You might also like
- 01 Drug File MHNDocument29 pages01 Drug File MHNamit85% (13)
- Drug Study - CefuroximeDocument1 pageDrug Study - Cefuroximewindstruck88% (26)
- Steth OgraphyDocument13 pagesSteth Ographyshahidkhan 6543216543210% (1)
- Color Reactions of CarbohydrateDocument3 pagesColor Reactions of CarbohydrateRifat Ues SayeedNo ratings yet
- Practical 5: ENZYMES AND DIGESTIONDocument12 pagesPractical 5: ENZYMES AND DIGESTIONhafizah_9071% (7)
- DPT Colleges of PakistanDocument24 pagesDPT Colleges of PakistanAli Bin AsimNo ratings yet
- Simple Method of Acid Base Balance InterpretationDocument11 pagesSimple Method of Acid Base Balance InterpretationChin ChanNo ratings yet
- Lab Report On Blood PressureDocument2 pagesLab Report On Blood PressureToni Calsado50% (2)
- Case Scenarios 3rd Yr Head NursingDocument5 pagesCase Scenarios 3rd Yr Head NursingBianca MaeNo ratings yet
- Respiratory Physiology Lab ReportDocument15 pagesRespiratory Physiology Lab ReportThalia PacamalanNo ratings yet
- Pulmonary Function TestsDocument1 pagePulmonary Function Testsprecious_n143No ratings yet
- StethographyDocument3 pagesStethographyglad mohesh100% (4)
- RespirationDocument29 pagesRespirationbemina jaNo ratings yet
- Water Borne Diseases: Summyia Siddique (PT) MSCPPTDocument17 pagesWater Borne Diseases: Summyia Siddique (PT) MSCPPThfyfvgskfajNo ratings yet
- Exercise Metabolism PathwaysDocument31 pagesExercise Metabolism PathwaysHelmi RaisNo ratings yet
- LAB - Lung CapacityDocument5 pagesLAB - Lung CapacityWinnie LeeNo ratings yet
- Toxicology Coverage Midterm Exam PDFDocument17 pagesToxicology Coverage Midterm Exam PDFNestor BargioNo ratings yet
- Dr. Niranjan Murthy H.L Assistant Professor Dept of Physiology SSMCDocument37 pagesDr. Niranjan Murthy H.L Assistant Professor Dept of Physiology SSMCnirilib100% (2)
- 7 VisionDocument4 pages7 VisionZei RuhanoNo ratings yet
- Biochemistry JD 2Document6 pagesBiochemistry JD 2failinNo ratings yet
- Chemical CalculationsDocument3 pagesChemical CalculationsAri AdiantariNo ratings yet
- Medical Ionization: Iontophoresis DR - Saira DDocument22 pagesMedical Ionization: Iontophoresis DR - Saira DAnonymous -No ratings yet
- Lab TechnicianDocument33 pagesLab TechnicianNadeem MughalNo ratings yet
- Pharmacology Solved 2Document2 pagesPharmacology Solved 2Thoby Mlelwa100% (1)
- IMS MCQ Bank 2023Document28 pagesIMS MCQ Bank 2023Abdulrahman AlharbiNo ratings yet
- Glycogen Storage DiseaseDocument19 pagesGlycogen Storage DiseaseRold Brio SosNo ratings yet
- Lab Safety Hazards and Water Purity TestsDocument22 pagesLab Safety Hazards and Water Purity TestsSamuvelrajNo ratings yet
- Maintaining Normal PH Through BuffersDocument40 pagesMaintaining Normal PH Through BuffersRJ Noor JanNo ratings yet
- Titrimetric Methods for Quantitative Chemical AnalysisDocument13 pagesTitrimetric Methods for Quantitative Chemical AnalysisArnoWelgemoedNo ratings yet
- Determination of Sulphate Exp No: 9 Date AimDocument2 pagesDetermination of Sulphate Exp No: 9 Date AimkuthappadyNo ratings yet
- MCQ 23 Physio AnswersDocument8 pagesMCQ 23 Physio AnswersJulyhathul Kuraishi100% (1)
- Talent Management Case Studies NokiaDocument1 pageTalent Management Case Studies NokiakamsudhakarbalaNo ratings yet
- The Acid Base Balance: Faculty of Medicine Anesthesia and Intensive Care DepartmentDocument36 pagesThe Acid Base Balance: Faculty of Medicine Anesthesia and Intensive Care DepartmentCamelia A. ParuschiNo ratings yet
- Lab Report PDDocument17 pagesLab Report PDhaikalNo ratings yet
- UntitledDocument8 pagesUntitledYou TuberNo ratings yet
- Demonstration of The Reflex Pathway in FrogsDocument12 pagesDemonstration of The Reflex Pathway in FrogsRuwiniRajakarunaNo ratings yet
- Experiment 2 Titration of Amino AcidsDocument27 pagesExperiment 2 Titration of Amino AcidsjeromeNo ratings yet
- Abg Analysis ReviewerDocument21 pagesAbg Analysis ReviewerAyiessa_AJNo ratings yet
- Pharmacology (Intro-Drug Calculation)Document46 pagesPharmacology (Intro-Drug Calculation)May Chelle ErazoNo ratings yet
- Dermatological PharmacologyDocument53 pagesDermatological PharmacologyDesta BelachewNo ratings yet
- Glycogenesis: DR Nazakat HussainDocument16 pagesGlycogenesis: DR Nazakat HussainMuhammad Jamal100% (1)
- Case Histo PDFDocument19 pagesCase Histo PDFsomayya waliNo ratings yet
- Lab 04-Cardiovascular PhysiologyDocument18 pagesLab 04-Cardiovascular PhysiologyWilson CheungNo ratings yet
- Hydrochloric Acid VS: Methyl Red Solution Dissolve 50 MG ofDocument3 pagesHydrochloric Acid VS: Methyl Red Solution Dissolve 50 MG ofrina mediana100% (1)
- Pharmacology: Drugs That Affect The: Nervous SystemDocument84 pagesPharmacology: Drugs That Affect The: Nervous SystemSameh Saber100% (1)
- Osmolarity vs OsmolalityDocument13 pagesOsmolarity vs OsmolalityBurhan HameedNo ratings yet
- General Chemistry Laboratory Manual: Yildiz Technical University Faculty of Art & Science Chemistry DepartmentDocument36 pagesGeneral Chemistry Laboratory Manual: Yildiz Technical University Faculty of Art & Science Chemistry DepartmentLOLONo ratings yet
- Lab Report Exp.6Document8 pagesLab Report Exp.6Qj B PdkhNo ratings yet
- Disorders of Potassium Metabolism: Causes, Manifestations and Management (KOMAHS 3rd Year Medicine 9200Document20 pagesDisorders of Potassium Metabolism: Causes, Manifestations and Management (KOMAHS 3rd Year Medicine 9200Solomon Fallah Foa SandyNo ratings yet
- (BIO 024) LAB ACTIVITY 7 - ENZYMESDocument3 pages(BIO 024) LAB ACTIVITY 7 - ENZYMESAlyanna CamarilloNo ratings yet
- Kidney Regulation of Osmolarity - How the Kidneys Control Salt and Water LevelsDocument4 pagesKidney Regulation of Osmolarity - How the Kidneys Control Salt and Water LevelsYoyo WuNo ratings yet
- Arterial Blood Gas Case Questions and AnswersDocument7 pagesArterial Blood Gas Case Questions and AnswersWaqas QureshiNo ratings yet
- Red Blood Cell CountDocument4 pagesRed Blood Cell CountMohamed MokhtarNo ratings yet
- Biochem Reviewer FinalsDocument18 pagesBiochem Reviewer Finalscha cuteNo ratings yet
- #3 Pancreatic Hormones & Antidiabetic Drugs 14 PDFDocument14 pages#3 Pancreatic Hormones & Antidiabetic Drugs 14 PDFOmar BasimNo ratings yet
- Respiratory Failure PresentationDocument13 pagesRespiratory Failure PresentationHusnain Irshad AlviNo ratings yet
- Glycolysis and TCA CycleDocument45 pagesGlycolysis and TCA Cycleshakila786No ratings yet
- Role of Kidney in Acid Base BalanceDocument3 pagesRole of Kidney in Acid Base BalanceSirisha CkvNo ratings yet
- Introduction To Pathology: Sunilkumar.P Haematology & Transfusion Medicine ST - John's Medical College Hospital BangaloreDocument39 pagesIntroduction To Pathology: Sunilkumar.P Haematology & Transfusion Medicine ST - John's Medical College Hospital BangalorefahdabdNo ratings yet
- Sports PhysiologyDocument3 pagesSports PhysiologyCLEMENTNo ratings yet
- Handbook of Endocrine Research TechniquesFrom EverandHandbook of Endocrine Research TechniquesFlora de PabloNo ratings yet
- Week 10 Lab Exercise 9 Respiratory System PhysiologyDocument5 pagesWeek 10 Lab Exercise 9 Respiratory System PhysiologySetnami DhulNo ratings yet
- LabDocument6 pagesLabapi-462581208No ratings yet
- AbdomenDocument1 pageAbdomenThalia PacamalanNo ratings yet
- Action PlanDocument2 pagesAction PlanThalia PacamalanNo ratings yet
- Abdomen ANATLABDocument92 pagesAbdomen ANATLABThalia PacamalanNo ratings yet
- Calcium PDFDocument7 pagesCalcium PDFThalia PacamalanNo ratings yet
- PhysioguytonDocument5 pagesPhysioguytonThalia PacamalanNo ratings yet
- QuizletDocument3 pagesQuizletThalia PacamalanNo ratings yet
- QuizletDocument3 pagesQuizletThalia PacamalanNo ratings yet
- LipidsDocument16 pagesLipidsThalia PacamalanNo ratings yet
- Lipids Classification and FunctionsDocument4 pagesLipids Classification and FunctionsThalia PacamalanNo ratings yet
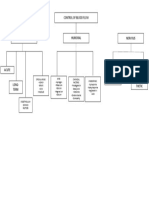
- Control of blood flow through local, humoral and nervous factorsDocument1 pageControl of blood flow through local, humoral and nervous factorsThalia PacamalanNo ratings yet
- Conclusion: (Absorbance of Sample/absorbance of Standard) X Concentration of Standard Concentration of SampleDocument1 pageConclusion: (Absorbance of Sample/absorbance of Standard) X Concentration of Standard Concentration of SampleThalia PacamalanNo ratings yet
- Cartilage His ToDocument4 pagesCartilage His ToThalia PacamalanNo ratings yet
- Meda QantasDocument12 pagesMeda QantasAviasiNo ratings yet
- Dashe 2013Document5 pagesDashe 2013Nữ Vương Nguyễn TrầnNo ratings yet
- Osteoporosis Clinical Case by SlidesgoDocument30 pagesOsteoporosis Clinical Case by SlidesgoHussein Al-jmrawiNo ratings yet
- El DSM-5-TR Un Análisis 101. Una Revisión Ejecutiva Completa de Los Espectros Clasificados en El Manual Diagnóstico y Estadístico de Los Trastornos Mentales, Quinta Edición, Revisión Del Texto - Scientia Media GroupDocument454 pagesEl DSM-5-TR Un Análisis 101. Una Revisión Ejecutiva Completa de Los Espectros Clasificados en El Manual Diagnóstico y Estadístico de Los Trastornos Mentales, Quinta Edición, Revisión Del Texto - Scientia Media GroupHenry RuedaNo ratings yet
- Worksheet 1 (Before Lec 1) PDFDocument4 pagesWorksheet 1 (Before Lec 1) PDFLei Zaira BiendimaNo ratings yet
- Case Based Discussion Astma Bronchiale, Hypertension: Chusna Helmia 01.209.5853Document26 pagesCase Based Discussion Astma Bronchiale, Hypertension: Chusna Helmia 01.209.5853helmiaNo ratings yet
- Supraglottic Airways in Difficult Airway Management: Successes, Failures, Use and MisuseDocument12 pagesSupraglottic Airways in Difficult Airway Management: Successes, Failures, Use and Misusejangkrik21No ratings yet
- Download Clinical Psychopharmacology Principles And Practice 1St Edition S Nassir Ghaemi full chapterDocument67 pagesDownload Clinical Psychopharmacology Principles And Practice 1St Edition S Nassir Ghaemi full chapterdoug.wiggins940100% (4)
- ScriptDocument3 pagesScriptVictoria Dinio FernandoNo ratings yet
- Status EpilepticusDocument22 pagesStatus EpilepticusVivi Kristiani RumapeaNo ratings yet
- Thyroid DiseasesDocument44 pagesThyroid DiseasesPLDT HOMENo ratings yet
- Characteristics of Functional Shoulder InstabilityDocument11 pagesCharacteristics of Functional Shoulder InstabilityOla BochniakNo ratings yet
- Emrcp CNS 38-62Document22 pagesEmrcp CNS 38-62dryusufsNo ratings yet
- LEC 1 Microbiology Intro and Hx. Lec 1Document62 pagesLEC 1 Microbiology Intro and Hx. Lec 1nicewanNo ratings yet
- The Twelve Salts and Some of Their Keynote SymptomsDocument2 pagesThe Twelve Salts and Some of Their Keynote Symptomstaichi7No ratings yet
- L5 - Nature of Clinical Lab - PMLS1Document98 pagesL5 - Nature of Clinical Lab - PMLS1John Daniel AriasNo ratings yet
- CP For Eye NurseDocument3 pagesCP For Eye NursemelanNo ratings yet
- Fetal DistressDocument49 pagesFetal DistressLenny SucalditoNo ratings yet
- Pilocarpine Eye DropDocument3 pagesPilocarpine Eye DropSidahmed SiDo BouchenakNo ratings yet
- Reca Op Claim Form 12-11-0Document25 pagesReca Op Claim Form 12-11-0Ehren OertellNo ratings yet
- Abnormal Labor. BBBB WWPPTXDocument53 pagesAbnormal Labor. BBBB WWPPTXHamss Ahmed100% (2)
- Pediatrics Question PaperDocument21 pagesPediatrics Question Paperprinceej100% (3)
- Clinical Report of DR. Md. Murshidul Ahsan On E.coli & SalmonellaDocument51 pagesClinical Report of DR. Md. Murshidul Ahsan On E.coli & SalmonellamurshidvetNo ratings yet
- Nursing Care PlanDocument10 pagesNursing Care PlanSittie Rohaina SabanNo ratings yet
- 2016 Guidelines For The Management of Thyroid Storm From Japan Thyroid AssociationDocument40 pages2016 Guidelines For The Management of Thyroid Storm From Japan Thyroid AssociationMartha RosanaNo ratings yet
- Methods of Specimen Collection For Diagnosis of Superficial and Subcutaneous Fungal InfectionsDocument5 pagesMethods of Specimen Collection For Diagnosis of Superficial and Subcutaneous Fungal InfectionssaadmcsNo ratings yet
- Childhood Trauma:Impact On Personality/Role in Personality DisordersDocument13 pagesChildhood Trauma:Impact On Personality/Role in Personality DisordersNancee Y.No ratings yet
- Blood TransfusionDocument5 pagesBlood TransfusionCla67% (3)