You might also like
- Comp P2 22Document10 pagesComp P2 22chuasioklengNo ratings yet
- H2 Chemistry 9729 P3 - Section ADocument9 pagesH2 Chemistry 9729 P3 - Section AchuasioklengNo ratings yet
- 2020 JPJC H2 Chem Prelim Paper 4 QP - Final PDFDocument19 pages2020 JPJC H2 Chem Prelim Paper 4 QP - Final PDFchuasioklengNo ratings yet
- H2 Chem Prelim Paper 2Document28 pagesH2 Chem Prelim Paper 2chuasioklengNo ratings yet
- H2 Chemistry 9729 P3 - Section BDocument4 pagesH2 Chemistry 9729 P3 - Section BchuasioklengNo ratings yet
- E Lit 22 - 3Document7 pagesE Lit 22 - 3chuasioklengNo ratings yet
- E Lit 22 - 1Document9 pagesE Lit 22 - 1chuasioklengNo ratings yet
- Comp P1 22Document8 pagesComp P1 22chuasioklengNo ratings yet
- H2 Chem Prelim Paper 3Document40 pagesH2 Chem Prelim Paper 3chuasioklengNo ratings yet
- Paper 2 QNDocument19 pagesPaper 2 QNchuasioklengNo ratings yet
- 2020 ACJC Paper 4 Qns PDFDocument18 pages2020 ACJC Paper 4 Qns PDFchuasioklengNo ratings yet
- Catholic Junior College: Chemistry Higher 1Document9 pagesCatholic Junior College: Chemistry Higher 1chuasioklengNo ratings yet
- ASR 2020 J2Prelim H2Chem P4 QP PDFDocument20 pagesASR 2020 J2Prelim H2Chem P4 QP PDFchuasioklengNo ratings yet
- 2020 JC2 Prelim H2 Chemistry Paper 4 QP PDFDocument21 pages2020 JC2 Prelim H2 Chemistry Paper 4 QP PDFchuasioklengNo ratings yet
- Paper 1 QNDocument10 pagesPaper 1 QNchuasioklengNo ratings yet
- Paper 2 QNDocument19 pagesPaper 2 QNchuasioklengNo ratings yet
- Part 2Document2 pagesPart 2chuasioklengNo ratings yet
- The Chemistry of Food: Proposed Sabbatical Program For Hwa Chong Institution (Year 2)Document2 pagesThe Chemistry of Food: Proposed Sabbatical Program For Hwa Chong Institution (Year 2)chuasioklengNo ratings yet
- 1530 Specimen Paper & Mark Scheme PDFDocument100 pages1530 Specimen Paper & Mark Scheme PDFchuasioklengNo ratings yet
- A CHEM - 2007 - Paper - 2Document14 pagesA CHEM - 2007 - Paper - 2chuasioklengNo ratings yet
- Catholic Junior College: Chemistry Higher 1Document10 pagesCatholic Junior College: Chemistry Higher 1chuasioklengNo ratings yet
- The Chemistry of Food: Proposed Sabbatical Program For Hwa Chong Institution (Year 2)Document2 pagesThe Chemistry of Food: Proposed Sabbatical Program For Hwa Chong Institution (Year 2)chuasioklengNo ratings yet
- A CHEM - 2007 - Paper - 1Document12 pagesA CHEM - 2007 - Paper - 1chuasioklengNo ratings yet
- Experiment #14: Preparation of Banana Oil and Characterization Using IR SpectrosDocument8 pagesExperiment #14: Preparation of Banana Oil and Characterization Using IR SpectroschuasioklengNo ratings yet
- Adult 2244 & Ref - v1Document147 pagesAdult 2244 & Ref - v1chuasioklengNo ratings yet
- Catalogue of Equations - Edexcel Chemistry Syllabus A 1530Document13 pagesCatalogue of Equations - Edexcel Chemistry Syllabus A 1530chuasioklengNo ratings yet
- S Jc1 C: Chedule FOR HemistryDocument1 pageS Jc1 C: Chedule FOR HemistrychuasioklengNo ratings yet
- S Jc2 C: Chedule FOR HemistryDocument1 pageS Jc2 C: Chedule FOR HemistrychuasioklengNo ratings yet
- Commentaries - Historical BooksDocument3 pagesCommentaries - Historical BookschuasioklengNo ratings yet
- Hemistry Esources: Study GuidesDocument2 pagesHemistry Esources: Study GuideschuasioklengNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Computing Test StatisticDocument8 pagesComputing Test StatisticFranklin BenitezNo ratings yet
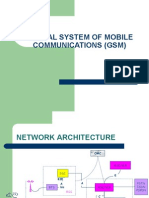
- GSMDocument38 pagesGSMapi-370641475% (8)
- Online Medical Delivery ServiceDocument10 pagesOnline Medical Delivery ServiceYESHUDAS JIVTODENo ratings yet
- Basics On Piping LayoutDocument11 pagesBasics On Piping Layoutpuru55980No ratings yet
- Ok - Las-Q2 Oral - Com W1Document5 pagesOk - Las-Q2 Oral - Com W1Ruben Rosendal De AsisNo ratings yet
- MA 105 TutorialsDocument29 pagesMA 105 TutorialsABHIJEET SHARMANo ratings yet
- Quality Assurance Measures For Procurement of Purchased PartsDocument26 pagesQuality Assurance Measures For Procurement of Purchased Partssakshi patilNo ratings yet
- Image PlacementDocument4 pagesImage PlacementJanix MagbanuaNo ratings yet
- Introducing The Open Banking StandardDocument12 pagesIntroducing The Open Banking StandardOpen Data Institute96% (25)
- CitiBank ApplicationDocument15 pagesCitiBank ApplicationJordan P HunterNo ratings yet
- Excel Charts and Graph TipsDocument6 pagesExcel Charts and Graph TipsKrystalNo ratings yet
- Session 7 - Beyond Tests - Alternatives in AssessmentDocument53 pagesSession 7 - Beyond Tests - Alternatives in AssessmenttrandinhgiabaoNo ratings yet
- Friday 11 January 2019: Health and Social CareDocument24 pagesFriday 11 January 2019: Health and Social CareAnette RodriguezNo ratings yet
- Principles of PaleontologyDocument10 pagesPrinciples of Paleontologyvitrinite50% (2)
- BAH Series 6000 Manguard - 113534-91Document40 pagesBAH Series 6000 Manguard - 113534-91AhmedNo ratings yet
- Change Pattern 1 To Pattern 2 by Moving Only Three Counters, Each Counter OnceDocument14 pagesChange Pattern 1 To Pattern 2 by Moving Only Three Counters, Each Counter OnceReshmiNo ratings yet
- SECTION 33 05 13 Manholes: Revised 03/2012Document52 pagesSECTION 33 05 13 Manholes: Revised 03/2012FAISAL NAZEERNo ratings yet
- Gas Cutting - by KiranDocument40 pagesGas Cutting - by KiransridharchebroluNo ratings yet
- TEST PearsonsDocument4 pagesTEST Pearsonsazertytyty000No ratings yet
- Republic of The Philippines Social Security System MemberDocument1 pageRepublic of The Philippines Social Security System MemberreyNo ratings yet
- Life Skills Preparation Form Grade 4Document20 pagesLife Skills Preparation Form Grade 4Ricardo DomingosNo ratings yet
- AccountingDocument45 pagesAccountingAfia ZaheenNo ratings yet
- Data Privacy Notice TemplateDocument1 pageData Privacy Notice TemplateangeloNo ratings yet
- Ian Robb a.M.I.struct.E. (Auth.) - Steel Frame Design Examples-Macmillan Education UK (1961)Document216 pagesIan Robb a.M.I.struct.E. (Auth.) - Steel Frame Design Examples-Macmillan Education UK (1961)GT100% (1)
- 2D1N Night Nueva VizcayaDocument3 pages2D1N Night Nueva VizcayaKaye RoldanNo ratings yet
- Rating and OTB RatingDocument7 pagesRating and OTB RatingpontathesmithjapanNo ratings yet
- Community-Based Eco Activity: An Out-of-School Youth Environment Education ProgramDocument10 pagesCommunity-Based Eco Activity: An Out-of-School Youth Environment Education ProgramInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Shadowfinder - Big Damn HeroesDocument30 pagesShadowfinder - Big Damn HeroesSteampunkObrimos100% (1)
- Lesson Plan - The V LanguageDocument4 pagesLesson Plan - The V LanguageLê Thị Ái NhiNo ratings yet
- Four Gears ModelDocument13 pagesFour Gears ModelPratik PatilNo ratings yet