You might also like
- Action PlanDocument2 pagesAction PlanThalia PacamalanNo ratings yet
- Respiratory Physiology Lab ReportDocument15 pagesRespiratory Physiology Lab ReportThalia PacamalanNo ratings yet
- QuizletDocument3 pagesQuizletThalia PacamalanNo ratings yet
- Respiratory Physiology Lab ReportDocument15 pagesRespiratory Physiology Lab ReportThalia PacamalanNo ratings yet
- Conclusion: (Absorbance of Sample/absorbance of Standard) X Concentration of Standard Concentration of SampleDocument1 pageConclusion: (Absorbance of Sample/absorbance of Standard) X Concentration of Standard Concentration of SampleThalia PacamalanNo ratings yet
- Biochem Trans9 LipidsDocument4 pagesBiochem Trans9 LipidsThalia PacamalanNo ratings yet
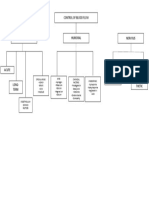
- Control of Blood FlowDocument1 pageControl of Blood FlowThalia PacamalanNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Pathophysiology Model MCQDocument3 pagesPathophysiology Model MCQPrince Xavier100% (1)
- LESSON PLAN in SCIENCE 6 RecoveredDocument4 pagesLESSON PLAN in SCIENCE 6 RecoveredApril Grace Genobatin BinayNo ratings yet
- Ontario - Schedule of Benefits 2021Document970 pagesOntario - Schedule of Benefits 2021Raj LoganathanNo ratings yet
- Reg B - 01 - PPT Anatomy and Physiology of BledderDocument10 pagesReg B - 01 - PPT Anatomy and Physiology of BledderElda FanizahNo ratings yet
- SonoAce - R7 - Reference Manual - EDocument230 pagesSonoAce - R7 - Reference Manual - EEcomedical PlussNo ratings yet
- The Pelvis: Assignment OnDocument40 pagesThe Pelvis: Assignment OnSubhada GosaviNo ratings yet
- Renal Physiology PDFDocument12 pagesRenal Physiology PDFLolitaNo ratings yet
- What Is The Parasympathetic Nervous SystemDocument2 pagesWhat Is The Parasympathetic Nervous Systemjmplayschords100% (2)
- Nervous SystemDocument94 pagesNervous Systemmr pcNo ratings yet
- Atlas Hematologi - Sandoz HariyadiDocument145 pagesAtlas Hematologi - Sandoz HariyadiAnna100% (3)
- Hemodynamic Disorders: BY Dr. Birhane H (MD)Document88 pagesHemodynamic Disorders: BY Dr. Birhane H (MD)Biruck BirhanuNo ratings yet
- The Human Heart: Learner's Book Pg. # 8-9Document17 pagesThe Human Heart: Learner's Book Pg. # 8-9hareem FatimaNo ratings yet
- Identify The Choice That Best Completes The Statement or Answers The QuestionDocument14 pagesIdentify The Choice That Best Completes The Statement or Answers The QuestionCamille BaybayNo ratings yet
- Compatibility Testing: Week 5Document33 pagesCompatibility Testing: Week 5Bridgette100% (1)
- Human Circulatory SystemDocument3 pagesHuman Circulatory SystemMir Rehan Mushtaq100% (1)
- Family Case Study 1Document12 pagesFamily Case Study 1Mark Anthony Torcino AbianNo ratings yet
- Platelets-Composition, Function, Hemostasis and Its Individual PhasesDocument14 pagesPlatelets-Composition, Function, Hemostasis and Its Individual PhasesHebsiba PonnayyanNo ratings yet
- Unit IX Lecture NotesDocument4 pagesUnit IX Lecture NotesSteve Sullivan100% (2)
- Summative Test No. 2 ScienceDocument3 pagesSummative Test No. 2 ScienceMelissa Favila PanagaNo ratings yet
- Techniques in Neuroanatomical ResearchDocument404 pagesTechniques in Neuroanatomical ResearchVlad TomaNo ratings yet
- Anatomy and Physiology of The Cardiovascular SystemDocument6 pagesAnatomy and Physiology of The Cardiovascular SystemDawn Santiago RNNo ratings yet
- MilliwaysDocument12 pagesMilliwaysTurtle ArtNo ratings yet
- IMS - Immunomodulation & ImmunodeficienciesDocument3 pagesIMS - Immunomodulation & ImmunodeficienciesJeanne RodiñoNo ratings yet
- Animal Kingdom - Part 1.ppsxDocument59 pagesAnimal Kingdom - Part 1.ppsxShiyan Shirani0% (1)
- Breathing and Exchange of GasesDocument3 pagesBreathing and Exchange of GasesMaahika MitraNo ratings yet
- Comparison Chart of Gram +ve & - VeDocument2 pagesComparison Chart of Gram +ve & - Veسيفل إسلامNo ratings yet
- HINANAY SSG 4 Antepartum CareDocument4 pagesHINANAY SSG 4 Antepartum CareHenie Louise HinanayNo ratings yet
- Case StudyDocument52 pagesCase Studykennedy1434475% (4)
- Sliding Filament Model of ContractionDocument3 pagesSliding Filament Model of ContractionRATU ZULFI AMALIAHNo ratings yet
- Grade 12mainDocument7 pagesGrade 12mainDoris LiNo ratings yet