You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Sin Missing The MarkDocument2 pagesSin Missing The MarkCeray67No ratings yet
- (De) Forming Woman - Images of Feminine Political Subjectivity in Latin American Literature, From Disappearance To FemicideDocument1 page(De) Forming Woman - Images of Feminine Political Subjectivity in Latin American Literature, From Disappearance To FemicideAndreia AlmeidaNo ratings yet
- Asakura (2008) Returning To The "Homeland" - Work-Related Ethnic Discrimination and The Health of Japanese Brazilians in JapanDocument9 pagesAsakura (2008) Returning To The "Homeland" - Work-Related Ethnic Discrimination and The Health of Japanese Brazilians in JapanAndreia AlmeidaNo ratings yet
- (A) Canfield (2017) Determinants of Substance Use Amongst Brazilians Residing in The UK - The Role of AcculturationDocument11 pages(A) Canfield (2017) Determinants of Substance Use Amongst Brazilians Residing in The UK - The Role of AcculturationAndreia AlmeidaNo ratings yet
- CH 02 The Transnational Turn - Looking Back and Looking AheadDocument18 pagesCH 02 The Transnational Turn - Looking Back and Looking AheadAndreia AlmeidaNo ratings yet
- (A) Lazar-Neto (2017) Depression and Its Correlates Among Brazilian Immigrants in Massachusetts PDFDocument9 pages(A) Lazar-Neto (2017) Depression and Its Correlates Among Brazilian Immigrants in Massachusetts PDFAndreia AlmeidaNo ratings yet
- (A) Lindsay (2019) Parenting PracticesDocument19 pages(A) Lindsay (2019) Parenting PracticesAndreia AlmeidaNo ratings yet
- Bianchi (2010) Partner - Selection - Among - LatinoDocument11 pagesBianchi (2010) Partner - Selection - Among - LatinoAndreia AlmeidaNo ratings yet
- Treatment of Psychological DisordersDocument34 pagesTreatment of Psychological DisordersAndreia AlmeidaNo ratings yet
- Life Span Development: A Six-Unit Lesson Plan For High School Psychology TeachersDocument52 pagesLife Span Development: A Six-Unit Lesson Plan For High School Psychology TeachersAndreia AlmeidaNo ratings yet
- (2008) Frosh & Baraister Psychoanalysis - and - Psychosocial - StudiesDocument21 pages(2008) Frosh & Baraister Psychoanalysis - and - Psychosocial - StudiesAndreia Almeida100% (1)
- Deep Maternal AlienationDocument4 pagesDeep Maternal AlienationAndreia AlmeidaNo ratings yet
- Gibson (2010) - Professional Identity Development - A Grounded Theory of Transformational Tasks of New Counselors.Document19 pagesGibson (2010) - Professional Identity Development - A Grounded Theory of Transformational Tasks of New Counselors.Andreia AlmeidaNo ratings yet
- Taking A Stand: Using Psychoanalysis To Explore The Positioning of Subjects in DiscourseDocument15 pagesTaking A Stand: Using Psychoanalysis To Explore The Positioning of Subjects in DiscourseAndreia AlmeidaNo ratings yet
- Differentiated frames in sport psychology: Using workshops to develop capacitiesDocument9 pagesDifferentiated frames in sport psychology: Using workshops to develop capacitiesAndreia AlmeidaNo ratings yet
- Addiction From The Harmful Dysfunction Perspective - How There Can Be A Mental Disorder in A Normal Brain PDFDocument9 pagesAddiction From The Harmful Dysfunction Perspective - How There Can Be A Mental Disorder in A Normal Brain PDFAndreia AlmeidaNo ratings yet
- Feminist Historiography As Methodology T PDFDocument38 pagesFeminist Historiography As Methodology T PDFAndreia AlmeidaNo ratings yet
- Parent - Teacher Agreement On ADHD Symptoms Across Development27Document22 pagesParent - Teacher Agreement On ADHD Symptoms Across Development27Andreia AlmeidaNo ratings yet
- Clinical Utility of The Vanderbilt ADHD Diagnostic Parent Rating Scale Comorbidity Screening ScalesDocument15 pagesClinical Utility of The Vanderbilt ADHD Diagnostic Parent Rating Scale Comorbidity Screening ScalesAndreia AlmeidaNo ratings yet
- (2014) Frosh The Nature of The Psychosocial - Debates From Studies in The PsychosocialDocument11 pages(2014) Frosh The Nature of The Psychosocial - Debates From Studies in The PsychosocialAndreia AlmeidaNo ratings yet
- Wolraich (2003) Psychometric Properties of The Vanderbilt ADHD Diagnostic Parent Rating Scale in A Referred PopulationDocument11 pagesWolraich (2003) Psychometric Properties of The Vanderbilt ADHD Diagnostic Parent Rating Scale in A Referred PopulationAndreia AlmeidaNo ratings yet
- The Diagnosis of Mental Disorders: The Problem of ReificationDocument25 pagesThe Diagnosis of Mental Disorders: The Problem of ReificationAndreia AlmeidaNo ratings yet
- HammenDocument18 pagesHammenAndreia AlmeidaNo ratings yet
- Beck PDFDocument13 pagesBeck PDFAndreia AlmeidaNo ratings yet
- HaroonDocument26 pagesHaroonAndreia AlmeidaNo ratings yet
- PDF - Webb & Lee, 2011Document16 pagesPDF - Webb & Lee, 2011Andreia AlmeidaNo ratings yet
- Revisão AnsiedadeDocument30 pagesRevisão AnsiedadeEzequiel NascimentoNo ratings yet
- Lee& Webb, 2014Document22 pagesLee& Webb, 2014Andreia AlmeidaNo ratings yet
- Chapter One PDFDocument30 pagesChapter One PDFAndreia AlmeidaNo ratings yet
- The Changing Role of LibrariesDocument8 pagesThe Changing Role of LibrarieseducationdoctorNo ratings yet
- Quality Home AppliancesDocument3 pagesQuality Home AppliancesKevin WillisNo ratings yet
- Calendar - CWDocument5 pagesCalendar - CWshashi dhotreNo ratings yet
- What Are Montane Forests?Document3 pagesWhat Are Montane Forests?Anonymous Kip5Q1YgdNo ratings yet
- Indian Constitutional Law and Philosophy - Page 9Document32 pagesIndian Constitutional Law and Philosophy - Page 9Prinsu SenNo ratings yet
- Aqeelcv New For Print2Document6 pagesAqeelcv New For Print2Jawad KhawajaNo ratings yet
- Understanding The Mindanao ConflictDocument7 pagesUnderstanding The Mindanao ConflictInday Espina-VaronaNo ratings yet
- An Interview with Novelist Anita BrooknerDocument12 pagesAn Interview with Novelist Anita BrooknerlupearriegueNo ratings yet
- Canadian Hot Rods - January 2015Document100 pagesCanadian Hot Rods - January 2015RichardNo ratings yet
- AMA - Australias Forest Industries at A GlanceDocument2 pagesAMA - Australias Forest Industries at A GlanceCarlos D. GuiradosNo ratings yet
- The Core Beliefs and Practices of SikhismDocument26 pagesThe Core Beliefs and Practices of SikhismGVNo ratings yet
- Introducing Bill Evans: Nat HentoffDocument2 pagesIntroducing Bill Evans: Nat HentoffSeda BalcıNo ratings yet
- Case StudyDocument3 pagesCase StudyCrystal HolgadoNo ratings yet
- Application For Admission To Master of Computer Applications (MCA) COURSES, KERALA: 2010-2011Document5 pagesApplication For Admission To Master of Computer Applications (MCA) COURSES, KERALA: 2010-2011anishbaiNo ratings yet
- Complaint For Maintenance of Possession and of Agricultural LeaseholdDocument12 pagesComplaint For Maintenance of Possession and of Agricultural LeaseholdluckyNo ratings yet
- Functions of MoneyDocument15 pagesFunctions of MoneyRidhima MathurNo ratings yet
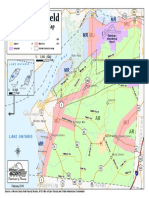
- Town of Hounsfield Zoning Map Feb 2016Document1 pageTown of Hounsfield Zoning Map Feb 2016pandorasboxofrocksNo ratings yet
- Framework of Understanding Taxes in The Philippines-1Document9 pagesFramework of Understanding Taxes in The Philippines-1Mergierose DalgoNo ratings yet
- Weekly Home Learning Plan: Placido T. Amo Senior High SchoolDocument12 pagesWeekly Home Learning Plan: Placido T. Amo Senior High SchoolMary Cherill UmaliNo ratings yet
- NATO Bombing of Yugoslavia (TEXT)Document4 pagesNATO Bombing of Yugoslavia (TEXT)ana milutinovicNo ratings yet
- IDCF Guidelines 2016Document47 pagesIDCF Guidelines 2016anunad100% (2)
- Shooting An ElephantDocument2 pagesShooting An ElephantShilpaDasNo ratings yet
- CCC Letter To CPMGDocument3 pagesCCC Letter To CPMGAjay PandeyNo ratings yet
- Review Quality Assurance PDFDocument339 pagesReview Quality Assurance PDFBelayneh TadesseNo ratings yet
- Culpable Homicide Section 299 and 300 of IPCDocument8 pagesCulpable Homicide Section 299 and 300 of IPCdinoopmvNo ratings yet
- 2 2005Document13 pages2 2005VinothKumarDhananjayan100% (1)
- Income-Tax-Calculator 2023-24Document8 pagesIncome-Tax-Calculator 2023-24AlokNo ratings yet
- A) Formal PowerDocument2 pagesA) Formal PowerTejas RathodNo ratings yet
- CyberOps Associate - CA - Lab Answers Archives - InfraExam 2022Document4 pagesCyberOps Associate - CA - Lab Answers Archives - InfraExam 2022arunshanNo ratings yet