You might also like
- Diagnosis and Management of Oral MucositisDocument20 pagesDiagnosis and Management of Oral MucositisAlfyGototronNo ratings yet
- Oral Health in Children With Leukemia: Review ArticleDocument8 pagesOral Health in Children With Leukemia: Review ArticleNindy TweelingenNo ratings yet
- 1752 1947 3 98Document4 pages1752 1947 3 98Rini RiantiNo ratings yet
- Importance of Pharmacist Intervention in The Management of Ulcerative Colitis-A Case StudyDocument4 pagesImportance of Pharmacist Intervention in The Management of Ulcerative Colitis-A Case StudyVasavi KishanNo ratings yet
- Ok PM BellaDocument25 pagesOk PM Bellapark kinanNo ratings yet
- Mejia 2017Document12 pagesMejia 2017Hadiqa AlmasNo ratings yet
- Maxillary Ulceration Resulting From Using A Rapid Maxillary Expander in A Diabetic PatientDocument5 pagesMaxillary Ulceration Resulting From Using A Rapid Maxillary Expander in A Diabetic PatientPrabowo BomazdicahyoNo ratings yet
- Antimicrobial Photodynamic Theraphy Combined With Periodontal TreatmentDocument6 pagesAntimicrobial Photodynamic Theraphy Combined With Periodontal Treatmentahmad ridlo hanifudin tahierNo ratings yet
- Chemotherapyorradiation-Inducedoralmucositis: Rajesh V. Lalla,, Deborah P. Saunders,, Douglas E. PetersonDocument9 pagesChemotherapyorradiation-Inducedoralmucositis: Rajesh V. Lalla,, Deborah P. Saunders,, Douglas E. PetersonKaren AnguloNo ratings yet
- A Review and Guide To Drug Associated Oral Adverse Effects-Oral Mucosal and Lichenoid Reactions. Part 2Document10 pagesA Review and Guide To Drug Associated Oral Adverse Effects-Oral Mucosal and Lichenoid Reactions. Part 2Sheila ParreirasNo ratings yet
- Mco 2 3 337 PDF PDFDocument4 pagesMco 2 3 337 PDF PDFhendra ardiantoNo ratings yet
- Diabetes and Periodontitis Link UpdateDocument5 pagesDiabetes and Periodontitis Link UpdateTarek NaeemNo ratings yet
- 2022 - TenOrio - Oral Manifestations of Autoimmune Polyglandular Syndrome Type 1Document5 pages2022 - TenOrio - Oral Manifestations of Autoimmune Polyglandular Syndrome Type 1NATALIA SILVA ANDRADENo ratings yet
- Diagnosis and Management of Benign Gastric and Duodenal DiseaseDocument16 pagesDiagnosis and Management of Benign Gastric and Duodenal DiseaseMaría Lourdes Rodríguez ZavalaNo ratings yet
- Holistic Management For Severe Oral Lichen Planus - A Case ReportDocument8 pagesHolistic Management For Severe Oral Lichen Planus - A Case Reportrahmania alikhlashNo ratings yet
- Managing Recurrent Oral Ulcers in Cushing's HabitusDocument4 pagesManaging Recurrent Oral Ulcers in Cushing's HabitusAzzNo ratings yet
- Management of Oral Lichen Plannus: A Clinical Study: Jayachandran S, Koijamsashikumar SDocument4 pagesManagement of Oral Lichen Plannus: A Clinical Study: Jayachandran S, Koijamsashikumar Sranz ibonkNo ratings yet
- Asia-Pacific Consensus Statements On Crohn's Disease. Part 2: ManagementDocument13 pagesAsia-Pacific Consensus Statements On Crohn's Disease. Part 2: ManagementtiaraNo ratings yet
- Type 2 diabetes and periodontal diseaseDocument10 pagesType 2 diabetes and periodontal diseaseObed AZARD -No ratings yet
- FF 304dysgeusia1Document3 pagesFF 304dysgeusia1Manuel HuamanNo ratings yet
- [03241750 - Acta Medica Bulgarica] Extraintestinal Manifestations and Intestinal Complications in Patients with Crohn's Disease_ Associations with Some Clinico-Laboratory Findings, Immunological Markers and Therapy.pdfDocument6 pages[03241750 - Acta Medica Bulgarica] Extraintestinal Manifestations and Intestinal Complications in Patients with Crohn's Disease_ Associations with Some Clinico-Laboratory Findings, Immunological Markers and Therapy.pdfTeodorNo ratings yet
- 2 ND JC PDF - SindhuDocument8 pages2 ND JC PDF - SindhuDadi SindhuNo ratings yet
- Challenge in DiagnosisDocument6 pagesChallenge in Diagnosissgoeldoc_550661200No ratings yet
- Photobiomodulation Therapy in The Treatment of Oral Mucositis, Dysphagia, Oral Dryness, Taste Alteration, and Burning Mouth Sensation Due To Cancer Therapy: A Case SeriesDocument11 pagesPhotobiomodulation Therapy in The Treatment of Oral Mucositis, Dysphagia, Oral Dryness, Taste Alteration, and Burning Mouth Sensation Due To Cancer Therapy: A Case SeriesRomian ValenciaNo ratings yet
- Crohn'S Disease: Rahul R Menon I MSC MB & GeDocument25 pagesCrohn'S Disease: Rahul R Menon I MSC MB & GerahulbioNo ratings yet
- Crohn's DiseaseDocument8 pagesCrohn's DiseaseShannen Madrid Tindugan100% (1)
- Periodontal Status and Risk Factors in Patients WiDocument16 pagesPeriodontal Status and Risk Factors in Patients Wipennyshevlin1No ratings yet
- Jada 2003 Vernillo 24S 33SDocument10 pagesJada 2003 Vernillo 24S 33SnobelcyrilNo ratings yet
- Generalized Severe Periodontitis and Periodontal Abscess in Type 2 Diabetes A Case ReportDocument6 pagesGeneralized Severe Periodontitis and Periodontal Abscess in Type 2 Diabetes A Case ReportMarisa PramasheillaNo ratings yet
- Denture Stomatitis and DMDocument6 pagesDenture Stomatitis and DMNajeeb UllahNo ratings yet
- Eficacy of Cryotherapy in The Prevention of Oral Mucosistis inDocument15 pagesEficacy of Cryotherapy in The Prevention of Oral Mucosistis inPaola GilNo ratings yet
- Duodenal Ulcer - StatPearls - NCBI BookshelfDocument6 pagesDuodenal Ulcer - StatPearls - NCBI Bookshelfimehap033No ratings yet
- Oral Health and Type 2 DiabetesDocument3 pagesOral Health and Type 2 DiabeteseveliiiinNo ratings yet
- Clinical Classification of The Status of The Pulp and Dental HealthDocument15 pagesClinical Classification of The Status of The Pulp and Dental HealthrahaazadNo ratings yet
- JIAP April 2018 - The Association Between Inflammatory Bowel Disease and Periodontal Conditions - Is There A Common Bacterial Etiology?Document12 pagesJIAP April 2018 - The Association Between Inflammatory Bowel Disease and Periodontal Conditions - Is There A Common Bacterial Etiology?nadeen.yehiaNo ratings yet
- Characterization of A Novel Dual Murine Model of Chemotherapy-Induced Oral and Intestinal MucositisDocument18 pagesCharacterization of A Novel Dual Murine Model of Chemotherapy-Induced Oral and Intestinal MucositisJeQeJu-MuhjiNo ratings yet
- Periodontitis and DiabetesDocument3 pagesPeriodontitis and DiabetesPatricia JethaniNo ratings yet
- Diabetes.rtfDocument5 pagesDiabetes.rtfyumnaelahiNo ratings yet
- Diabetes and Periodontal Disease: A Bidirectional RelationshipDocument4 pagesDiabetes and Periodontal Disease: A Bidirectional RelationshipPentiya Vita AyuniNo ratings yet
- Oncological-Therapy Related Oral Mucositis As An Interdisciplinary Problem Literature ReviewDocument12 pagesOncological-Therapy Related Oral Mucositis As An Interdisciplinary Problem Literature ReviewHilya Aliva AufiaNo ratings yet
- Current Treatment of Oral Candidiasis: A Literature ReviewDocument12 pagesCurrent Treatment of Oral Candidiasis: A Literature ReviewgilangNo ratings yet
- Inflammatory Bowel DiseaseDocument66 pagesInflammatory Bowel Diseasestephanie gayetaNo ratings yet
- Role of Low-Level Laser Therapy As An Adjunct To Initial Periodontal Treatment in Type 2 Diabetic Patients A Split-Mouth Randomized Controlled Clinical TrialDocument5 pagesRole of Low-Level Laser Therapy As An Adjunct To Initial Periodontal Treatment in Type 2 Diabetic Patients A Split-Mouth Randomized Controlled Clinical Trialdeva devaNo ratings yet
- Case ReportDocument6 pagesCase ReportFahmi FirmansyahNo ratings yet
- Crohns Epidemio Diagnositco y TratamientoDocument16 pagesCrohns Epidemio Diagnositco y TratamientoSantiago ZamudioNo ratings yet
- Final Ugib Sec To BpudDocument17 pagesFinal Ugib Sec To BpudBaby Kate BONGCARASNo ratings yet
- RebamipideDocument5 pagesRebamipidejunerubinNo ratings yet
- Manage IBD with Biomarkers, Drug MonitoringDocument13 pagesManage IBD with Biomarkers, Drug MonitoringShafa ShaviraNo ratings yet
- Changing Trends in Peptic Ulcer Prevalence in A Tertiary Care Setting in The PhilippinesDocument3 pagesChanging Trends in Peptic Ulcer Prevalence in A Tertiary Care Setting in The PhilippinesRumelle ReyesNo ratings yet
- Associations of Blood Glucose Helper T Cells and Cytokine Levels With Degree of Periodontal Lesion in Type 2 Diabetes Mellitus Patients Accompanied by Chronic PeriodontitisAfrican Health SciencesDocument7 pagesAssociations of Blood Glucose Helper T Cells and Cytokine Levels With Degree of Periodontal Lesion in Type 2 Diabetes Mellitus Patients Accompanied by Chronic PeriodontitisAfrican Health SciencesnoorasyillaNo ratings yet
- Reviews: Clinical Implications of Mucosal Healing For The Management of IBDDocument15 pagesReviews: Clinical Implications of Mucosal Healing For The Management of IBDkaibullaevNo ratings yet
- An Investigation Into The Prevalence and Treatment of Oral MucositisDocument11 pagesAn Investigation Into The Prevalence and Treatment of Oral MucositisHilya Aliva AufiaNo ratings yet
- Review Article: Oral Health Impact Profile in Celiac Patients: Analysis of Recent Findings in A Literature ReviewDocument10 pagesReview Article: Oral Health Impact Profile in Celiac Patients: Analysis of Recent Findings in A Literature ReviewJohamurillocNo ratings yet
- IBD Final11Document41 pagesIBD Final11abraham debebeNo ratings yet
- Benefits of Nonsurgical Periodontal Treatment in Patients With Type 2 Diabetes Mellitus and Chronic Periodontitis: A Randomized Controlled TrialDocument22 pagesBenefits of Nonsurgical Periodontal Treatment in Patients With Type 2 Diabetes Mellitus and Chronic Periodontitis: A Randomized Controlled TrialliguojieNo ratings yet
- NewpudpaperDocument15 pagesNewpudpaperapi-2868560640% (1)
- Dental Perspective of Pemphigus VulgarisDocument5 pagesDental Perspective of Pemphigus VulgarisSherlyNo ratings yet
- Fast Facts: Inflammatory Bowel Disease: Translating the science into compassionate IBD careFrom EverandFast Facts: Inflammatory Bowel Disease: Translating the science into compassionate IBD careNo ratings yet
- Gastroenterology For General SurgeonsFrom EverandGastroenterology For General SurgeonsMatthias W. WichmannNo ratings yet
- Multiple Choice Questions: (Recent Question 2013)Document3 pagesMultiple Choice Questions: (Recent Question 2013)Dr-Sanjay SinghaniaNo ratings yet
- Epidemiology and Public HealthDocument21 pagesEpidemiology and Public HealthFatima SumabatNo ratings yet
- Vaccination CrisisDocument61 pagesVaccination CrisisShoshannah100% (7)
- COVID-19 Diagnostic ReportDocument2 pagesCOVID-19 Diagnostic ReportSheetalNo ratings yet
- EPISCLERITIS & ScleritisDocument14 pagesEPISCLERITIS & ScleritisChikita Artia SariNo ratings yet
- Clostridium Tetani: Scientific ClassificationDocument4 pagesClostridium Tetani: Scientific ClassificationGael Forbes RealNo ratings yet
- Laporan Obat Sesuai Foemularium Februari 2019Document24 pagesLaporan Obat Sesuai Foemularium Februari 2019Maria AmabiNo ratings yet
- Whats New in GINA 2021 FinalDocument47 pagesWhats New in GINA 2021 FinalHeriestian eriesNo ratings yet
- Verify Urine & Blood Test Reports OnlineDocument9 pagesVerify Urine & Blood Test Reports OnlineRajat singhNo ratings yet
- PDF 2125204723Document1 pagePDF 2125204723Abdul AleemNo ratings yet
- Dermatofitosis FitzpatrickDocument28 pagesDermatofitosis FitzpatrickFadli IlhamNo ratings yet
- Epiglottitis and LaryngitisDocument9 pagesEpiglottitis and Laryngitisputri balqisNo ratings yet
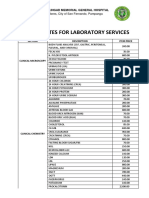
- JBLMGH Rates For Laboratory Services: Jose B. Lingad Memorial General HospitalDocument4 pagesJBLMGH Rates For Laboratory Services: Jose B. Lingad Memorial General HospitalApril NNo ratings yet
- Signs and SymptomsDocument6 pagesSigns and Symptomsdareine22No ratings yet
- Gram-Negative Rod Escherichia coliDocument25 pagesGram-Negative Rod Escherichia coliVer Garcera TalosigNo ratings yet
- Dr. Bernice E. Eddy Cutter VaccineDocument1 pageDr. Bernice E. Eddy Cutter VaccineCTSoldierNo ratings yet
- Community Acquired PneumoniaDocument17 pagesCommunity Acquired PneumoniaDaniel Puentes SánchezNo ratings yet
- Avian Influenza in ChickensDocument19 pagesAvian Influenza in ChickensShah NawazNo ratings yet
- Dyshidrotic Eczema: January 2014Document4 pagesDyshidrotic Eczema: January 2014Strawberry ShortcakeNo ratings yet
- Classification of Infectious Diseases by The Mechanism of TransmissionDocument17 pagesClassification of Infectious Diseases by The Mechanism of TransmissionAyomide AlayandeNo ratings yet
- Jennilyn Rose A. Atotubo, MD Joan E. Cerrada, MDDocument2 pagesJennilyn Rose A. Atotubo, MD Joan E. Cerrada, MDDenise DianeNo ratings yet
- MEMO - RV RTPCR - MergedDocument5 pagesMEMO - RV RTPCR - MergedMukesh KumarNo ratings yet
- Tuberculosis VaccineDocument15 pagesTuberculosis Vaccinesatheeshpharma6No ratings yet
- Smallpox Pamphlet Group 2Document3 pagesSmallpox Pamphlet Group 2classdocsNo ratings yet
- Top 10 Deadly Diseases You Can't CureDocument8 pagesTop 10 Deadly Diseases You Can't CureIlham Siloger GerhanadiNo ratings yet
- Lista DiagnosticeDocument566 pagesLista DiagnosticeGeanina MireaNo ratings yet
- Vero CellsDocument34 pagesVero Cellssyapina adewNo ratings yet
- This Study Resource Was: Dlugasch - Ch02-Applied Pathophysiology For The Advanced Practice Nurse, 1eDocument4 pagesThis Study Resource Was: Dlugasch - Ch02-Applied Pathophysiology For The Advanced Practice Nurse, 1eHugs0% (1)
- BTC023Document2 pagesBTC023jaskirat singhNo ratings yet




















![[03241750 - Acta Medica Bulgarica] Extraintestinal Manifestations and Intestinal Complications in Patients with Crohn's Disease_ Associations with Some Clinico-Laboratory Findings, Immunological Markers and Therapy.pdf](https://imgv2-1-f.scribdassets.com/img/document/472637710/149x198/2a81753cb8/1597598960?v=1)