 2012) FinalSeanNo ratings yet
- 017-2013 - MR (MOA Kalahi Cidss)Document3 pages017-2013 - MR (MOA Kalahi Cidss)SbGuinobatanNo ratings yet
- Periodontal Probing and Techniques JCDocument58 pagesPeriodontal Probing and Techniques JCAbhay TandonNo ratings yet
- Ulvac Ulvoil r7Document5 pagesUlvac Ulvoil r7Hiskia Benindo PurbaNo ratings yet
- Raw Milk or Packaged Milk?Document2 pagesRaw Milk or Packaged Milk?Marriam TariqNo ratings yet
- The ConsulDocument4 pagesThe ConsulPrince Adesina HaastrupNo ratings yet
- VENTILATOR MEKANIK DeswitaDocument25 pagesVENTILATOR MEKANIK DeswitaDinda AndrifaNo ratings yet
- Chapter 6 Test Skeletal SystemDocument49 pagesChapter 6 Test Skeletal SystemAlexandra CampeanuNo ratings yet
- Topic 13Document23 pagesTopic 13hasvinNo ratings yet
- Woman Burned by Acid in Random Subway Attack Has 16th SurgeryDocument1 pageWoman Burned by Acid in Random Subway Attack Has 16th Surgeryed2870winNo ratings yet
- NFPA Codes & Standards - 10Document1 pageNFPA Codes & Standards - 10karpanaiNo ratings yet
- MAPEH Study NotesDocument5 pagesMAPEH Study NotesBithao DaisyNo ratings yet
- Ujian Akhir SekolahDocument7 pagesUjian Akhir SekolahAhmad andis ArifinNo ratings yet
- In-Vitro Anti-Inflammatory and Anti-Arthritic: Activity of N-Butanol Fraction From Telosma Pallida (Roxb) Craib LeafDocument7 pagesIn-Vitro Anti-Inflammatory and Anti-Arthritic: Activity of N-Butanol Fraction From Telosma Pallida (Roxb) Craib LeafPunitNo ratings yet
- Star Health and Allied Insurance Company Limited: Customer Information Sheet - Family Health Optima Insurance PlanDocument12 pagesStar Health and Allied Insurance Company Limited: Customer Information Sheet - Family Health Optima Insurance Plananiket goyalNo ratings yet
- How The Red Cross Raised Half A Billion Dollars For Haiti - and Built Six Homes - ProPublicaDocument15 pagesHow The Red Cross Raised Half A Billion Dollars For Haiti - and Built Six Homes - ProPublicaGina PistolNo ratings yet
- NHP Original 1985 PDFDocument4 pagesNHP Original 1985 PDFAndrei IordanNo ratings yet
- To The Philosophy of The Human Person: Quarter 1 - Module 4.2: Care For The EnvironmentDocument21 pagesTo The Philosophy of The Human Person: Quarter 1 - Module 4.2: Care For The EnvironmentDustin EsguerraNo ratings yet