You might also like
- The Management of Herpes Labialis Oral Thrush andDocument5 pagesThe Management of Herpes Labialis Oral Thrush andFebri YolandaNo ratings yet
- Management of Oral Manifestations in A Case of Cushing's HabitusDocument4 pagesManagement of Oral Manifestations in A Case of Cushing's HabitusAzzNo ratings yet
- Lichen Planus, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandLichen Planus, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Megaloblastic LeukemiaDocument5 pagesMegaloblastic Leukemiamy_scribd_account11No ratings yet
- Angular Cheilitis PDFDocument4 pagesAngular Cheilitis PDFandi winayaNo ratings yet
- 15 D16 298 Popovska MirjanaDocument5 pages15 D16 298 Popovska MirjanaVera Radojkova NikolovskaNo ratings yet
- Ijpi 3 2 75 79Document5 pagesIjpi 3 2 75 79Rabiatul AdawiyahNo ratings yet
- 2022 - TenOrio - Oral Manifestations of Autoimmune Polyglandular Syndrome Type 1Document5 pages2022 - TenOrio - Oral Manifestations of Autoimmune Polyglandular Syndrome Type 1NATALIA SILVA ANDRADENo ratings yet
- Benign Migratory Glossitis: Case Report and Literature ReviewDocument3 pagesBenign Migratory Glossitis: Case Report and Literature ReviewBharat NarumanchiNo ratings yet
- Clinical: Taste Change Associated With A Dental Procedure: Case Report and Review of The LiteratureDocument7 pagesClinical: Taste Change Associated With A Dental Procedure: Case Report and Review of The LiteraturemumutdwsNo ratings yet
- Angular Cheilitis Induced Defisiensi BesiDocument2 pagesAngular Cheilitis Induced Defisiensi Besiucy lucyana rusidaNo ratings yet
- Holistic Management For Severe Oral Lichen Planus - A Case ReportDocument8 pagesHolistic Management For Severe Oral Lichen Planus - A Case Reportrahmania alikhlashNo ratings yet
- Physiotherapy For Improving Mouth Opening & Tongue Protrution in Patients With Oral Submucous Fibrosis (OSMF) - Case SeriesDocument9 pagesPhysiotherapy For Improving Mouth Opening & Tongue Protrution in Patients With Oral Submucous Fibrosis (OSMF) - Case SeriesViral ParekhNo ratings yet
- Treatment Plan 2Document11 pagesTreatment Plan 2api-547661785No ratings yet
- Lichen Planus Article PDFDocument3 pagesLichen Planus Article PDFSuresh KumarNo ratings yet
- Safari - 29 Mar 2019 21.26Document1 pageSafari - 29 Mar 2019 21.26DwiNo ratings yet
- Conservative Management of Amlodipine Induced Gingival Enlargement: A ClinicalDocument3 pagesConservative Management of Amlodipine Induced Gingival Enlargement: A ClinicalachmadsyobriNo ratings yet
- Lichen Planus PDFDocument5 pagesLichen Planus PDFRobins DhakalNo ratings yet
- Papillon Lefevre Syndrome-A Literature Review and Case ReportDocument7 pagesPapillon Lefevre Syndrome-A Literature Review and Case ReportnadhiracindyNo ratings yet
- Generalized Severe Periodontitis and Periodontal Abscess in Type 2 Diabetes A Case ReportDocument6 pagesGeneralized Severe Periodontitis and Periodontal Abscess in Type 2 Diabetes A Case ReportMarisa PramasheillaNo ratings yet
- Oral Erythroplakia - A Case Report: Mahendra Patait, Urvashi Nikate, Kedar Saraf, Priyanka Singh and Vishal JadhavDocument4 pagesOral Erythroplakia - A Case Report: Mahendra Patait, Urvashi Nikate, Kedar Saraf, Priyanka Singh and Vishal JadhavhelmysiswantoNo ratings yet
- A CASE OF RADIATION - INDUCED MUCOSITiS - PPTX NAVITADocument44 pagesA CASE OF RADIATION - INDUCED MUCOSITiS - PPTX NAVITANavita SharmaNo ratings yet
- Dental Journal: Burning Mouth Syndrome Caused by Xerostomia Secondary To AmlodipineDocument4 pagesDental Journal: Burning Mouth Syndrome Caused by Xerostomia Secondary To AmlodipinesafiraplNo ratings yet
- Podj 4 PDFDocument3 pagesPodj 4 PDFNur Sita DewiNo ratings yet
- Determination of Salivary Levels of Mucin and Amylase in Chronic Periodontitis PacientsDocument7 pagesDetermination of Salivary Levels of Mucin and Amylase in Chronic Periodontitis PacientsOctavian BoaruNo ratings yet
- Case Report Necrotizing Ulcerative Gingivitis, A Rare Manifestation As A Sequel of Drug-Induced Gingival Overgrowth: A Case ReportDocument7 pagesCase Report Necrotizing Ulcerative Gingivitis, A Rare Manifestation As A Sequel of Drug-Induced Gingival Overgrowth: A Case ReportPutri Dwi AnggrainiNo ratings yet
- Case Study (Iph) Amoebiasis Diarrhea With Mild DHNDocument9 pagesCase Study (Iph) Amoebiasis Diarrhea With Mild DHNLance_Joshua_7907No ratings yet
- Dentino Jurnal Kedokteran Gigi: Vol IV. No 1. Maret 2019Document4 pagesDentino Jurnal Kedokteran Gigi: Vol IV. No 1. Maret 2019Lidya DiandraNo ratings yet
- Ok PM BellaDocument25 pagesOk PM Bellapark kinanNo ratings yet
- Txplan 2Document5 pagesTxplan 2api-453476924No ratings yet
- Crohn's Disease: Low-Level Laser Therapy (LLLT) As An Adjuvant Treatment of Oral LesionsDocument6 pagesCrohn's Disease: Low-Level Laser Therapy (LLLT) As An Adjuvant Treatment of Oral LesionshilmiNo ratings yet
- Mucopolysaccharidosis MPS Review of The LiteratureDocument7 pagesMucopolysaccharidosis MPS Review of The Literatureadinda kerenNo ratings yet
- Tratamiento Con AINESDocument6 pagesTratamiento Con AINESCarol Chávez MedinaNo ratings yet
- A Systematic Approach To Xerostomia Diagnosis and ManagementDocument10 pagesA Systematic Approach To Xerostomia Diagnosis and ManagementLeHoaiNo ratings yet
- Oral Hygiene Day 2021: Oral Health Care and DiabetesDocument40 pagesOral Hygiene Day 2021: Oral Health Care and DiabetesAASIM AlamNo ratings yet
- Microflora Analysis of Saliva Causing Chronic Periodontitis in Type 2 Diabetic PatientDocument16 pagesMicroflora Analysis of Saliva Causing Chronic Periodontitis in Type 2 Diabetic PatientArslan JavedNo ratings yet
- JR IPM - Comprehensive Management of Oral Frailty in Multiple Systemic Disease Geriatric Patient (Case Report)Document30 pagesJR IPM - Comprehensive Management of Oral Frailty in Multiple Systemic Disease Geriatric Patient (Case Report)NUR HAYUNINGTYASNo ratings yet
- The Treatment of Oral Lesions in Behcets SyndromeDocument5 pagesThe Treatment of Oral Lesions in Behcets SyndromeUtami MayasariNo ratings yet
- Jurnal SistemikDocument3 pagesJurnal SistemikMariatun Zahro NasutionNo ratings yet
- Exfoliative Cheilitis ReportDocument1 pageExfoliative Cheilitis ReportYani YoelianiNo ratings yet
- Capstone ProjectDocument36 pagesCapstone Projectapi-462295397No ratings yet
- Oral Health in Children With Leukemia: Review ArticleDocument8 pagesOral Health in Children With Leukemia: Review ArticleNindy TweelingenNo ratings yet
- The Periodontal ManagementDocument7 pagesThe Periodontal ManagementAnshori 'arie' RohimiNo ratings yet
- Changes in Salivary Flow Rate and PH in Stressful ConditionsDocument6 pagesChanges in Salivary Flow Rate and PH in Stressful ConditionsNgọc Kim Bảo NguyễnNo ratings yet
- Allergicstomatitis 2012Document6 pagesAllergicstomatitis 2012Agustine Hanafi PutriNo ratings yet
- Case Study 2Document8 pagesCase Study 2api-547898337No ratings yet
- 2016 Article 913Document5 pages2016 Article 913housic1No ratings yet
- Acute Submandibular Sialadenitis-A Case ReportDocument4 pagesAcute Submandibular Sialadenitis-A Case ReportsurgaNo ratings yet
- Care Plan 1st YearDocument7 pagesCare Plan 1st Yearapi-562748135No ratings yet
- Case Report Benign Mucosal Membrane Pemphigoid As A Differential Diagnosis of Necrotizing Periodontal DiseaseDocument4 pagesCase Report Benign Mucosal Membrane Pemphigoid As A Differential Diagnosis of Necrotizing Periodontal DiseaseYeni PuspitasariNo ratings yet
- Capstone Paper 1Document16 pagesCapstone Paper 1api-409808326No ratings yet
- Efficacy of 25% Glucose in Glycerin and Honey in The Management of Primary Atrophic Rhinitis: A Comparative Prospective StudyDocument4 pagesEfficacy of 25% Glucose in Glycerin and Honey in The Management of Primary Atrophic Rhinitis: A Comparative Prospective StudySathiyamoorthy KarunakaranNo ratings yet
- Treatment PlanningDocument5 pagesTreatment Planningapi-453476924No ratings yet
- JR IpmDocument85 pagesJR IpmNUR HAYUNINGTYASNo ratings yet
- Erosive Lichen Planus: A Case ReportDocument4 pagesErosive Lichen Planus: A Case ReportNuningK93No ratings yet
- Iaat 12 I 2 P 458Document5 pagesIaat 12 I 2 P 458Virma PutraNo ratings yet
- 4.management of Aphthous Ulceration With Topical QuercetinDocument9 pages4.management of Aphthous Ulceration With Topical QuercetinCoste Iulia RoxanaNo ratings yet
- HangersSupportsReferenceDataGuide PDFDocument57 pagesHangersSupportsReferenceDataGuide PDFIndra RosadiNo ratings yet
- Study and Interpretation of The ScoreDocument10 pagesStudy and Interpretation of The ScoreDwightPile-GrayNo ratings yet
- Module 7 NSTP 1Document55 pagesModule 7 NSTP 1PanJan BalNo ratings yet
- The Phases of The Moon Station Activity Worksheet Pa2Document3 pagesThe Phases of The Moon Station Activity Worksheet Pa2api-284353863100% (1)
- Bagian AwalDocument17 pagesBagian AwalCitra Monalisa LaoliNo ratings yet
- Ships Near A Rocky Coast With Awaiting Landing PartyDocument2 pagesShips Near A Rocky Coast With Awaiting Landing PartyFouaAj1 FouaAj1No ratings yet
- Solutions DPP 2Document3 pagesSolutions DPP 2Tech. VideciousNo ratings yet
- You Can't Blame A FireDocument8 pagesYou Can't Blame A FireMontana QuarterlyNo ratings yet
- HDO OpeationsDocument28 pagesHDO OpeationsAtif NadeemNo ratings yet
- ABHA Coil ProportionsDocument5 pagesABHA Coil ProportionsOctav OctavianNo ratings yet
- Chapter 4: Thermal ComfortDocument16 pagesChapter 4: Thermal ComfortWengelNo ratings yet
- Sharat Babu Digumarti Vs State, Govt. of NCT of Delhi (Bazee - Com Case, Appeal) - Information Technology ActDocument17 pagesSharat Babu Digumarti Vs State, Govt. of NCT of Delhi (Bazee - Com Case, Appeal) - Information Technology ActRavish Rana100% (1)
- Ubicomp PracticalDocument27 pagesUbicomp Practicalvikrant sharmaNo ratings yet
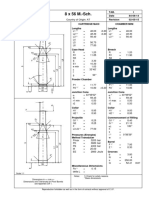
- 8 X 56 M.-SCH.: Country of Origin: ATDocument1 page8 X 56 M.-SCH.: Country of Origin: ATMohammed SirelkhatimNo ratings yet
- CBSE 10th ResultsDocument1 pageCBSE 10th ResultsAkshit SinghNo ratings yet
- Air Blower ManualDocument16 pagesAir Blower ManualshaiknayeemabbasNo ratings yet
- Tata NanoDocument25 pagesTata Nanop01p100% (1)
- Addendum ESIA Oct 2019Document246 pagesAddendum ESIA Oct 2019melkamuNo ratings yet
- An Analysis of Students' Error in Using Possesive Adjective in Their Online Writing TasksDocument19 pagesAn Analysis of Students' Error in Using Possesive Adjective in Their Online Writing TasksKartika Dwi NurandaniNo ratings yet
- JEE Mains Paper 1 (12 Apr 2019 Shift 2) EnglishDocument131 pagesJEE Mains Paper 1 (12 Apr 2019 Shift 2) EnglishRudraksha KushwahaNo ratings yet
- Thermal Physics Lecture 1Document53 pagesThermal Physics Lecture 1Swee Boon OngNo ratings yet
- Guidelines For Doing Business in Grenada & OECSDocument14 pagesGuidelines For Doing Business in Grenada & OECSCharcoals Caribbean GrillNo ratings yet
- 95-03097 Ballvlv300350 WCB PDFDocument26 pages95-03097 Ballvlv300350 WCB PDFasitdeyNo ratings yet
- 02 CT311 Site WorksDocument26 pages02 CT311 Site Worksshaweeeng 101No ratings yet
- Fortnite Task Courier Pack 1500 V Bucks - BuscarDocument1 pageFortnite Task Courier Pack 1500 V Bucks - Buscariancard321No ratings yet
- Ticket: Fare DetailDocument1 pageTicket: Fare DetailSajal NahaNo ratings yet
- Previews 1633186 PreDocument11 pagesPreviews 1633186 PreDavid MorenoNo ratings yet
- Unit 1 Bearer PlantsDocument2 pagesUnit 1 Bearer PlantsEmzNo ratings yet
- QAU TTS Form Annual AssessmentDocument6 pagesQAU TTS Form Annual AssessmentsohaibtarikNo ratings yet
- Densha: Memories of A Train Ride Through Kyushu: By: Scott NesbittDocument7 pagesDensha: Memories of A Train Ride Through Kyushu: By: Scott Nesbittapi-16144421No ratings yet
- Summary of Mary Claire Haver's The Galveston DietFrom EverandSummary of Mary Claire Haver's The Galveston DietRating: 5 out of 5 stars5/5 (1)
- Forever Strong: A New, Science-Based Strategy for Aging WellFrom EverandForever Strong: A New, Science-Based Strategy for Aging WellNo ratings yet
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookFrom EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookRating: 3.5 out of 5 stars3.5/5 (2)
- Find Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeFrom EverandFind Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeRating: 4 out of 5 stars4/5 (3)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyFrom EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyRating: 4.5 out of 5 stars4.5/5 (3)
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomFrom EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomRating: 4 out of 5 stars4/5 (1)
- Secrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainFrom EverandSecrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainRating: 3.5 out of 5 stars3.5/5 (38)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisFrom EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisRating: 3 out of 5 stars3/5 (2)
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonFrom EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonRating: 3.5 out of 5 stars3.5/5 (33)
- Grit & Grace: Train the Mind, Train the Body, Own Your LifeFrom EverandGrit & Grace: Train the Mind, Train the Body, Own Your LifeRating: 4 out of 5 stars4/5 (3)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)From EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Rating: 4 out of 5 stars4/5 (411)
- Sugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthFrom EverandSugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthRating: 4 out of 5 stars4/5 (6)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeFrom EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNo ratings yet
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsFrom EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsRating: 4 out of 5 stars4/5 (49)
- Glucose Revolution: The Life-Changing Power of Balancing Your Blood SugarFrom EverandGlucose Revolution: The Life-Changing Power of Balancing Your Blood SugarRating: 5 out of 5 stars5/5 (351)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouFrom EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouNo ratings yet
- The Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyFrom EverandThe Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyNo ratings yet
- How to Be Well: The 6 Keys to a Happy and Healthy LifeFrom EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeRating: 5 out of 5 stars5/5 (1)
- The Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingFrom EverandThe Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingRating: 4 out of 5 stars4/5 (3)
- The End of Craving: Recovering the Lost Wisdom of Eating WellFrom EverandThe End of Craving: Recovering the Lost Wisdom of Eating WellRating: 4.5 out of 5 stars4.5/5 (82)
- The Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodFrom EverandThe Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodNo ratings yet
- Hungry for Change: Ditch the Diets, Conquer the Cravings, and Eat Your Way to Lifelong HealthFrom EverandHungry for Change: Ditch the Diets, Conquer the Cravings, and Eat Your Way to Lifelong HealthRating: 4 out of 5 stars4/5 (7)
- Allen Carr's Easy Way for Women to Lose Weight: The original Easyway methodFrom EverandAllen Carr's Easy Way for Women to Lose Weight: The original Easyway methodRating: 4.5 out of 5 stars4.5/5 (18)
- Molecules of Emotion: Why You Feel the Way You FeelFrom EverandMolecules of Emotion: Why You Feel the Way You FeelRating: 4 out of 5 stars4/5 (128)
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthFrom EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthNo ratings yet
- Keto Friendly Recipes: Easy Keto For Busy PeopleFrom EverandKeto Friendly Recipes: Easy Keto For Busy PeopleRating: 3.5 out of 5 stars3.5/5 (2)