You might also like
- The Companies' (Incorporation) Procedure in Japan: Akash Saxena - 17A014 Semester - VIDocument13 pagesThe Companies' (Incorporation) Procedure in Japan: Akash Saxena - 17A014 Semester - VIMeghna SinghNo ratings yet
- International Humanitarian Law (IHL) : Virtual ClassesDocument71 pagesInternational Humanitarian Law (IHL) : Virtual ClassesMeghna SinghNo ratings yet
- CH 8 Working Capital Management 2019Document77 pagesCH 8 Working Capital Management 2019Meghna SinghNo ratings yet
- Corporate Strategy: Mod Iii Topic 4Document27 pagesCorporate Strategy: Mod Iii Topic 4Meghna SinghNo ratings yet
- PRO BONO REPORT - EditedDocument3 pagesPRO BONO REPORT - EditedMeghna SinghNo ratings yet
- Nature of Indian ConstitutionDocument46 pagesNature of Indian ConstitutionMeghna SinghNo ratings yet
- Salient Features of Indian ConstitutionDocument28 pagesSalient Features of Indian ConstitutionMeghna SinghNo ratings yet
- Noshirwan Reply To AppDocument6 pagesNoshirwan Reply To AppMeghna SinghNo ratings yet
- Principles of Taxation Law - Ist Internal AssignmentDocument8 pagesPrinciples of Taxation Law - Ist Internal AssignmentMeghna SinghNo ratings yet
- New Doc 2019-10-22 00.10.31Document26 pagesNew Doc 2019-10-22 00.10.31Meghna SinghNo ratings yet
- Human Rights And: Nternational Umanitarian AWDocument15 pagesHuman Rights And: Nternational Umanitarian AWMeghna Singh100% (1)
- Text of The Constitution Including Preambles, Articles, Schedules Etc. It IsDocument14 pagesText of The Constitution Including Preambles, Articles, Schedules Etc. It IsMeghna SinghNo ratings yet
- (Assignment Towards Partial Fulfillment of The Assessment in The Subject of ADR) (Final Word Count: 2537, Excluding Footnotes)Document8 pages(Assignment Towards Partial Fulfillment of The Assessment in The Subject of ADR) (Final Word Count: 2537, Excluding Footnotes)Meghna SinghNo ratings yet
- Constitutional Law - Iii Assignment Paper: State of Bihar V. Bihar Pensioner'S Samaj Air 2006 SC 2100Document12 pagesConstitutional Law - Iii Assignment Paper: State of Bihar V. Bihar Pensioner'S Samaj Air 2006 SC 2100Meghna SinghNo ratings yet
- IN OUR CONSTITUENT ASSEMBLY This Twenty-Sixth Day of November, 1949, Do Hereby Adopt, Enact and Give To Ourselves This Constitution."Document6 pagesIN OUR CONSTITUENT ASSEMBLY This Twenty-Sixth Day of November, 1949, Do Hereby Adopt, Enact and Give To Ourselves This Constitution."Meghna SinghNo ratings yet
- Ihl - AgmDocument31 pagesIhl - AgmMeghna SinghNo ratings yet
- Family LawDocument29 pagesFamily LawMeghna SinghNo ratings yet
- Admin ProjectDocument23 pagesAdmin ProjectMeghna SinghNo ratings yet
- 17A014 10 Mark Assignment TPA 2020Document7 pages17A014 10 Mark Assignment TPA 2020Meghna SinghNo ratings yet
- RPO/analysis-of-state-RPO-regulations - PDF: Elationship Between Domestic ANDDocument64 pagesRPO/analysis-of-state-RPO-regulations - PDF: Elationship Between Domestic ANDMeghna SinghNo ratings yet
- Compensation To Clinical Trial Participants in India - A Gap AnalysisDocument8 pagesCompensation To Clinical Trial Participants in India - A Gap AnalysisMeghna SinghNo ratings yet
- GST DissertationDocument33 pagesGST DissertationMeghna SinghNo ratings yet
- CompiledDocument17 pagesCompiledMeghna SinghNo ratings yet
- Securities End Sem NotesDocument31 pagesSecurities End Sem NotesMeghna SinghNo ratings yet
- Gujarat National Law University: WTO Limitations On Trade Measures To Enforce Ocean ConservationDocument20 pagesGujarat National Law University: WTO Limitations On Trade Measures To Enforce Ocean ConservationMeghna SinghNo ratings yet
- Naman Devpura and Sakshya Jain PDFDocument22 pagesNaman Devpura and Sakshya Jain PDFMeghna SinghNo ratings yet
- Economics II ProjectDocument20 pagesEconomics II ProjectMeghna SinghNo ratings yet
- New Drugs and Clinical Trials Rules, 2019 - A Regulatory Overview - India Corporate LawDocument7 pagesNew Drugs and Clinical Trials Rules, 2019 - A Regulatory Overview - India Corporate LawMeghna SinghNo ratings yet
- Gujarat National Law University: Utmost Good FaithDocument26 pagesGujarat National Law University: Utmost Good FaithMeghna SinghNo ratings yet
- Essar Steel CaseDocument3 pagesEssar Steel CaseMeghna SinghNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Failure Patterns of Different Bracket Systems and Their Influence On Treatment Duration - A Retrospective Cohort StudyDocument10 pagesFailure Patterns of Different Bracket Systems and Their Influence On Treatment Duration - A Retrospective Cohort StudyHuma SaleemNo ratings yet
- 2022 NEHCC Registration ProgramDocument20 pages2022 NEHCC Registration ProgramHome Care, Hospice Palliative Care Alliance NHNo ratings yet
- OSPEDocument5 pagesOSPEKavya RajuNo ratings yet
- This Study Resource Was: Chapter 9: Essay QuestionsDocument5 pagesThis Study Resource Was: Chapter 9: Essay QuestionsSherlock HolmesNo ratings yet
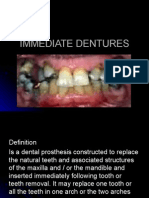
- Immediate DenturesDocument23 pagesImmediate DenturesWael FahadNo ratings yet
- A Case Study On Employee Engagement: Marriott International, IncDocument12 pagesA Case Study On Employee Engagement: Marriott International, IncPreeti Singh Yadav Student, Jaipuria LucknowNo ratings yet
- Observational StudiesDocument4 pagesObservational StudiesDavid PaulNo ratings yet
- Evaluation VII Back To The Future Grecia BecerraDocument8 pagesEvaluation VII Back To The Future Grecia BecerraGrecia BecerraNo ratings yet
- If Your Baby Is BreechDocument16 pagesIf Your Baby Is BreechAryana BudiawanNo ratings yet
- Eova PDFDocument5 pagesEova PDFWenni QorinnaNo ratings yet
- Case 1 Health PlusDocument2 pagesCase 1 Health PlusCia SevillaNo ratings yet
- Typhidot TestDocument1 pageTyphidot TestPre Cadet AcademyNo ratings yet
- Acute Necrotizing Ulcerative GingivitisDocument7 pagesAcute Necrotizing Ulcerative GingivitisdonnyNo ratings yet
- Elizabeth Garrett AndersonDocument2 pagesElizabeth Garrett AndersonvvvNo ratings yet
- Dermatomyositis NCPDocument3 pagesDermatomyositis NCPMakki MarcosNo ratings yet
- Health System in PakistanDocument2 pagesHealth System in PakistanbukhariNo ratings yet
- National Survey of Long-Haul Truck Driver Health and Injury - 508CLNDocument29 pagesNational Survey of Long-Haul Truck Driver Health and Injury - 508CLNBilal Karim KhanNo ratings yet
- Nephrology 7E 2016 PDFDocument2,710 pagesNephrology 7E 2016 PDFĐàoTrườngGiangNo ratings yet
- Fatima Exam QuestionsDocument15 pagesFatima Exam QuestionsPisay Shehannah Grail MedinaNo ratings yet
- Introduction To The Principles and Concepts of Hygiene and Environmental HealthDocument24 pagesIntroduction To The Principles and Concepts of Hygiene and Environmental HealthHimanshu GoelNo ratings yet
- Health Teaching PlanDocument9 pagesHealth Teaching PlanJulianne B. Dela CruzNo ratings yet
- Maritime Declaration of HealthDocument1 pageMaritime Declaration of Healthalive2flirt100% (1)
- Beat Tonsil BookDocument19 pagesBeat Tonsil BookXheni MeleNo ratings yet
- The Management of Cigarette Addiction and Its Impact Among Grade 12 EIM Students of ICIDocument19 pagesThe Management of Cigarette Addiction and Its Impact Among Grade 12 EIM Students of ICICHARLIE ABOTANIONo ratings yet
- All Types of Doctors-PRINTDocument62 pagesAll Types of Doctors-PRINTvinod bhadakeNo ratings yet
- Edlphc2014a by TladiDocument508 pagesEdlphc2014a by Tladiabubakr fingerNo ratings yet
- Assisting A Patient With Ambulation Using A Walker: Page 1/2Document2 pagesAssisting A Patient With Ambulation Using A Walker: Page 1/2Mac Cristian A. CaraganNo ratings yet
- AQ4PDocument3 pagesAQ4PAhmed GaberNo ratings yet
- Orar Sem IiDocument4 pagesOrar Sem IiOlivér CsákNo ratings yet
- VaccinesDocument11 pagesVaccinesZora DNo ratings yet