You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Multiple Sclerosis Nursing Care PlanDocument4 pagesMultiple Sclerosis Nursing Care PlanCHRISTIE MONTANONo ratings yet
- Ch01 Medical Surgical NursingDocument8 pagesCh01 Medical Surgical Nursingmicky1121100% (1)
- Nursing Care Plan Case PreDocument3 pagesNursing Care Plan Case PreKhatzky MeiNo ratings yet
- Estradiol 10mcg (Vagifen)Document13 pagesEstradiol 10mcg (Vagifen)asdwasdNo ratings yet
- Speech Text - Mental HealthDocument2 pagesSpeech Text - Mental Healthjohnny suhNo ratings yet
- Living WillDocument3 pagesLiving WillBalkiss TouzriNo ratings yet
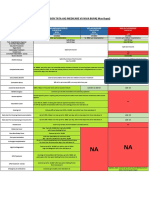
- Comparison Tata Aig Medicare Vs Niva BupaDocument1 pageComparison Tata Aig Medicare Vs Niva BupaTikekar ShubhamNo ratings yet
- 5 PPT Tle 7 Week 5Document51 pages5 PPT Tle 7 Week 5jerico juarezNo ratings yet
- Covid 19Document31 pagesCovid 19Lee BuelaNo ratings yet
- Learner's Activity Sheet: MAPEH Physical Education (Quarter I - Week 1)Document4 pagesLearner's Activity Sheet: MAPEH Physical Education (Quarter I - Week 1)She Ena Man UelNo ratings yet
- Punjab Healthcare Commission: CG-09RM-Ed2Document168 pagesPunjab Healthcare Commission: CG-09RM-Ed2saimaNo ratings yet
- What Can We Eat After Tooth ExtractionDocument4 pagesWhat Can We Eat After Tooth Extractionkings furyNo ratings yet
- Referat Rontgen Thorax Dan KelainannyaDocument31 pagesReferat Rontgen Thorax Dan KelainannyawindarhyngtysNo ratings yet
- EMJ EthicsReviewAAU AdamuDocument9 pagesEMJ EthicsReviewAAU AdamuJateni joteNo ratings yet
- Benign Paroxysmal Positional Vertigo (BPPV) - A Simple SolutionDocument5 pagesBenign Paroxysmal Positional Vertigo (BPPV) - A Simple SolutionagniosaiNo ratings yet
- PreeclampsiaDocument13 pagesPreeclampsiaAnamikaNo ratings yet
- Intake Form: Health Declaration For TravellersDocument1 pageIntake Form: Health Declaration For TravellersHekiXamNo ratings yet
- Chapter 01: Drug Regulation, Actions, and Responses Workman & Lacharity: Understanding Pharmacology: Essentials For Medication Safety, 2Nd EditionDocument13 pagesChapter 01: Drug Regulation, Actions, and Responses Workman & Lacharity: Understanding Pharmacology: Essentials For Medication Safety, 2Nd Editionleo chenNo ratings yet
- BHW Pocket HandbookDocument70 pagesBHW Pocket HandbookGa B B Orlongan100% (9)
- Form F Tule DOWNSDocument2 pagesForm F Tule DOWNSAnand ChineyNo ratings yet
- Chapter 5 Challenge Solution: Project Management FoundationsDocument2 pagesChapter 5 Challenge Solution: Project Management FoundationspraveenNo ratings yet
- Mini-PAT Paper Form - Updated June 18Document2 pagesMini-PAT Paper Form - Updated June 18Benjamin NgNo ratings yet
- Viral ShahDocument2 pagesViral ShahAkshay ShahNo ratings yet
- Research India - Google ScholarDocument1 pageResearch India - Google Scholarritesh jadhavNo ratings yet
- Dehydration in ChildrenDocument24 pagesDehydration in ChildrenDani AsmareNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanJoyce AnglubenNo ratings yet
- San Cristobal Elementary School School Clinic LogbookDocument3 pagesSan Cristobal Elementary School School Clinic LogbookLhenzky BernarteNo ratings yet
- 100 Item Exam On Fundamentals of Nursing - Pulse - Blood Pressure PDFDocument12 pages100 Item Exam On Fundamentals of Nursing - Pulse - Blood Pressure PDFJawad AkbarNo ratings yet
- NCPDocument4 pagesNCPDivine TejadaNo ratings yet
- Varicose VeinsDocument25 pagesVaricose VeinsByancaPredescu50% (2)