You might also like
- Lab09 Therapy4 IronDeficiencyDocument5 pagesLab09 Therapy4 IronDeficiencyHayna Rose100% (1)
- Serial KillersDocument25 pagesSerial KillersCarrie Davis Dellinger100% (1)
- Metabolic Acidosis: General Patient InformationDocument4 pagesMetabolic Acidosis: General Patient InformationRisen Delos ReyesNo ratings yet
- Chapter 12 - Hypertension - Pass The Salt, Please Level IIDocument7 pagesChapter 12 - Hypertension - Pass The Salt, Please Level IIRichix K Yabe0% (1)
- The Process of PhlebotomyDocument102 pagesThe Process of PhlebotomyCatherine Merilleno100% (1)
- Case Presentation-1Document22 pagesCase Presentation-1srija vijjapuNo ratings yet
- Changing Light Bulbs SafelyDocument1 pageChanging Light Bulbs SafelyAshok Suresh100% (4)
- Pulmonary EmbolismDocument27 pagesPulmonary EmbolismEfren Ezekiel AlbiosNo ratings yet
- CASE PRESENTATION ON AnemiaDocument25 pagesCASE PRESENTATION ON AnemiaSafoora Rafeeq100% (2)
- Indian Goat Farm Project ReportDocument5 pagesIndian Goat Farm Project ReportTariq Shah71% (7)
- 第五組 Type 2 Diabetes Mellitus PDFDocument4 pages第五組 Type 2 Diabetes Mellitus PDFLi LizNo ratings yet
- India 2030 PDFDocument188 pagesIndia 2030 PDFGray HouserNo ratings yet
- A Case Study On Parkinsons DiseaseDocument42 pagesA Case Study On Parkinsons DiseaseMark Tristan AsuncionNo ratings yet
- Case Study On Transcardial RevascularizationDocument34 pagesCase Study On Transcardial RevascularizationAJ RAJANo ratings yet
- Adime PT 2Document8 pagesAdime PT 2api-357368000No ratings yet
- DLP Eng3 - q3 Cot 2 Giving Possible Solutions To A ProblemDocument6 pagesDLP Eng3 - q3 Cot 2 Giving Possible Solutions To A ProblemNardita Castro100% (1)
- Example Letter of Medical NecessityDocument4 pagesExample Letter of Medical Necessitystarlette.hara100% (1)
- Case Presentation On Depression: BY: Mirza Habeeb Pharm D-III Yr 15122D1007Document32 pagesCase Presentation On Depression: BY: Mirza Habeeb Pharm D-III Yr 15122D1007Habeeb0% (1)
- PharReview - Individual Learning Activity - CLINICAL LABORATORY TESTS APPLICATIONDocument10 pagesPharReview - Individual Learning Activity - CLINICAL LABORATORY TESTS APPLICATIONGamotkoto PharmacyNo ratings yet
- Chapter 12 - Hypertension - Lost Shaker of Salt Level IIDocument6 pagesChapter 12 - Hypertension - Lost Shaker of Salt Level IIleensaeed26No ratings yet
- Shared RX Modules For FinalsDocument11 pagesShared RX Modules For FinalsOdyNo ratings yet
- Assignment - HypertensionDocument6 pagesAssignment - HypertensionAyessa Salazar100% (2)
- Recitation Final 2022Document11 pagesRecitation Final 2022api-662601291No ratings yet
- Dr. Vincent Morning Report SummaryDocument25 pagesDr. Vincent Morning Report SummaryPHOENIX LUNANo ratings yet
- HyperDocument21 pagesHyperayamalkawi204No ratings yet
- Diabetes Case Study: Goals and Treatment PlanDocument3 pagesDiabetes Case Study: Goals and Treatment PlanRoxanne Nasingao100% (1)
- Gout and HyperuricemiaDocument8 pagesGout and Hyperuricemiaندى القلويNo ratings yet
- Recovered File 1Document11 pagesRecovered File 1the orgmeNo ratings yet
- Case Study On Acute Gastroenteritis and Acid Peptic-2Document15 pagesCase Study On Acute Gastroenteritis and Acid Peptic-2FHAMITHANo ratings yet
- Studi KasusDocument9 pagesStudi KasusWina YustisiaNo ratings yet
- Case Study # 1Document3 pagesCase Study # 1Kia MercadoNo ratings yet
- MburiDocument11 pagesMburirahmaNo ratings yet
- Type Ii Diabetes: Presented by Thomas Eipe Pharmd InternDocument31 pagesType Ii Diabetes: Presented by Thomas Eipe Pharmd InternThomas EipeNo ratings yet
- Creatinine Clearance: 58 Ml/min: Fasting Lipid ProfileDocument4 pagesCreatinine Clearance: 58 Ml/min: Fasting Lipid ProfileAnn DassNo ratings yet
- Case Presentation On TIA and IHDDocument14 pagesCase Presentation On TIA and IHDS SAI BALAJI IYERNo ratings yet
- Chapter 14 - Dyslipidemia - Afraid of Another Attack Level IIDocument6 pagesChapter 14 - Dyslipidemia - Afraid of Another Attack Level IIfarah amraneNo ratings yet
- Osteoporosis MergedDocument73 pagesOsteoporosis MergedrlpmanglicmotNo ratings yet
- Nursing Process 3Document10 pagesNursing Process 3Shubhra Sheoran100% (1)
- Cystic Fibrosis: Prepared By: Johanna PepitoDocument38 pagesCystic Fibrosis: Prepared By: Johanna PepitoDharrenceNo ratings yet
- Final Hypertesiion Case For Pharmacotherapycourse WorkDocument37 pagesFinal Hypertesiion Case For Pharmacotherapycourse WorkBhavatharini ArunNo ratings yet
- Case Presentation On CKD With HTNDocument17 pagesCase Presentation On CKD With HTNmanoj sNo ratings yet
- Morning Report: Wednesday, March 8 2017Document14 pagesMorning Report: Wednesday, March 8 2017Safitri NindyaNo ratings yet
- CASE STUDY-Fhamitha Saara.ADocument11 pagesCASE STUDY-Fhamitha Saara.AFHAMITHANo ratings yet
- Aki 1Document2 pagesAki 1May ZaiterNo ratings yet
- Case Studies Therapy 1Document9 pagesCase Studies Therapy 1WONDWOSSEN ALEMUNo ratings yet
- Askep CKD Bahasa InggrisDocument10 pagesAskep CKD Bahasa InggrisElisabeth PanjaitanNo ratings yet
- Case Presentation On:: Rheumatoid Arthritis With Newly Diagnoised Steroid Related DM With Systemic HypertensionDocument12 pagesCase Presentation On:: Rheumatoid Arthritis With Newly Diagnoised Steroid Related DM With Systemic HypertensionSamyuktaNo ratings yet
- Case 1Document3 pagesCase 1bl9nkverseNo ratings yet
- CASEDocument1 pageCASENurhaifa MocademaNo ratings yet
- A Case On HypertensionDocument31 pagesA Case On HypertensionMark Tristan AsuncionNo ratings yet
- 2017 Refeeding Syndrome A Case Report PDFDocument6 pages2017 Refeeding Syndrome A Case Report PDFManual de VacunaciónNo ratings yet
- Severe Pneumonia and Hyperglycemia Case ReportDocument16 pagesSevere Pneumonia and Hyperglycemia Case ReportWilujeng AnggrainiNo ratings yet
- Acfrogbrljfmls 12moh9g Xejuq8r Rvex-End2jznh-5pkfr7b6m2fqezl48rpy1sfxosstcb1h5bcgyhkyp0ykwz7qgz0m61cvrh7o Bfxu0wyxfblyh4m67kpjxl1zem4m3fdw4e-H012yimDocument2 pagesAcfrogbrljfmls 12moh9g Xejuq8r Rvex-End2jznh-5pkfr7b6m2fqezl48rpy1sfxosstcb1h5bcgyhkyp0ykwz7qgz0m61cvrh7o Bfxu0wyxfblyh4m67kpjxl1zem4m3fdw4e-H012yimJemy Tamaño MorongNo ratings yet
- Pharmacotherapeutics - I: Case Study On Anterior Wall Myocardial InfarctionDocument20 pagesPharmacotherapeutics - I: Case Study On Anterior Wall Myocardial InfarctionDr. Suba Senthil0% (1)
- Template Duty ReportDocument6 pagesTemplate Duty ReportJefri SusantoNo ratings yet
- Grupo 10 RevisadoDocument27 pagesGrupo 10 RevisadoRonald GarcíaNo ratings yet
- Clinical Case S2Document4 pagesClinical Case S2Christiam Nicolas Roman OrtizNo ratings yet
- Stroke by K. NusrithaDocument13 pagesStroke by K. NusrithaSai SharathNo ratings yet
- Mortality-conference-2022.03.24 FINAL (自動儲存)Document51 pagesMortality-conference-2022.03.24 FINAL (自動儲存)許誌元No ratings yet
- DiabetesHypertensionDocument24 pagesDiabetesHypertensionnurulNo ratings yet
- Type 2 Diabetes Mellitus and Metabolic SyndromeDocument20 pagesType 2 Diabetes Mellitus and Metabolic Syndromemaryjoy021924No ratings yet
- DK IPD 3 - Ogie AsitesDocument174 pagesDK IPD 3 - Ogie AsiteshariogieNo ratings yet
- Title: 1. Case Study 1 2. Case Study 2 3. Case Study 3 4. Case Study 4 5. Case Study 5 6. Case Study 6Document33 pagesTitle: 1. Case Study 1 2. Case Study 2 3. Case Study 3 4. Case Study 4 5. Case Study 5 6. Case Study 6drpraveendevarbhaviNo ratings yet
- Case StudyDocument19 pagesCase Studylakshitataneja1998No ratings yet
- UGIB FinalDocument35 pagesUGIB FinalChin Heng TohNo ratings yet
- Concept Map # (Insert Student Name Here)Document15 pagesConcept Map # (Insert Student Name Here)aplesgjskNo ratings yet
- Group 6: Neñeria, Sharla Marsh: Methanol PoisoningDocument3 pagesGroup 6: Neñeria, Sharla Marsh: Methanol PoisoningStephanie Guibone QuiaoNo ratings yet
- Group 6: Pagbilao, Meriel Maan: Benzene PoisoningDocument2 pagesGroup 6: Pagbilao, Meriel Maan: Benzene PoisoningStephanie Guibone QuiaoNo ratings yet
- COVID-19 test results reportDocument1 pageCOVID-19 test results reportStephanie Guibone QuiaoNo ratings yet
- QC Research CriticDocument4 pagesQC Research CriticStephanie Guibone QuiaoNo ratings yet
- Pcol Case 1 OnlyDocument12 pagesPcol Case 1 OnlyStephanie Guibone QuiaoNo ratings yet
- Rubrics For Case AnalysisDocument1 pageRubrics For Case AnalysisStephanie Guibone QuiaoNo ratings yet
- Case Analysis FormatDocument2 pagesCase Analysis FormatStephanie Guibone QuiaoNo ratings yet
- Case Analysis FormatDocument2 pagesCase Analysis FormatStephanie Guibone QuiaoNo ratings yet
- Program FlowDocument1 pageProgram FlowStephanie Guibone QuiaoNo ratings yet
- FormsDocument4 pagesFormsStephanie Guibone QuiaoNo ratings yet
- Reviewing Literature Learning Disability Fiction and The Social Work PerspectiveDocument13 pagesReviewing Literature Learning Disability Fiction and The Social Work Perspectiveauthor.avengingangelNo ratings yet
- Legalize ItDocument2 pagesLegalize Itaisar aisarNo ratings yet
- Introduction To Criminology: By: Catherine G. Acedo, RcrimDocument34 pagesIntroduction To Criminology: By: Catherine G. Acedo, RcrimJEEHAN DELA CRUZNo ratings yet
- Rajiv Gandhi University Thesis Topics PediatricsDocument6 pagesRajiv Gandhi University Thesis Topics PediatricsWriteMyBusinessPaperSingapore100% (2)
- ProteinDocument89 pagesProteinAki OtaniNo ratings yet
- Stiletto - Spring 2015Document24 pagesStiletto - Spring 2015TGI Justice ProjectNo ratings yet
- Week 4Document21 pagesWeek 4Zoila EscalonaNo ratings yet
- CareGroup Case Study QuestionsDocument1 pageCareGroup Case Study QuestionsEnrica Melissa PanjaitanNo ratings yet
- Ecological Systems Theory by Bronfenbrenner: Prepared By: Karen B. Reginaldo Jung PuertoDocument20 pagesEcological Systems Theory by Bronfenbrenner: Prepared By: Karen B. Reginaldo Jung Puertochristian ferrerNo ratings yet
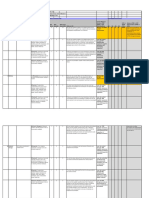
- PROCESS - Risk Assessment & HACCP Planning: Section 7.4.1Document4 pagesPROCESS - Risk Assessment & HACCP Planning: Section 7.4.1Wisnu samuel Atmaja triwarsitaNo ratings yet
- Broselow Pediatric Emergency TapeDocument13 pagesBroselow Pediatric Emergency TapePaulo KaleNo ratings yet
- Sociological Theories of Deviance: Definitions & ConsiderationsDocument10 pagesSociological Theories of Deviance: Definitions & ConsiderationsP TejeswariNo ratings yet
- Australian VSK 2018 LRDocument13 pagesAustralian VSK 2018 LRmuhamadrafie1975No ratings yet
- Nursing Leadership Roles ResponsibilitiesDocument2 pagesNursing Leadership Roles ResponsibilitiesDan Dan ManaoisNo ratings yet
- BT-740 OP Manual (740-ENG-OPM-EUR-R02) PDFDocument50 pagesBT-740 OP Manual (740-ENG-OPM-EUR-R02) PDFJaneth Pariona SedanNo ratings yet
- List of Allianz Efu Network (Panel) Hospitals: Hospital Name Address Telephone # KarachiDocument6 pagesList of Allianz Efu Network (Panel) Hospitals: Hospital Name Address Telephone # KarachiFaizan BasitNo ratings yet
- DSP 15-12-23Document36 pagesDSP 15-12-23Fu'ad ParkhaniNo ratings yet
- Chapter 33 Health AssessmentDocument2 pagesChapter 33 Health AssessmentHanz RapadasNo ratings yet
- Explaining Medication To Patients: Ni Kadek Ary Susandi, S.S., M.App - LingDocument11 pagesExplaining Medication To Patients: Ni Kadek Ary Susandi, S.S., M.App - LingmirahayuuNo ratings yet
- Grand Rounds NirsevimabDocument30 pagesGrand Rounds Nirsevimabapi-648891519No ratings yet
- List of Visiting DoctorDocument3 pagesList of Visiting Doctordulal pramanickNo ratings yet
- Pengumuman Jadwal Rapid Test Antigen Gratis Bagi Peserta Ujian SKB CPNS Pemerintah Kota Pangkalpinang 2021Document16 pagesPengumuman Jadwal Rapid Test Antigen Gratis Bagi Peserta Ujian SKB CPNS Pemerintah Kota Pangkalpinang 2021Syahrul SalehNo ratings yet
- Vijaya Diagnostic HIV Test ReportDocument1 pageVijaya Diagnostic HIV Test Reportpasham bharat simha reddy100% (1)