You might also like
- Oxitard Capsules Improve Oral Submucous Fibrosis SymptomsDocument5 pagesOxitard Capsules Improve Oral Submucous Fibrosis SymptomssevattapillaiNo ratings yet
- 2022 - TenOrio - Oral Manifestations of Autoimmune Polyglandular Syndrome Type 1Document5 pages2022 - TenOrio - Oral Manifestations of Autoimmune Polyglandular Syndrome Type 1NATALIA SILVA ANDRADENo ratings yet
- Case Report Necrotizing Ulcerative Gingivitis, A Rare Manifestation As A Sequel of Drug-Induced Gingival Overgrowth: A Case ReportDocument7 pagesCase Report Necrotizing Ulcerative Gingivitis, A Rare Manifestation As A Sequel of Drug-Induced Gingival Overgrowth: A Case ReportPutri Dwi AnggrainiNo ratings yet
- Crohn's Disease: Low-Level Laser Therapy (LLLT) As An Adjuvant Treatment of Oral LesionsDocument6 pagesCrohn's Disease: Low-Level Laser Therapy (LLLT) As An Adjuvant Treatment of Oral LesionshilmiNo ratings yet
- 1752 1947 3 98Document4 pages1752 1947 3 98Rini RiantiNo ratings yet
- Physiotherapy Improves Mouth Opening in OSMFDocument9 pagesPhysiotherapy Improves Mouth Opening in OSMFViral ParekhNo ratings yet
- Sequelae of A Treated Stevens Johnson SyndromeA Case ReportDocument3 pagesSequelae of A Treated Stevens Johnson SyndromeA Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Drug Treatment of Oral Sub Mucous Fibrosis - A Review PDFDocument3 pagesDrug Treatment of Oral Sub Mucous Fibrosis - A Review PDFAnamika AttrishiNo ratings yet
- Podj 4Document6 pagesPodj 4cutchaimahNo ratings yet
- Ramsay Hunt Syndrome With Oral Findings - A Rare Case - CASE REPORT KEDUA BAGUSDocument7 pagesRamsay Hunt Syndrome With Oral Findings - A Rare Case - CASE REPORT KEDUA BAGUSfoto pasienNo ratings yet
- Case Report Benign Mucosal Membrane Pemphigoid As A Differential Diagnosis of Necrotizing Periodontal DiseaseDocument4 pagesCase Report Benign Mucosal Membrane Pemphigoid As A Differential Diagnosis of Necrotizing Periodontal DiseaseYeni PuspitasariNo ratings yet
- Benign Migratory Glossitis: Case Report and Literature ReviewDocument3 pagesBenign Migratory Glossitis: Case Report and Literature ReviewBharat NarumanchiNo ratings yet
- Homoeopathy Helps Manage Radiation-Induced Mucositis in NHLDocument44 pagesHomoeopathy Helps Manage Radiation-Induced Mucositis in NHLNavita SharmaNo ratings yet
- Lichen Planus Article PDFDocument3 pagesLichen Planus Article PDFSuresh KumarNo ratings yet
- KuretaseDocument3 pagesKuretaserindaNo ratings yet
- 7 CR 2 ArjunDocument4 pages7 CR 2 Arjunkiara wardanaNo ratings yet
- Abstract Kopapdi PendekDocument1 pageAbstract Kopapdi PendekRudy ChandraNo ratings yet
- Journal of Drug Discovery and Therapeutics 1 (4) 2013, 01-02Document2 pagesJournal of Drug Discovery and Therapeutics 1 (4) 2013, 01-02Bayu SaputroNo ratings yet
- 10 1093@qjmed@hcx164 PDFDocument2 pages10 1093@qjmed@hcx164 PDFAida Juniati SyafniNo ratings yet
- Case Report For A Refractory Recurrent Aphthous Stomatitis Treated With Jibaekpalmi-HwonDocument5 pagesCase Report For A Refractory Recurrent Aphthous Stomatitis Treated With Jibaekpalmi-HwonAL-ABATCHI -10No ratings yet
- Care Plan 1st YearDocument7 pagesCare Plan 1st Yearapi-562748135No ratings yet
- Oral Candidiasis: A Short Review and A Case Report: December 2018Document5 pagesOral Candidiasis: A Short Review and A Case Report: December 2018RAfii KerenNo ratings yet
- Candida-Associated Cheilitis: Online Images in The Medical SciencesDocument2 pagesCandida-Associated Cheilitis: Online Images in The Medical Sciencesfelaxis fNo ratings yet
- 6179 13644 1 SMDocument7 pages6179 13644 1 SMirma jovitaNo ratings yet
- Artículo de Periodoncia 2Document7 pagesArtículo de Periodoncia 2Margareth Roxanna Mendieta GirónNo ratings yet
- Management of Puberty Associated Gingival Enlargement in An Adolescent Female - A Case Report With A Follow-Up of 1 YearDocument4 pagesManagement of Puberty Associated Gingival Enlargement in An Adolescent Female - A Case Report With A Follow-Up of 1 YearDha Dina SevofrationNo ratings yet
- Drug-Induced Oral Candidiasis - A Case ReportDocument4 pagesDrug-Induced Oral Candidiasis - A Case ReportFajarRahmantiyoNo ratings yet
- 12 Sequel To Renal Transplant An Oral Physician's PerspectiveDocument5 pages12 Sequel To Renal Transplant An Oral Physician's PerspectivevinhannyNo ratings yet
- Chronic Inflammatory Gingival Enlargement: A CaseDocument3 pagesChronic Inflammatory Gingival Enlargement: A CaseArida Khoiruza Asy'ariNo ratings yet
- MagicMouthwash For OralMucositis Sol Stanford PDFDocument2 pagesMagicMouthwash For OralMucositis Sol Stanford PDFManuel ArenasNo ratings yet
- One Stage Full-Mouth Disinfection Improves Periodontitis OutcomesDocument14 pagesOne Stage Full-Mouth Disinfection Improves Periodontitis OutcomesAnita PrastiwiNo ratings yet
- Role of Buccal Fat Pad Versus Collagen in The Surgical Management of Oral Submucous Fibrosis: A Comparative EvaluationDocument4 pagesRole of Buccal Fat Pad Versus Collagen in The Surgical Management of Oral Submucous Fibrosis: A Comparative EvaluationASJADI SHEIKHNo ratings yet
- Chronic Suppurative Osteomyelitis of The Mandible CaseDocument4 pagesChronic Suppurative Osteomyelitis of The Mandible Caseporsche_cruiseNo ratings yet
- The Management of Herpes Labialis Oral Thrush andDocument5 pagesThe Management of Herpes Labialis Oral Thrush andFebri YolandaNo ratings yet
- Angular Cheilitis Guide: Causes, Symptoms & TreatmentDocument3 pagesAngular Cheilitis Guide: Causes, Symptoms & TreatmentNur Sita DewiNo ratings yet
- Erythema Multiforme: A Case Series and Review of Literature: November 2018Document8 pagesErythema Multiforme: A Case Series and Review of Literature: November 2018Nurlina NurdinNo ratings yet
- Stomatitis Medicamentosa Case Report SummaryDocument5 pagesStomatitis Medicamentosa Case Report Summaryathika yuraseptiNo ratings yet
- Lack of Reliable Evidence For Oral Submucous Fibrosis TreatmentsDocument2 pagesLack of Reliable Evidence For Oral Submucous Fibrosis TreatmentsashajangamNo ratings yet
- Apgh 3 1Document2 pagesApgh 3 1Rashmi Ranjan BeheraNo ratings yet
- Treatment Plan 2Document11 pagesTreatment Plan 2api-547661785No ratings yet
- Effectiveness of Micronutrients and Physiotherapy in The Management of Oral Submucous Fibrosis PDFDocument5 pagesEffectiveness of Micronutrients and Physiotherapy in The Management of Oral Submucous Fibrosis PDFNia LieantoNo ratings yet
- Treatment PlanningDocument5 pagesTreatment Planningapi-453476924No ratings yet
- Papillon Lefevre Syndrome-A Literature Review and Case ReportDocument7 pagesPapillon Lefevre Syndrome-A Literature Review and Case ReportnadhiracindyNo ratings yet
- JIndianSocPeriodontol214326-4026404 010706Document3 pagesJIndianSocPeriodontol214326-4026404 010706Fatma HandayaniNo ratings yet
- Ok PM BellaDocument25 pagesOk PM Bellapark kinanNo ratings yet
- Current Treatment of Oral Candidiasis: A Literature ReviewDocument12 pagesCurrent Treatment of Oral Candidiasis: A Literature ReviewgilangNo ratings yet
- Generalized Severe Periodontitis and Periodontal Abscess in Type 2 Diabetes A Case ReportDocument6 pagesGeneralized Severe Periodontitis and Periodontal Abscess in Type 2 Diabetes A Case ReportMarisa PramasheillaNo ratings yet
- 15 D16 298 Popovska MirjanaDocument5 pages15 D16 298 Popovska MirjanaVera Radojkova NikolovskaNo ratings yet
- Dental Journal: Burning Mouth Syndrome Caused by Xerostomia Secondary To AmlodipineDocument4 pagesDental Journal: Burning Mouth Syndrome Caused by Xerostomia Secondary To AmlodipinesafiraplNo ratings yet
- Jurnal Gingivitis Vivian 190631174Document5 pagesJurnal Gingivitis Vivian 190631174VivianNo ratings yet
- StomatitisDocument3 pagesStomatitiswidya RDNo ratings yet
- Tangible Results Following Scaling and Root Planing in Treating: Generalized Aggressive Periodontitis (GAP) - A Case ReportDocument8 pagesTangible Results Following Scaling and Root Planing in Treating: Generalized Aggressive Periodontitis (GAP) - A Case ReportDeanita PutriNo ratings yet
- Holistic Management For Severe Oral Lichen Planus - A Case ReportDocument8 pagesHolistic Management For Severe Oral Lichen Planus - A Case Reportrahmania alikhlashNo ratings yet
- 9410-Article Text-37001-1-10-20221215Document6 pages9410-Article Text-37001-1-10-20221215Julia KhaerunisaNo ratings yet
- Ojsadmin, 1340Document4 pagesOjsadmin, 1340Dr NisrinNo ratings yet
- Treating Oral Thrush in a Child with ItraconazoleDocument2 pagesTreating Oral Thrush in a Child with ItraconazoleaandakuNo ratings yet
- Clinical Characteristics of Patients With Oral CandidiasisDocument8 pagesClinical Characteristics of Patients With Oral CandidiasisHilya Aliva AufiaNo ratings yet
- Case Report: Idiopathic Orofacial Granulomatosis With Varied Clinical PresentationDocument4 pagesCase Report: Idiopathic Orofacial Granulomatosis With Varied Clinical PresentationPrince AhmedNo ratings yet
- Immunological Effectiveness of Immuno - and Biocorrective Treatment of Dental Diseases in Pregnant WomenDocument4 pagesImmunological Effectiveness of Immuno - and Biocorrective Treatment of Dental Diseases in Pregnant WomenCentral Asian StudiesNo ratings yet
- Antibiotic Prophylaxis in Patients With Rheumatic Heart Disease and Prosthetic DevicesDocument6 pagesAntibiotic Prophylaxis in Patients With Rheumatic Heart Disease and Prosthetic DevicesAzzNo ratings yet
- 2003JADGrandinianatomicpost PDFDocument5 pages2003JADGrandinianatomicpost PDFLeliNo ratings yet
- Oral Manifeststions of Endocrine DisorderDocument8 pagesOral Manifeststions of Endocrine DisorderpratheeparamkumarNo ratings yet
- WarfarinDocument19 pagesWarfarinAditya Dana IswaraNo ratings yet
- Is It Better To Restore or Extract Deciduous Teeth-A SurveyDocument3 pagesIs It Better To Restore or Extract Deciduous Teeth-A SurveyAzzNo ratings yet
- Website Covid PrecautionsDocument1 pageWebsite Covid PrecautionsAzzNo ratings yet
- MB2Systems May1995Document5 pagesMB2Systems May1995grzeniouNo ratings yet
- Heat Transfer Surfaces Guide PDFDocument8 pagesHeat Transfer Surfaces Guide PDFJohan ConradieNo ratings yet
- EMBRYOLOGYDocument4 pagesEMBRYOLOGYbhagavan prasadNo ratings yet
- Analysis of Alloy Constituents (Cu and ZnDocument5 pagesAnalysis of Alloy Constituents (Cu and Znaryan kushwaha100% (2)
- Sps 500 (STD) ProgramDocument164 pagesSps 500 (STD) Programwahyu100% (1)
- Product Brochure-Electronically Controlled Air Dryer-ECA PDFDocument4 pagesProduct Brochure-Electronically Controlled Air Dryer-ECA PDFAnonymous O0T8aZZNo ratings yet
- Working Length Determination in RCTDocument38 pagesWorking Length Determination in RCTDidar Sadiq Kwekha100% (1)
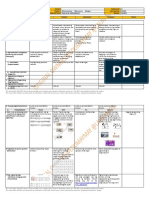
- DLL - MAPEH 4 - Q4 - W8 - New@edumaymay@lauramos@angieDocument8 pagesDLL - MAPEH 4 - Q4 - W8 - New@edumaymay@lauramos@angieDonna Lyn Domdom PadriqueNo ratings yet
- AU440-36V-MH: DimensionsDocument2 pagesAU440-36V-MH: DimensionsJohnny FucahoriNo ratings yet
- Examination of Power Electronics (Pel) : AnswerDocument10 pagesExamination of Power Electronics (Pel) : Answerves vegasNo ratings yet
- Opening SpeechDocument1 pageOpening SpeechTaniușa SavaNo ratings yet
- TDI - Full Cave Diver Course: TDI Instructor Manual Part 2 - Diver Standards Date: 12/31/2009 Revision: 10.0Document5 pagesTDI - Full Cave Diver Course: TDI Instructor Manual Part 2 - Diver Standards Date: 12/31/2009 Revision: 10.0BraulioNo ratings yet
- IIAP Mock 1 Answer KeyDocument6 pagesIIAP Mock 1 Answer KeyTGiF Travel0% (1)
- Surgical Technologist Resume SampleDocument2 pagesSurgical Technologist Resume Sampleresume7.com100% (3)
- DC-FAST 1.000, 2.000, 3.000, 5.000, 6.000 e 7.000 - New Project - 2021 - PT - BRDocument65 pagesDC-FAST 1.000, 2.000, 3.000, 5.000, 6.000 e 7.000 - New Project - 2021 - PT - BRCentrifugal SeparatorNo ratings yet
- Research ProposalDocument10 pagesResearch ProposalRonNo ratings yet
- Ecl7000 enDocument2 pagesEcl7000 ensuchaya tupyangNo ratings yet
- Name: Sport: Movement PrepDocument24 pagesName: Sport: Movement PrepS HNo ratings yet
- NSEA Solved Paper 2015Document30 pagesNSEA Solved Paper 2015vv12345670% (1)
- Help to Buy ISA GuideDocument4 pagesHelp to Buy ISA GuidefsdesdsNo ratings yet
- SC upholds reclusion perpetua for statutory rape within the familyDocument9 pagesSC upholds reclusion perpetua for statutory rape within the familymrvirginesNo ratings yet
- DBXLH 8585B VTMDocument4 pagesDBXLH 8585B VTMmau_mmx5738No ratings yet
- Validity and ReliabilityDocument13 pagesValidity and ReliabilityZarnigar AltafNo ratings yet
- Jsa-0002 - CCTV Pipe Inspection RapidDocument8 pagesJsa-0002 - CCTV Pipe Inspection RapidMohamad AfifNo ratings yet
- Barbecue Sauce HomadeDocument22 pagesBarbecue Sauce HomadeLiza NasrNo ratings yet
- VBAC Parents Guide v2 April 2019Document110 pagesVBAC Parents Guide v2 April 2019The VBAC Link100% (4)
- A Study To Assess The Knowledge of Antenatal Mothers Regarding Selected Minor Disorders Affecting PregnancyDocument4 pagesA Study To Assess The Knowledge of Antenatal Mothers Regarding Selected Minor Disorders Affecting PregnancyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Ecosystem Components and InteractionsDocument31 pagesEcosystem Components and InteractionsBirraa TajuNo ratings yet
- TS68Document52 pagesTS68finandariefNo ratings yet
- Seven Appear in Court On Cocaine, P Charges After North Island Drug Raids - NZ HeraldDocument3 pagesSeven Appear in Court On Cocaine, P Charges After North Island Drug Raids - NZ HeraldVagamundos ArgentinosNo ratings yet
- ANIMAL BEHAVIOR SCIENCEDocument37 pagesANIMAL BEHAVIOR SCIENCEZ AlbertNo ratings yet