You might also like
- Chic, Elegant, and Fun 3D Eiffel Tower Sticker Scene: Lined Personal Journal, Diary, & Notebook | Wide-RuleFrom EverandChic, Elegant, and Fun 3D Eiffel Tower Sticker Scene: Lined Personal Journal, Diary, & Notebook | Wide-RuleNo ratings yet
- Budgeting For Clinical TrialsDocument30 pagesBudgeting For Clinical TrialsArun NairNo ratings yet
- Resolution 128 and Supporting DocumentsDocument3 pagesResolution 128 and Supporting DocumentsCurtisNo ratings yet
- Pet Insurance ComparisonsDocument2 pagesPet Insurance ComparisonsHSVC50% (2)
- Kaiser Permanente California Plans and Benefits Brochure KPIF 2011Document6 pagesKaiser Permanente California Plans and Benefits Brochure KPIF 2011DennisNo ratings yet
- ConvertDocument2 pagesConvertpham_thu_hangNo ratings yet
- 2022 Benefits Summary For FA EE'sDocument6 pages2022 Benefits Summary For FA EE'sFrancisca VigilNo ratings yet
- Marjorie Bse 4a EconomicsDocument25 pagesMarjorie Bse 4a Economics062691No ratings yet
- CVS Caremark Pricing InformationDocument2 pagesCVS Caremark Pricing Informationalex.goldschmidt5521No ratings yet
- 2021 THNM Individual Health PlansDocument1 page2021 THNM Individual Health PlansSara SnowNo ratings yet
- Plan ComparisonDocument2 pagesPlan ComparisonSahil JindalNo ratings yet
- Ppto Australia R03 PDFDocument1 pagePpto Australia R03 PDFMichael CastrillónNo ratings yet
- Eye Med SummaryDocument2 pagesEye Med SummaryparthaNo ratings yet
- Excel ApplicationDocument2 pagesExcel Applicationapi-381460003No ratings yet
- FOCA Compensation ChartDocument1 pageFOCA Compensation ChartprojectcurveappealNo ratings yet
- Ms Out of Pocket Protection RatesDocument2 pagesMs Out of Pocket Protection Ratesapi-425909885No ratings yet
- Faculty of Management Science: Name: Fazil Ahmed Sec: B STUDENT ID: (27-2019)Document6 pagesFaculty of Management Science: Name: Fazil Ahmed Sec: B STUDENT ID: (27-2019)fazil ahmedNo ratings yet
- Cs Plus NYC Area Epo 2q 2009Document1 pageCs Plus NYC Area Epo 2q 2009KristieNo ratings yet
- Grant BudgetDocument6 pagesGrant Budgetapi-354983120No ratings yet
- Personal Budget WordDocument4 pagesPersonal Budget Wordapi-353822671No ratings yet
- Simple Annual BudgetDocument2 pagesSimple Annual BudgetPedro FreitasNo ratings yet
- Budget For I Love Coffee Shop Pty LTD in 2022 (Financial Year)Document6 pagesBudget For I Love Coffee Shop Pty LTD in 2022 (Financial Year)Shefali GoyalNo ratings yet
- Proposed 2022 Fee Schedule For Detroit LakesDocument7 pagesProposed 2022 Fee Schedule For Detroit LakesMichael AchterlingNo ratings yet
- Medical Comparison Chart 2020Document3 pagesMedical Comparison Chart 2020hollingermikeNo ratings yet
- Terrell and Terrell Property Management 1960 Wellington Avenue-DuplexDocument11 pagesTerrell and Terrell Property Management 1960 Wellington Avenue-DuplexVishwa PatelNo ratings yet
- HCOs Variances SolDocument3 pagesHCOs Variances SolSimon OllyNo ratings yet
- 1 Nathan Schwartz Ucf Forecast Sheets Canvas - 1Document2 pages1 Nathan Schwartz Ucf Forecast Sheets Canvas - 1api-624802175No ratings yet
- Costs According To RegionsDocument1 pageCosts According To RegionsFernando G. OrozcoNo ratings yet
- Net After Tax Rate of Return 2018Document1 pageNet After Tax Rate of Return 2018cherry LiNo ratings yet
- Benefits Highlights 2018Document5 pagesBenefits Highlights 2018Marcus CosmeNo ratings yet
- Personal BudgetDocument2 pagesPersonal Budgetapi-417329934No ratings yet
- Untitled Spreadsheet-3Document3 pagesUntitled Spreadsheet-3api-434964251No ratings yet
- Taimoor Shahzad 265100 ME10D EE Assignment 01Document3 pagesTaimoor Shahzad 265100 ME10D EE Assignment 01Get-Set-GoNo ratings yet
- Costs 2Document1 pageCosts 2Fernando G. OrozcoNo ratings yet
- Personal Budget Template: Expenses 37%Document10 pagesPersonal Budget Template: Expenses 37%CarloNo ratings yet
- OriginalDocument36 pagesOriginalXiaochen TangNo ratings yet
- Ch. 6. Answers To Review Questions (See Task 2)Document3 pagesCh. 6. Answers To Review Questions (See Task 2)mohamed yNo ratings yet
- PHP T2 P VZDDocument1 pagePHP T2 P VZDNATSOIncNo ratings yet
- Sensitivity SlideDocument4 pagesSensitivity SlideIan TanNo ratings yet
- Fill Y According To X Fill Y According To XDocument14 pagesFill Y According To X Fill Y According To XAgna AegeanNo ratings yet
- EyeMed Benefit Plan SummaryDocument2 pagesEyeMed Benefit Plan SummaryNestor Fabian Bermudez ZuletaNo ratings yet
- Unit 4 AssignmentDocument3 pagesUnit 4 Assignmentwriter post100% (1)
- Profit & Loss For Kami's Clothing As at 2018Document3 pagesProfit & Loss For Kami's Clothing As at 2018Veer SinghNo ratings yet
- Msla Business FeesDocument1 pageMsla Business FeesNBC MontanaNo ratings yet
- Cost Analysis & Staffing Plan for Medical ClinicDocument1 pageCost Analysis & Staffing Plan for Medical ClinicemilyanncrNo ratings yet
- My Income Chart: Expenses and SavingsDocument1 pageMy Income Chart: Expenses and SavingsJessica AningatNo ratings yet
- Inflation AssignmentDocument2 pagesInflation Assignmentaneeshbadola01No ratings yet
- Simple Personal Budget1Document2 pagesSimple Personal Budget1I Gede Rai SudanaNo ratings yet
- Nuevo MenúPGDocument4 pagesNuevo MenúPGEduardo HernandezNo ratings yet
- Niva TravelAssure Students SS v6Document2 pagesNiva TravelAssure Students SS v6Sam JejNo ratings yet
- Track Personal Cash Flow with This Monthly Budget TemplateDocument2 pagesTrack Personal Cash Flow with This Monthly Budget TemplatejoytoriolsantiagoNo ratings yet
- Ch9 - Cengage 2, 4, 6, 8, 10, 12, 14Document5 pagesCh9 - Cengage 2, 4, 6, 8, 10, 12, 14Apdev OptionNo ratings yet
- TareaDocument1 pageTareaEdgar TorresNo ratings yet
- Group Critical Illness Insurance CoverageDocument2 pagesGroup Critical Illness Insurance CoverageAndrewNo ratings yet
- Coaching prices 2023 One-pagerDocument1 pageCoaching prices 2023 One-pagerMukuka MbeweNo ratings yet
- Project BudgetDocument1 pageProject Budgetapi-246873879No ratings yet
- Budget For 100 Conventional BroilersDocument3 pagesBudget For 100 Conventional BroilersMary Jessah LumbabNo ratings yet
- Project staffing and costs breakdownDocument2 pagesProject staffing and costs breakdownHeriberto Hernandez RodriguezNo ratings yet
- Trading Journal NOV2020Document95 pagesTrading Journal NOV2020Antonio AndradeNo ratings yet
- Property & Liability Renewal ComparisonDocument58 pagesProperty & Liability Renewal Comparisonpalanisamy744100% (1)
- Asian RapDocument2 pagesAsian RapTitoNo ratings yet
- WWE® To Adjourn Annual Meeting For Third Time Due To COVID-19 ConcernsDocument2 pagesWWE® To Adjourn Annual Meeting For Third Time Due To COVID-19 ConcernsTitoNo ratings yet
- WWE® Names Nick Khan President & Chief Revenue OfficerDocument2 pagesWWE® Names Nick Khan President & Chief Revenue OfficerTitoNo ratings yet
- WWE® Introduces The New Free Version of WWE® NetworkDocument2 pagesWWE® Introduces The New Free Version of WWE® NetworkTitoNo ratings yet
- WWE® and Discovery Announce New Partnership in ItalyDocument3 pagesWWE® and Discovery Announce New Partnership in ItalyTitoNo ratings yet
- WWE® To Adjourn Annual Meeting For Second Time Due To COVID-19 ConcernsDocument2 pagesWWE® To Adjourn Annual Meeting For Second Time Due To COVID-19 ConcernsTitoNo ratings yet
- WWE® Announces Adjournment and Change of Format of 2020 Annual Meeting of StockholdersDocument2 pagesWWE® Announces Adjournment and Change of Format of 2020 Annual Meeting of StockholdersTitoNo ratings yet
- WWE® Names Kristina Salen Chief Financial OfficerDocument2 pagesWWE® Names Kristina Salen Chief Financial OfficerTitoNo ratings yet
- WWE® Brings The ThunderDocument2 pagesWWE® Brings The ThunderTitoNo ratings yet
- WWE® Declares Quarterly DividendDocument2 pagesWWE® Declares Quarterly DividendTitoNo ratings yet
- WWE® Elects Erika Nardini To Board of DirectorsDocument2 pagesWWE® Elects Erika Nardini To Board of DirectorsTitoNo ratings yet
- WWE® Elects Steve Pamon To Board of DirectorsDocument2 pagesWWE® Elects Steve Pamon To Board of DirectorsTitoNo ratings yet
- WWE® To Report Second Quarter 2020 ResultsDocument2 pagesWWE® To Report Second Quarter 2020 ResultsTitoNo ratings yet
- WWE® Reports Strong Second Quarter 2020 Results Driven by Sustained Cost SavingsDocument12 pagesWWE® Reports Strong Second Quarter 2020 Results Driven by Sustained Cost SavingsTitoNo ratings yet
- Undertaker®'s Final Farewell Set For WWE® Survivor Series®Document2 pagesUndertaker®'s Final Farewell Set For WWE® Survivor Series®TitoNo ratings yet
- WWE® To Report Third Quarter 2020 ResultsDocument2 pagesWWE® To Report Third Quarter 2020 ResultsTitoNo ratings yet
- WWE® Declares Quarterly DividendDocument2 pagesWWE® Declares Quarterly DividendTitoNo ratings yet
- WWE® Names Karen Mullane Controller & Chief Accounting OfficerDocument2 pagesWWE® Names Karen Mullane Controller & Chief Accounting OfficerTitoNo ratings yet
- WWE® Reports Strong Third Quarter 2020 ResultsDocument11 pagesWWE® Reports Strong Third Quarter 2020 ResultsTitoNo ratings yet
- 18th Annual WWE® Tribute To The Troops® To Air On FOXDocument3 pages18th Annual WWE® Tribute To The Troops® To Air On FOXTitoNo ratings yet
- WWE® ThunderDome™ Takes Over Tropicana FieldDocument2 pagesWWE® ThunderDome™ Takes Over Tropicana FieldTitoNo ratings yet
- q2 2019 Earnings Website PresentationDocument16 pagesq2 2019 Earnings Website PresentationTitoNo ratings yet
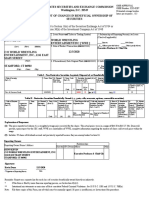
- WWE SEC FilingDocument2 pagesWWE SEC FilingTitoNo ratings yet
- q4 and Fy 2018 Earnings Website Presentation Vfinal PDFDocument19 pagesq4 and Fy 2018 Earnings Website Presentation Vfinal PDFTitoNo ratings yet
- Wwe Presentation 11 30 18 PDFDocument40 pagesWwe Presentation 11 30 18 PDFTitoNo ratings yet
- WWE Q1 2019 Results Drive Future GrowthDocument17 pagesWWE Q1 2019 Results Drive Future GrowthTitoNo ratings yet
- SFASU - Film and Culture SyllabusDocument8 pagesSFASU - Film and Culture SyllabusTitoNo ratings yet
- Wwe Presentation 7 28 18Document41 pagesWwe Presentation 7 28 18vikasNo ratings yet
- q4 and Fy 2018 Earnings Website Presentation Vfinal PDFDocument19 pagesq4 and Fy 2018 Earnings Website Presentation Vfinal PDFTitoNo ratings yet
- Wwe Investor Presentation 05 29 18 Fy2017 PDFDocument41 pagesWwe Investor Presentation 05 29 18 Fy2017 PDFTitoNo ratings yet
- SO311222Document25 pagesSO311222Fiqri RismainiNo ratings yet
- Dr. P S Adhya 7186Document1 pageDr. P S Adhya 7186Partha AdhyaNo ratings yet
- EBBA Delegation 2019Document3 pagesEBBA Delegation 2019jina morganNo ratings yet
- Muskuloskeletal Disorder Menggunakan: Analisa Dan Penilaian Risiko Metode Manual Tasks Risk Assessment (Mantra)Document8 pagesMuskuloskeletal Disorder Menggunakan: Analisa Dan Penilaian Risiko Metode Manual Tasks Risk Assessment (Mantra)Dirgntra AlanNo ratings yet
- Booklet - EpfpclDocument9 pagesBooklet - EpfpclAnonymous G5Od0CTrmeNo ratings yet
- Indian Cookware and Home Decor Product CatalogDocument31 pagesIndian Cookware and Home Decor Product CatalogSuraj PramanikNo ratings yet
- Trophy Winners 2019Document10 pagesTrophy Winners 2019blackguard999No ratings yet
- Handbook AdhesiveDocument68 pagesHandbook Adhesivec100% (2)
- Seoul International Invention Fair 2019Document2 pagesSeoul International Invention Fair 2019Mohammad Nuh Al-hudawy SiraitNo ratings yet
- CH 5 - Cyprus RestaurantDocument15 pagesCH 5 - Cyprus RestaurantmazenfarhatNo ratings yet
- Intro To Psychology Crash Course Psychology 1Document3 pagesIntro To Psychology Crash Course Psychology 1Hahaha YeahNo ratings yet
- Reviewer Ansc 111Document6 pagesReviewer Ansc 111Jeric MadroñoNo ratings yet
- ReptileDocument4 pagesReptileDratonius 101No ratings yet
- Imogene Martina KingDocument7 pagesImogene Martina KingJoanna Marie TulioNo ratings yet
- Topic 3 BRUNEI The Oilfields LabourersDocument3 pagesTopic 3 BRUNEI The Oilfields LabourersRichmond BlancoNo ratings yet
- BAslam - Kassimali Matrix - Analysis - of - StructureDocument123 pagesBAslam - Kassimali Matrix - Analysis - of - StructureAmitabha ChakrabortyNo ratings yet
- Molykote: 111 CompoundDocument2 pagesMolykote: 111 CompoundEcosuministros ColombiaNo ratings yet
- Trix Price List OCT 2018 PDFDocument2 pagesTrix Price List OCT 2018 PDFApNo ratings yet
- Tie Systems: The Right Solution For All Wall Formwork: Waterproof Gas-Proof Fire Resistant Soundproof Radiation-ProofDocument16 pagesTie Systems: The Right Solution For All Wall Formwork: Waterproof Gas-Proof Fire Resistant Soundproof Radiation-Proofidesawy1982No ratings yet
- The Yale-Brown Obsessive Compulsive Scale I. Development, Use, and ReliabilityDocument6 pagesThe Yale-Brown Obsessive Compulsive Scale I. Development, Use, and Reliabilitynurulhafizhah01No ratings yet
- School Form 2 Daily Attendance Report of Learners For Senior High School (SF2-SHS)Document2 pagesSchool Form 2 Daily Attendance Report of Learners For Senior High School (SF2-SHS)Charly Mint Atamosa IsraelNo ratings yet
- HIST2601 HSienaDocument6 pagesHIST2601 HSienaQuinn HarringtonNo ratings yet
- Blood Componant Therapy (Autosaved)Document47 pagesBlood Componant Therapy (Autosaved)drkapiltNo ratings yet
- Gang Violence in Jamaica: Causes, Effects and SolutionsDocument20 pagesGang Violence in Jamaica: Causes, Effects and SolutionsRicardoMoody50% (2)
- A Beginner's Guide To Pig FarmingDocument87 pagesA Beginner's Guide To Pig FarmingIdada EzekielNo ratings yet
- Fmea - Failure Mode Effect AnalysisDocument23 pagesFmea - Failure Mode Effect AnalysisAsawari JoshiNo ratings yet
- EER WorksheetDocument3 pagesEER WorksheetMichael PoddubnyNo ratings yet
- 6 Review of Related LiteratureDocument2 pages6 Review of Related Literaturerusty0% (2)
- Tupad Orientation Presentation 2017Document54 pagesTupad Orientation Presentation 2017Anonymous EvbW4o1U7100% (5)
- CALIMOVEDocument46 pagesCALIMOVERasheedAladdinNGuiomala0% (1)
- Breaking the Habit of Being YourselfFrom EverandBreaking the Habit of Being YourselfRating: 4.5 out of 5 stars4.5/5 (1456)
- The Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerFrom EverandThe Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerRating: 4.5 out of 5 stars4.5/5 (58)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipFrom EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipRating: 4.5 out of 5 stars4.5/5 (1135)
- Deep Sleep Meditation: Fall Asleep Instantly with Powerful Guided Meditations, Hypnosis, and Affirmations. Overcome Anxiety, Depression, Insomnia, Stress, and Relax Your Mind!From EverandDeep Sleep Meditation: Fall Asleep Instantly with Powerful Guided Meditations, Hypnosis, and Affirmations. Overcome Anxiety, Depression, Insomnia, Stress, and Relax Your Mind!Rating: 4.5 out of 5 stars4.5/5 (10)
- Summary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissFrom EverandSummary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissRating: 4.5 out of 5 stars4.5/5 (81)
- Really Very Crunchy: A Beginner's Guide to Removing Toxins from Your Life without Adding Them to Your PersonalityFrom EverandReally Very Crunchy: A Beginner's Guide to Removing Toxins from Your Life without Adding Them to Your PersonalityRating: 5 out of 5 stars5/5 (27)
- The Stress-Proof Brain: Master Your Emotional Response to Stress Using Mindfulness and NeuroplasticityFrom EverandThe Stress-Proof Brain: Master Your Emotional Response to Stress Using Mindfulness and NeuroplasticityRating: 4.5 out of 5 stars4.5/5 (109)
- Chair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouFrom EverandChair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouRating: 3.5 out of 5 stars3.5/5 (5)
- 369: Manifesting Through 369 and the Law of Attraction - METHODS, TECHNIQUES AND EXERCISESFrom Everand369: Manifesting Through 369 and the Law of Attraction - METHODS, TECHNIQUES AND EXERCISESRating: 5 out of 5 stars5/5 (50)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Creation Frequency: Tune In to the Power of the Universe to Manifest the Life of Your DreamsFrom EverandThe Creation Frequency: Tune In to the Power of the Universe to Manifest the Life of Your DreamsRating: 5 out of 5 stars5/5 (549)
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomFrom EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomRating: 4 out of 5 stars4/5 (1)
- Allen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductFrom EverandAllen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductRating: 5 out of 5 stars5/5 (31)
- Deep Sleep Hypnosis: Guided Meditation For Sleep & HealingFrom EverandDeep Sleep Hypnosis: Guided Meditation For Sleep & HealingRating: 4.5 out of 5 stars4.5/5 (103)
- Boundless: Upgrade Your Brain, Optimize Your Body & Defy AgingFrom EverandBoundless: Upgrade Your Brain, Optimize Your Body & Defy AgingRating: 4.5 out of 5 stars4.5/5 (66)
- Allen Carr's Easy Way for Women to Lose Weight: The original Easyway methodFrom EverandAllen Carr's Easy Way for Women to Lose Weight: The original Easyway methodRating: 4.5 out of 5 stars4.5/5 (18)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisFrom EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisRating: 3 out of 5 stars3/5 (2)
- Bedtime Stories for Adults: Tales to Soothe the Tired SoulsFrom EverandBedtime Stories for Adults: Tales to Soothe the Tired SoulsRating: 4 out of 5 stars4/5 (3)
- The Ikigai Journey: A Practical Guide to Finding Happiness and Purpose the Japanese WayFrom EverandThe Ikigai Journey: A Practical Guide to Finding Happiness and Purpose the Japanese WayRating: 5 out of 5 stars5/5 (27)
- The Self-Care Solution: A Year of Becoming Happier, Healthier, and Fitter—One Month at a TimeFrom EverandThe Self-Care Solution: A Year of Becoming Happier, Healthier, and Fitter—One Month at a TimeRating: 3 out of 5 stars3/5 (5)
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeFrom EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeRating: 3.5 out of 5 stars3.5/5 (13)
- Midnight Meditations: Calm Your Thoughts, Still Your Body, and Return to SleepFrom EverandMidnight Meditations: Calm Your Thoughts, Still Your Body, and Return to SleepRating: 5 out of 5 stars5/5 (2)
- The Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingFrom EverandThe Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingRating: 4 out of 5 stars4/5 (3)
- Glucose Revolution: The Life-Changing Power of Balancing Your Blood SugarFrom EverandGlucose Revolution: The Life-Changing Power of Balancing Your Blood SugarRating: 5 out of 5 stars5/5 (349)