You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Pa Q Technical ManualDocument68 pagesPa Q Technical ManualZia MalikNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- All AWS - CodesDocument11 pagesAll AWS - CodesPradip Tapan BanerjeeNo ratings yet
- Biochem Trans9 LipidsDocument4 pagesBiochem Trans9 LipidsThalia PacamalanNo ratings yet
- NFJPIA - Mockboard 2011 - MAS PDFDocument7 pagesNFJPIA - Mockboard 2011 - MAS PDFAbigail Faye RoxasNo ratings yet
- Foundations of Commutative Rings and Their ModulesDocument711 pagesFoundations of Commutative Rings and Their ModulesAntonio Torres Peña100% (1)
- Vibration of Hydro Units in HPP - VladislavlevDocument352 pagesVibration of Hydro Units in HPP - VladislavlevDouglas Barros VelozoNo ratings yet
- 610 SIdata SheetsDocument26 pages610 SIdata Sheetssjois_hsNo ratings yet
- VP Engineering CTO in San Francisco Bay CA Resume Ahmed EzzatDocument3 pagesVP Engineering CTO in San Francisco Bay CA Resume Ahmed EzzatAhmedEzzat2No ratings yet
- Action PlanDocument2 pagesAction PlanThalia PacamalanNo ratings yet
- Respiratory Physiology Lab ReportDocument15 pagesRespiratory Physiology Lab ReportThalia PacamalanNo ratings yet
- QuizletDocument3 pagesQuizletThalia PacamalanNo ratings yet
- Respiratory Physiology Lab ReportDocument15 pagesRespiratory Physiology Lab ReportThalia PacamalanNo ratings yet
- Conclusion: (Absorbance of Sample/absorbance of Standard) X Concentration of Standard Concentration of SampleDocument1 pageConclusion: (Absorbance of Sample/absorbance of Standard) X Concentration of Standard Concentration of SampleThalia PacamalanNo ratings yet
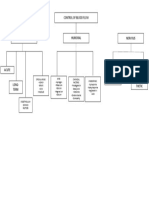
- Control of Blood FlowDocument1 pageControl of Blood FlowThalia PacamalanNo ratings yet
- Cat19579-Tachometer Cable PDFDocument1 pageCat19579-Tachometer Cable PDFshahrol effendy rodziNo ratings yet
- Missay Lesson Plan in Mathematics Guide For Your Lesson Plan Incase of NothingDocument9 pagesMissay Lesson Plan in Mathematics Guide For Your Lesson Plan Incase of Nothingangel shopNo ratings yet
- The Crashing Ventilated Patient Algorthm (Jairo I. Santanilla, ACEP, 2011)Document1 pageThe Crashing Ventilated Patient Algorthm (Jairo I. Santanilla, ACEP, 2011)PkernNo ratings yet
- SAFE Analysis & Design Report: License #C85Document16 pagesSAFE Analysis & Design Report: License #C85Antonysamy SanthanamNo ratings yet
- Diff Conc ManagersDocument34 pagesDiff Conc ManagersMuhd QNo ratings yet
- Material HPLCDocument19 pagesMaterial HPLCIsmil ImamaNo ratings yet
- Choked Flow of FluidsDocument4 pagesChoked Flow of FluidsEnrique VineNo ratings yet
- Quick Response Technique For Travel Demand Estimation in SmallDocument26 pagesQuick Response Technique For Travel Demand Estimation in SmallMonalisa GadpalliwarNo ratings yet
- 2140705Document3 pages21407059922116408No ratings yet
- Controlling Reheat Steam Temperature in Once Through BoilersDocument8 pagesControlling Reheat Steam Temperature in Once Through Boilersபிரசன்னகுமார் ஆனந்தன்No ratings yet
- En Tia L: ASM1061 Data SheetDocument19 pagesEn Tia L: ASM1061 Data Sheetjmbernal7487886No ratings yet
- Series 2400 Fiberglass Pipe and Fittings: Using Key-Lock Mechanical Joint or Taper/ Taper Adhesive JointDocument7 pagesSeries 2400 Fiberglass Pipe and Fittings: Using Key-Lock Mechanical Joint or Taper/ Taper Adhesive JointChristian UhreNo ratings yet
- High Commitment HR SystemsDocument50 pagesHigh Commitment HR Systemsshwetauttam0056296No ratings yet
- SQL QUERIES For Railway Reservation ProgramDocument10 pagesSQL QUERIES For Railway Reservation ProgramSowmya MNo ratings yet
- Swing ProgrammingDocument28 pagesSwing ProgrammingHoang Tuan KhanhNo ratings yet
- MD 2 FinalsDocument43 pagesMD 2 FinalsRea RebenqueNo ratings yet
- Assignment 2 NLP 20bci7108Document2 pagesAssignment 2 NLP 20bci7108rupa sreeNo ratings yet
- Log PDFDocument16 pagesLog PDFRovic James A. DuyanNo ratings yet
- JEE Main 2019 Answer Key Maths Shift 1 Career Point 10th JanDocument4 pagesJEE Main 2019 Answer Key Maths Shift 1 Career Point 10th JanAryan GoelNo ratings yet
- Answer StepExercise Min EOLDocument2 pagesAnswer StepExercise Min EOLKamal SaravananNo ratings yet
- Fire Fighting Robotic Vehicle: Project OnDocument25 pagesFire Fighting Robotic Vehicle: Project OnRuman Guha NiyogiNo ratings yet