You might also like
- Photon Benefits SummaryDocument7 pagesPhoton Benefits SummarysojithesouljaNo ratings yet
- 2022 Steven Charles BAG - CODocument4 pages2022 Steven Charles BAG - COAlejuanchis Kamacho GarciaNo ratings yet
- Trevor Kernan - LifeHappensDocument3 pagesTrevor Kernan - LifeHappensTrevor KernanNo ratings yet
- Pet Insurance ComparisonsDocument2 pagesPet Insurance ComparisonsHSVC50% (2)
- Plan ComparisonDocument4 pagesPlan Comparisontth79hj4dvNo ratings yet
- Your Customized Benefits Plan at HCL America IncDocument2 pagesYour Customized Benefits Plan at HCL America IncShiv RanjanNo ratings yet
- Projected Budget Spreadsheet 1Document10 pagesProjected Budget Spreadsheet 1Ismail UsmanNo ratings yet
- Budget Overview: Actual vs Projected ExpensesDocument6 pagesBudget Overview: Actual vs Projected Expensesivan.breNo ratings yet
- Family Budget (Monthly) 1Document6 pagesFamily Budget (Monthly) 1Naddie DeoreNo ratings yet
- Kaiser Permanente Compare Plans CA 2011 KPIFDocument1 pageKaiser Permanente Compare Plans CA 2011 KPIFDennis AlexanderNo ratings yet
- 2023 Talent BAAGDocument3 pages2023 Talent BAAGThi HanNo ratings yet
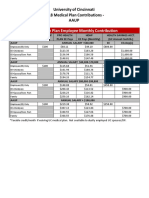
- 2018 Benefit Cost Aaup All FinalDocument2 pages2018 Benefit Cost Aaup All FinalStacy JohnsonNo ratings yet
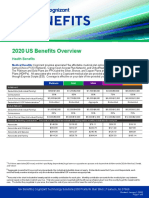
- 2020 US Benefits OverviewDocument5 pages2020 US Benefits OverviewrdmNo ratings yet
- 2010 UnitedHealthcare Benefits SummaryDocument1 page2010 UnitedHealthcare Benefits Summaryapi-27017317No ratings yet
- 2020 Rate Sheet - DiversifiedDocument2 pages2020 Rate Sheet - Diversifiedrobin floydNo ratings yet
- Summary of 2022 Benefit Changes: MedicalDocument5 pagesSummary of 2022 Benefit Changes: MedicalChinnu SalimathNo ratings yet
- 2017 Employee Benefit Highlights - Support StaffDocument8 pages2017 Employee Benefit Highlights - Support StaffJohn AcardoNo ratings yet
- M2A1 US Census Data SearchDocument6 pagesM2A1 US Census Data SearchragcajunNo ratings yet
- Plan ComparisonDocument2 pagesPlan ComparisonSahil JindalNo ratings yet
- Medical Comparison Chart 2020Document3 pagesMedical Comparison Chart 2020hollingermikeNo ratings yet
- Sbo - Health Insurance Rates Fy17.18Document1 pageSbo - Health Insurance Rates Fy17.18maria31691No ratings yet
- Budget DefenseDocument19 pagesBudget Defenseapi-687516998No ratings yet
- Benefits Overview 2018Document5 pagesBenefits Overview 2018Joby JoNo ratings yet
- Generic Open Enrollment KitDocument22 pagesGeneric Open Enrollment KitSteve BarrowsNo ratings yet
- Kaiser Permanente California Plans and Benefits Brochure KPIF 2011Document6 pagesKaiser Permanente California Plans and Benefits Brochure KPIF 2011DennisNo ratings yet
- Personal Budget & Finances (Sheida)Document5 pagesPersonal Budget & Finances (Sheida)Dana NimriNo ratings yet
- Harmonic ScalpelDocument2 pagesHarmonic ScalpelHerman HalimNo ratings yet
- Personal Budget Spreadsheet 10 2020-2 2Document4 pagesPersonal Budget Spreadsheet 10 2020-2 2api-685542779No ratings yet
- HA ZONE-Ben Cov Details PlanComp-EnglishApril12019DDocument4 pagesHA ZONE-Ben Cov Details PlanComp-EnglishApril12019DGilad RozenbergNo ratings yet
- SeKON Employee Benefits Summary 2016Document3 pagesSeKON Employee Benefits Summary 2016Ali HajassdolahNo ratings yet
- 2023+FMCNA+Medical+Plan+Cost+ComparisonDocument2 pages2023+FMCNA+Medical+Plan+Cost+ComparisonCristal PeoplesNo ratings yet
- Monthly Budget WorksheetDocument2 pagesMonthly Budget Worksheetapi-534083600No ratings yet
- 2010 UHC Medical Plan ComparisonDocument2 pages2010 UHC Medical Plan Comparisonapi-20618861No ratings yet
- Contribution RatesDocument1 pageContribution Ratesstuart52No ratings yet
- Monthly Family BudgetDocument3 pagesMonthly Family BudgetMohamed ElhousniNo ratings yet
- Applying To Become A NECA MemberDocument4 pagesApplying To Become A NECA MemberMarvin Lucero FiscalNo ratings yet
- Samantha Garcia - Making Money Count - 301133Document2 pagesSamantha Garcia - Making Money Count - 301133api-484500823No ratings yet
- Household Monthly Budget1Document12 pagesHousehold Monthly Budget1kanjulaNo ratings yet
- EmblemHealth Benefits 2019Document7 pagesEmblemHealth Benefits 2019Jorge Luis Rivera AgostoNo ratings yet
- You're AllDocument8 pagesYou're AllSunny BautistaNo ratings yet
- As An Individual, How Much Will I Save On Health Care?: For 1 AdultDocument5 pagesAs An Individual, How Much Will I Save On Health Care?: For 1 AdultBernewsAdminNo ratings yet
- Monthly Budget Analysis Reveals Need to Cut SpendingDocument3 pagesMonthly Budget Analysis Reveals Need to Cut Spendingwbfuller16641No ratings yet
- Household Monthly Budget1Document12 pagesHousehold Monthly Budget1Sujit ChauhanNo ratings yet
- Family Budget (Monthly)Document11 pagesFamily Budget (Monthly)HappyNo ratings yet
- Sdfsef DFG 2345Document10 pagesSdfsef DFG 2345sami senNo ratings yet
- Swera Gresresca 543Document10 pagesSwera Gresresca 543sami senNo ratings yet
- Mrtuine 5643Document10 pagesMrtuine 5643sami senNo ratings yet
- Living On Your OwnDocument1 pageLiving On Your Ownapi-445856493No ratings yet
- Dseerwassvc 123Document10 pagesDseerwassvc 123sami senNo ratings yet
- OfficeSuite BudgetOverviewDocument6 pagesOfficeSuite BudgetOverviewShreyas RamachandranNo ratings yet
- Young Adult BrochureDocument5 pagesYoung Adult BrochureahsanNo ratings yet
- Total Compensation Benefit Summary STMTDocument3 pagesTotal Compensation Benefit Summary STMTlorigross3No ratings yet
- Career BudgetDocument1 pageCareer Budgetapi-435326846No ratings yet
- Test 1Document2 pagesTest 1Christian DeKnockNo ratings yet
- Examining Child Expenditure MethodologiesDocument11 pagesExamining Child Expenditure MethodologiesTony CurtisNo ratings yet
- Choice MVDocument1 pageChoice MVGowell SupportNo ratings yet
- Personal Budgeting Spreadsheet by NeilDocument14 pagesPersonal Budgeting Spreadsheet by NeilHarsh ShahNo ratings yet
- Tailored Tailored Tailored Tailored: UST Global Health Cash PlanDocument4 pagesTailored Tailored Tailored Tailored: UST Global Health Cash PlanManasa KondaNo ratings yet
- Benefits HighlightsDocument1 pageBenefits HighlightsRobert AvramescuNo ratings yet