You might also like
- Credit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!From EverandCredit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!Rating: 1 out of 5 stars1/5 (1)
- A Beginner's Guide to Disability Insurance Claims in Canada: How to Apply for and Win Payment of Disability Insurance Benefits, Even After a Denial or Unsuccessful AppealFrom EverandA Beginner's Guide to Disability Insurance Claims in Canada: How to Apply for and Win Payment of Disability Insurance Benefits, Even After a Denial or Unsuccessful AppealNo ratings yet
- CHRA Reviewer 3Document15 pagesCHRA Reviewer 3Zaila Mitch100% (3)
- Anthem Dental Enrollment Enrollment Form 2014Document2 pagesAnthem Dental Enrollment Enrollment Form 2014Tanveer ShaikhNo ratings yet
- Health Questionnaire Form (HQF)Document1 pageHealth Questionnaire Form (HQF)salmanNo ratings yet
- What You Should Know Before Applying for SSDIDocument6 pagesWhat You Should Know Before Applying for SSDIkruno.grubesicNo ratings yet
- Connectors Linking Words - 61564Document1 pageConnectors Linking Words - 61564Jhon Edwar Fierro GonzalezNo ratings yet
- EDD UI BenefitsDocument9 pagesEDD UI Benefitsalex kapelNo ratings yet
- Get the Job with ConfidenceDocument4 pagesGet the Job with ConfidenceJesstoni CaniedoNo ratings yet
- Chapter - V The Legality of Strike: (1910) I KBP 506. (1949) LLJ 796 (I.T.)Document53 pagesChapter - V The Legality of Strike: (1910) I KBP 506. (1949) LLJ 796 (I.T.)Manish SinghNo ratings yet
- Employee Claim: A. Your Information (Employee)Document6 pagesEmployee Claim: A. Your Information (Employee)dratiffaridNo ratings yet
- Total and Permanent Disability Claim FormDocument2 pagesTotal and Permanent Disability Claim FormPrashob SugathanNo ratings yet
- Documents Form Medical Claim Il PDFDocument4 pagesDocuments Form Medical Claim Il PDFAnonymous isUyKYK1zwNo ratings yet
- Employees Retirement System of Texas Texas Employees Group Benefits Program (GBP) Evidence of Insurability (EOI) Application Active/Retired EmployeesDocument5 pagesEmployees Retirement System of Texas Texas Employees Group Benefits Program (GBP) Evidence of Insurability (EOI) Application Active/Retired EmployeesCarroll MixsonNo ratings yet
- Charity Care Application EnglishDocument7 pagesCharity Care Application EnglishDavidNo ratings yet
- Welcome To Blue Cross and Blue Shield of Illinois and Fort Dearborn LifeDocument6 pagesWelcome To Blue Cross and Blue Shield of Illinois and Fort Dearborn LifeBuy BaNo ratings yet
- Jawad Claim FormDocument2 pagesJawad Claim FormJawad KarimNo ratings yet
- Ci Benefits Rights InformationDocument15 pagesCi Benefits Rights InformationBladimir LoraNo ratings yet
- OSHA C-2 FormDocument6 pagesOSHA C-2 Formjuda823No ratings yet
- Domestic Maid Claim FormDocument4 pagesDomestic Maid Claim FormHihiNo ratings yet
- Application Form InsightsDocument5 pagesApplication Form InsightsPoi HHNo ratings yet
- Sukshma Hospi CashDocument4 pagesSukshma Hospi CashAdemuyiwa OlaniyiNo ratings yet
- BSIB GHS Claim FormDocument3 pagesBSIB GHS Claim FormmuhsinmohammedNo ratings yet
- Proof of Loss Form for Study USA HealthCareDocument2 pagesProof of Loss Form for Study USA HealthCareborn2bewildNo ratings yet
- Beacon Health Claim Form PDFDocument2 pagesBeacon Health Claim Form PDFcvasurNo ratings yet
- Guide For Receiving UI Benefits: Privacy Act StatementDocument13 pagesGuide For Receiving UI Benefits: Privacy Act StatementPackdaddyNo ratings yet
- GLOC Health Claim Form Fillable Form NewDocument2 pagesGLOC Health Claim Form Fillable Form NewRyanRamroopNo ratings yet
- Whats AppDocument3 pagesWhats AppmargeliscamargoNo ratings yet
- CIBenefitsRightsInformation BILLIECASEBIER-727202007224240Document15 pagesCIBenefitsRightsInformation BILLIECASEBIER-727202007224240BILLIE CASEBIERNo ratings yet
- Proposal Form New India Floater Mediclaim Policy-1Document7 pagesProposal Form New India Floater Mediclaim Policy-1Hemraj SonarNo ratings yet
- Bajaj Allianz Critical Care Proposal FormDocument3 pagesBajaj Allianz Critical Care Proposal FormAlina Fatma0% (1)
- Ci Benefits Rights InformationDocument15 pagesCi Benefits Rights Informationjuanchy12No ratings yet
- Claims Form For New India AssuranceDocument2 pagesClaims Form For New India AssuranceRafael BlackNo ratings yet
- Step 1 Packet NEW PDFDocument6 pagesStep 1 Packet NEW PDFPrabhjot KaurNo ratings yet
- Proposal Form Ashakiran PDFDocument6 pagesProposal Form Ashakiran PDFSreejith Rajendran PillaiNo ratings yet
- G B A S A P 1 4: IVE ACK Mile Pplication AGE OFDocument4 pagesG B A S A P 1 4: IVE ACK Mile Pplication AGE OFcancermoonwolfNo ratings yet
- 5star Family Protection Plan: Term Life Insurance To Age 100 ApplicationDocument2 pages5star Family Protection Plan: Term Life Insurance To Age 100 Applicationimi_swimNo ratings yet
- Claim FormDocument3 pagesClaim FormKhameer L Shah100% (1)
- Dol 5158 PUADocument2 pagesDol 5158 PUArsl.rexxNo ratings yet
- Entire Packet 10Document7 pagesEntire Packet 10JohnnyLarsonNo ratings yet
- Consumer Complaint FormDocument2 pagesConsumer Complaint Formnalgonda365No ratings yet
- NAIC Claim Form PDFDocument3 pagesNAIC Claim Form PDFMohit BaggaNo ratings yet
- Crewsure Claim Form (XLCatlin) 1.3Document2 pagesCrewsure Claim Form (XLCatlin) 1.3Andrei Belehuzi0% (1)
- WireWheel Short Term DisabilityDocument7 pagesWireWheel Short Term DisabilitySteve MooreNo ratings yet
- Aviva Pharmacist Liability Insurance Application 1Document3 pagesAviva Pharmacist Liability Insurance Application 1Anat HershkovitzNo ratings yet
- NTUC Claim FormDocument5 pagesNTUC Claim FormHihiNo ratings yet
- UCCA Application For Admission Form 3Document2 pagesUCCA Application For Admission Form 3Akinlabi HendricksNo ratings yet
- Shared Work Continued Claim Waiting Week Certification: Part A - Employee StatementDocument2 pagesShared Work Continued Claim Waiting Week Certification: Part A - Employee StatementKler KerNo ratings yet
- NSTUMP - Proposal FormDocument7 pagesNSTUMP - Proposal FormJagadeesh MaheshNo ratings yet
- Kutumb Swasthya Bima Policy - GroupDocument4 pagesKutumb Swasthya Bima Policy - Grouprohit kakkarNo ratings yet
- National Inurance Company Limited - Claim FormDocument3 pagesNational Inurance Company Limited - Claim FormfuckyouprettyNo ratings yet
- ICICI - Claim FormDocument5 pagesICICI - Claim FormRaja RamanNo ratings yet
- Accident Suraksha Claim FormDocument4 pagesAccident Suraksha Claim FormKeval ShahNo ratings yet
- Doctor's Indemnity Proposal FormDocument5 pagesDoctor's Indemnity Proposal FormPriyank guptaNo ratings yet
- UIBenefit Rights InformationDocument14 pagesUIBenefit Rights InformationNeeraj Singh RainaNo ratings yet
- NSESAF1 - New Style Employment and Supprt Allowance PDFDocument23 pagesNSESAF1 - New Style Employment and Supprt Allowance PDFEllie JeanNo ratings yet
- How To File PUA Application en 20200428Document7 pagesHow To File PUA Application en 20200428DustinNo ratings yet
- CI Benefits Rights InformationDocument15 pagesCI Benefits Rights Informationchris johnNo ratings yet
- Individual Characteristics Form (ICF) Work Opportunity Tax CreditDocument4 pagesIndividual Characteristics Form (ICF) Work Opportunity Tax CreditThembie DubeNo ratings yet
- ESI Declaration FormDocument3 pagesESI Declaration FormSourav SarkarNo ratings yet
- JF Elite Plus Student Insurance Claim Form: ImportantDocument2 pagesJF Elite Plus Student Insurance Claim Form: ImportantJayesh GoplaniNo ratings yet
- Form 6Document4 pagesForm 6ReidSchneiderNo ratings yet
- SA-8000 AwarenessDocument18 pagesSA-8000 AwarenessAsu AsuNo ratings yet
- Innovative and Modern Human Resource Practices in Indian BanksDocument6 pagesInnovative and Modern Human Resource Practices in Indian BanksSamba BahNo ratings yet
- Bangladesh labor laws overviewDocument3 pagesBangladesh labor laws overviewShazedul Haque RadhitNo ratings yet
- Beware of The "End Contractualization!" Battle Cry: Vicente B. Paqueo and Aniceto C. Orbeta JRDocument16 pagesBeware of The "End Contractualization!" Battle Cry: Vicente B. Paqueo and Aniceto C. Orbeta JRMarck GoNo ratings yet
- Human ResourceDocument13 pagesHuman ResourceK Memcha SinghaNo ratings yet
- Coca-Cola HBC's Commitment to Human RightsDocument3 pagesCoca-Cola HBC's Commitment to Human RightsAvani ShitoleNo ratings yet
- Oathtaking ProgramDocument3 pagesOathtaking ProgramnurseoncervixNo ratings yet
- Construction Laborer Job <40Document3 pagesConstruction Laborer Job <40yahia3fathy-965095No ratings yet
- Human Resource ManagementDocument22 pagesHuman Resource ManagementEmebet TesemaNo ratings yet
- Job Security & SatisfactionDocument8 pagesJob Security & Satisfactionyousuf AhmedNo ratings yet
- Data For Accident: (Refer Table 3)Document6 pagesData For Accident: (Refer Table 3)aminNo ratings yet
- Airtel ComplianceDocument1 pageAirtel ComplianceDhananjay BhedaNo ratings yet
- Oracle HRMS Daywise Schedule and Topic GuideDocument1 pageOracle HRMS Daywise Schedule and Topic GuidesekharbynaNo ratings yet
- Chapter 9 Performance Management and AppraisalDocument41 pagesChapter 9 Performance Management and Appraisalbachtiar ibnuNo ratings yet
- NBCUniversal MCoC & Post Audit Acceptance EnglishDocument2 pagesNBCUniversal MCoC & Post Audit Acceptance Englishholistic foodNo ratings yet
- OvertimeDocument2 pagesOvertimeMarla BarbotNo ratings yet
- The Relationship Between Motivation and Organizational BehaviorDocument3 pagesThe Relationship Between Motivation and Organizational Behavioradam100% (1)
- BAR Q Salaries Part 1Document3 pagesBAR Q Salaries Part 1RVirayNo ratings yet
- Sr HR Executive Recruitment Malayalam CochinDocument26 pagesSr HR Executive Recruitment Malayalam CochinAjay PCNo ratings yet
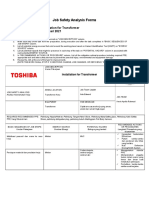
- Job Safety Analysis Forms: Job/Task: Installation For Transformer Date: 9 Januari 2021Document3 pagesJob Safety Analysis Forms: Job/Task: Installation For Transformer Date: 9 Januari 2021Akhli RohmatulohNo ratings yet
- Contract Labour R A Act 1970Document71 pagesContract Labour R A Act 1970Harshit ShrivastavaNo ratings yet
- Introduction To HRMDocument46 pagesIntroduction To HRMisraelNo ratings yet
- Performance Task 4Th Quarter Scaffold No. 1Document5 pagesPerformance Task 4Th Quarter Scaffold No. 1MayaNo ratings yet
- Labour Standards Code: Guide To The Nova ScotiaDocument47 pagesLabour Standards Code: Guide To The Nova ScotiaJohn SuttonNo ratings yet
- Management Unit 5 MCQ Test (Legislative Acts)Document7 pagesManagement Unit 5 MCQ Test (Legislative Acts)Sanika ShindeNo ratings yet
- Improving The Welfare of Gig Workers in IndiaDocument14 pagesImproving The Welfare of Gig Workers in IndiaawardanbhimawatNo ratings yet
- MBA 509-1 HRM Lecture 1 IUB FinalDocument35 pagesMBA 509-1 HRM Lecture 1 IUB FinalMd. Muhinur Islam AdnanNo ratings yet