You might also like
- Dr. Widyati ADR ANALYSIS-PERSIDocument39 pagesDr. Widyati ADR ANALYSIS-PERSIHanaNo ratings yet
- Schizophrenia, the Long View Questions You Should Ask Your 34th Psychiatric Consultation William R. Yee M.D., J.D., Copyright Applied for July 8th, 2022From EverandSchizophrenia, the Long View Questions You Should Ask Your 34th Psychiatric Consultation William R. Yee M.D., J.D., Copyright Applied for July 8th, 2022No ratings yet
- Naranjo AlgorithmDocument1 pageNaranjo AlgorithmIwa PrinandiNo ratings yet
- ADR ScalesDocument4 pagesADR ScalesAnonymous l39lxfzJNo ratings yet
- Drug and Therapeutics Committee: Session 4. Assessing and Managing Medicine SafetyDocument40 pagesDrug and Therapeutics Committee: Session 4. Assessing and Managing Medicine SafetyPratyNo ratings yet
- Pharmacovigilance: Department of Pharmacology and Toxicology, Faculty of PharmacyDocument52 pagesPharmacovigilance: Department of Pharmacology and Toxicology, Faculty of PharmacyNdhy Pharm HabibieNo ratings yet
- ADR Reporting Form for Mesco College of PharmacyDocument1 pageADR Reporting Form for Mesco College of PharmacyMarifuddin HussainiNo ratings yet
- Bookshelf_NBK548069Document5 pagesBookshelf_NBK548069diego.alvarez1No ratings yet
- Naranjo Probability Scale in Drug Induced Liver InjuryDocument5 pagesNaranjo Probability Scale in Drug Induced Liver InjuryArielle Grace PerezNo ratings yet
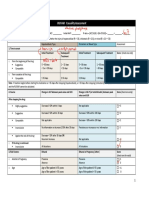
- RUCAM Causality Assessment for Drug-Induced Liver InjuryDocument2 pagesRUCAM Causality Assessment for Drug-Induced Liver Injuryirvan bNo ratings yet
- Livertoxrucamv5 PDFDocument2 pagesLivertoxrucamv5 PDFpokNo ratings yet
- RUCAM Risk ScoreDocument2 pagesRUCAM Risk ScoreStevenNo ratings yet
- Rucam PDFDocument2 pagesRucam PDFmarzinaNo ratings yet
- RUCAM Causality Assessment for Drug-Induced Liver InjuryDocument2 pagesRUCAM Causality Assessment for Drug-Induced Liver Injuryirvan bNo ratings yet
- WHO-UMC Causality CategoriesDocument2 pagesWHO-UMC Causality CategoriesbournvilleeaterNo ratings yet
- Tingkat Signifikansi Kejadian Efek Samping Obat Berdasarkan Skala NaranjoDocument2 pagesTingkat Signifikansi Kejadian Efek Samping Obat Berdasarkan Skala Naranjolab pkmsekolaqNo ratings yet
- NARANJO ALGORITHM ASSESSMENT TOOLDocument18 pagesNARANJO ALGORITHM ASSESSMENT TOOLAubey TanNo ratings yet
- ADR Form AkhDocument2 pagesADR Form Akhsofiasofi191980No ratings yet
- Naranjo AlgorithmDocument3 pagesNaranjo AlgorithmmilkymilkyNo ratings yet
- Liver Support Protocol Introduction GuideDocument9 pagesLiver Support Protocol Introduction GuideВиктория КривошеяNo ratings yet
- Adverse Drug ReactionDocument6 pagesAdverse Drug Reactionpranal patil (Pranal)No ratings yet
- Trigger Tools to Identify Adverse Drug Events (ADEsDocument2 pagesTrigger Tools to Identify Adverse Drug Events (ADEsArvenaa SubramaniamNo ratings yet
- PharmacovigilanceDocument33 pagesPharmacovigilanceAna Sarah KurniaNo ratings yet
- Dizziness and Nausea Vomitting Induced by Ropinirole Therapy in An Elderly Patient With Parkinson's Disease: A Case ReportDocument6 pagesDizziness and Nausea Vomitting Induced by Ropinirole Therapy in An Elderly Patient With Parkinson's Disease: A Case ReportRabiatul AdawiyahNo ratings yet
- Adverse Drug Reactions ADR Classes ADR Reporting ADRDocument37 pagesAdverse Drug Reactions ADR Classes ADR Reporting ADRMahum SohailNo ratings yet
- Clinical Condition and Medication Therapy of AmoxiDocument3 pagesClinical Condition and Medication Therapy of AmoxiRina HerowatiNo ratings yet
- Drug Related Pleural Disease: Charis Moschos MD., Ioannis Kalomenidis MD E-Mail: Ikalom@Document11 pagesDrug Related Pleural Disease: Charis Moschos MD., Ioannis Kalomenidis MD E-Mail: Ikalom@roland helmizarNo ratings yet
- PharmacovigilanceDocument31 pagesPharmacovigilanceapi-381097683% (6)
- NMPHHN280 Module4Document49 pagesNMPHHN280 Module4강소라No ratings yet
- Approved ADR FormatDocument3 pagesApproved ADR Formatinayat.kabirNo ratings yet
- Naranjo Causality ScaleDocument2 pagesNaranjo Causality ScaleZamharira MuslimNo ratings yet
- Risk Factors For Cutaneous Adverse Drug ReactionsDocument26 pagesRisk Factors For Cutaneous Adverse Drug ReactionsMukesh Kumar SharmaNo ratings yet
- CR 1.pdfDocument22 pagesCR 1.pdftyleree3No ratings yet
- Drug Screening Questionnaire DASTDocument2 pagesDrug Screening Questionnaire DASTErin CooperNo ratings yet
- Naranjo Algorithm: QuestionnaireDocument2 pagesNaranjo Algorithm: Questionnaireela ameliaNo ratings yet
- ADR Reporting SystemDocument58 pagesADR Reporting SystemYash DevrukhkarNo ratings yet
- Drug Interactions Reporting FormDocument3 pagesDrug Interactions Reporting FormBREAN -THE LEGENDNo ratings yet
- Southwestern Medical Center Case Presentation: Placental Abruption at 37 WeeksDocument33 pagesSouthwestern Medical Center Case Presentation: Placental Abruption at 37 WeeksChresia Schae MondejarNo ratings yet
- Case Study 47: Antipsychotic Drugs For Schizophrenia: ResultsDocument16 pagesCase Study 47: Antipsychotic Drugs For Schizophrenia: ResultsAngel Rose GeraldeNo ratings yet
- A Changed Alphabet and Neurological ChaosDocument31 pagesA Changed Alphabet and Neurological ChaosBisweswar OjhaNo ratings yet
- Comprehensive Case Study PsychDocument10 pagesComprehensive Case Study Psychapi-593862121No ratings yet
- Causality Assessment: 20 April 2015 Meyler Course 2015 Eugene Van Puijenbroek, MD PHD, Clinical PharmacologistDocument53 pagesCausality Assessment: 20 April 2015 Meyler Course 2015 Eugene Van Puijenbroek, MD PHD, Clinical PharmacologistSabina PetrarNo ratings yet
- Schizophrenia and Other Psychotic Disorders Clinical Practice GuidelineDocument7 pagesSchizophrenia and Other Psychotic Disorders Clinical Practice GuidelineDani NugrohoNo ratings yet
- DrugToxicityCauses,Symptoms,Treatment 1699189975465Document12 pagesDrugToxicityCauses,Symptoms,Treatment 1699189975465pearl ikebuakuNo ratings yet
- K26 - Efek Samping ObatDocument80 pagesK26 - Efek Samping ObatNastiti MaharaniNo ratings yet
- The Inimical Repercussions of Unauthoris PDFDocument5 pagesThe Inimical Repercussions of Unauthoris PDFkaushikthe1No ratings yet
- Drug Card TamifluDocument1 pageDrug Card TamifluAdrianne BazoNo ratings yet
- msfDocument20 pagesmsfAddisNo ratings yet
- Definitions: - Pharmacovigilance - Adverse Event - Adverse ReactionDocument16 pagesDefinitions: - Pharmacovigilance - Adverse Event - Adverse ReactionRamaiyan DhanapalNo ratings yet
- Favipiravir Tablet Manual: Please Read The Instructions Carefully and Use Under The Guidance of A PhysicianDocument4 pagesFavipiravir Tablet Manual: Please Read The Instructions Carefully and Use Under The Guidance of A Physicianchard xuNo ratings yet
- Fluvoxamine for COVID-19: A Potentially Lifesaving TreatmentDocument66 pagesFluvoxamine for COVID-19: A Potentially Lifesaving TreatmentVijay GauravNo ratings yet
- Causality Assessment of ADRsDocument45 pagesCausality Assessment of ADRsKrupasagar Pn PalegarNo ratings yet
- AcetaminophenDocument1 pageAcetaminophenKatie McPeek100% (1)
- NCM106 - Pharmacology: History: Hypersensitivity To Hydantoins, History of SinusDocument2 pagesNCM106 - Pharmacology: History: Hypersensitivity To Hydantoins, History of SinusBrandy RectoNo ratings yet
- Fluoxetine,: Behavioral Side Fluoxetine Children and AdolescentsDocument6 pagesFluoxetine,: Behavioral Side Fluoxetine Children and AdolescentsJulio JuarezNo ratings yet
- The Drug Interaction Probability ScaleDocument1 pageThe Drug Interaction Probability ScaleFina Ahmad Fitriana0% (1)
- MCQs Adult Part 1Document39 pagesMCQs Adult Part 1Ilinca mirnoviciNo ratings yet
- Drugallergydiagnosis: Anca M. Chiriac,, Pascal DemolyDocument11 pagesDrugallergydiagnosis: Anca M. Chiriac,, Pascal DemolyHusni mubarakNo ratings yet
- Chief Complaint: Exam:: Contact With and (Suspected) Exposure To Other Viral Communicable Diseases (V01.79, Z20.828)Document1 pageChief Complaint: Exam:: Contact With and (Suspected) Exposure To Other Viral Communicable Diseases (V01.79, Z20.828)Jayanth BhargavNo ratings yet
- 101MCQsinPharmacology-27 01 2017Document2 pages101MCQsinPharmacology-27 01 2017Ignacio NamuncuraNo ratings yet
- Adverse Effects of Voriconazole Analysis of The FRDocument10 pagesAdverse Effects of Voriconazole Analysis of The FRIgnacio NamuncuraNo ratings yet
- Hiragana Katakana WorksheetDocument23 pagesHiragana Katakana WorksheetAquasu Haisa100% (3)
- ヒューマノイドのBassカバーDocument10 pagesヒューマノイドのBassカバーIgnacio NamuncuraNo ratings yet
- 0897190010388145Document10 pages0897190010388145Ignacio NamuncuraNo ratings yet
- World Health Organization Model List of Essential MedicinesDocument65 pagesWorld Health Organization Model List of Essential MedicineschungNo ratings yet
- Ocular PharmacologyDocument11 pagesOcular PharmacologyIgnacio NamuncuraNo ratings yet
- Table3000CaracteresChinois PDFDocument125 pagesTable3000CaracteresChinois PDFAngelic PangkarayaNo ratings yet
- Stres KerjaDocument25 pagesStres KerjajoniNo ratings yet
- Busqueda BibliograficaDocument5 pagesBusqueda BibliograficaIgnacio NamuncuraNo ratings yet
- Feldman 2015Document20 pagesFeldman 2015Ignacio NamuncuraNo ratings yet
- Ni Hms 29614Document11 pagesNi Hms 29614Ignacio NamuncuraNo ratings yet
- Clin Pharm Consistent Process For Direct Patient Care White Paper PTHX 0814Document16 pagesClin Pharm Consistent Process For Direct Patient Care White Paper PTHX 0814Ignacio NamuncuraNo ratings yet
- How To Learn ChineseDocument47 pagesHow To Learn ChineseWy Teay100% (5)
- Conciliacion IDocument11 pagesConciliacion IIgnacio NamuncuraNo ratings yet
- 2015 Montini - Pharmacist Recommendations in An Intensive CareDocument6 pages2015 Montini - Pharmacist Recommendations in An Intensive CareIgnacio NamuncuraNo ratings yet
- Intensive Care Medicine in 2050: Global Perspectives: EditorialDocument5 pagesIntensive Care Medicine in 2050: Global Perspectives: EditorialIgnacio NamuncuraNo ratings yet
- Drug Regimens Special Populations ICUDocument14 pagesDrug Regimens Special Populations ICUIgnacio NamuncuraNo ratings yet
- Automating Medication Regimen Complexity IndexDocument8 pagesAutomating Medication Regimen Complexity IndexIgnacio NamuncuraNo ratings yet
- 2011 Risk Score To Hospitalized Patients For Clinical Pharmacy RationalizationDocument6 pages2011 Risk Score To Hospitalized Patients For Clinical Pharmacy RationalizationIgnacio NamuncuraNo ratings yet
- CDTM CMM 2015 FinalDocument12 pagesCDTM CMM 2015 FinalIgnacio NamuncuraNo ratings yet
- Scottsbasslessons Slap Lesson PDFDocument1 pageScottsbasslessons Slap Lesson PDFIgnacio NamuncuraNo ratings yet
- ADE Trigger ToolDocument7 pagesADE Trigger ToolIgnacio NamuncuraNo ratings yet
- C C P L U: Ritical ARE Harmacotherapy Iterature PdateDocument9 pagesC C P L U: Ritical ARE Harmacotherapy Iterature PdateIgnacio NamuncuraNo ratings yet
- Bedside Glucose Monitoring Is It Safe A New,.1Document8 pagesBedside Glucose Monitoring Is It Safe A New,.1Ignacio NamuncuraNo ratings yet
- Key Articles and Guidelines Relative To Intensive Care Unit Pharmacotherapy: 2009 UpdateDocument42 pagesKey Articles and Guidelines Relative To Intensive Care Unit Pharmacotherapy: 2009 UpdateIgnacio NamuncuraNo ratings yet
- Caracterizacion de Ade Farmacia ClinicaDocument11 pagesCaracterizacion de Ade Farmacia ClinicaIgnacio NamuncuraNo ratings yet
- UCI Pharmacist RoleDocument6 pagesUCI Pharmacist RoleIgnacio NamuncuraNo ratings yet
- Prehistoric Music History IDocument2 pagesPrehistoric Music History IIgnacio NamuncuraNo ratings yet
- Microteaching: MDR - TBDocument16 pagesMicroteaching: MDR - TBVikram Singh RanawatNo ratings yet
- Medical Laboratory Tests: Tang PingDocument42 pagesMedical Laboratory Tests: Tang Pingapi-19916399No ratings yet
- A A PHN IntroDocument354 pagesA A PHN IntroGabriel PhilippeNo ratings yet
- Pediatric AssessmentDocument54 pagesPediatric AssessmentThetnaungsoeNo ratings yet
- Breach of Duty of CareDocument46 pagesBreach of Duty of CareJavier LimNo ratings yet
- Rehabilitation of A Complex Oro-Facial Defect by Modified Prosthetic ApproachDocument3 pagesRehabilitation of A Complex Oro-Facial Defect by Modified Prosthetic ApproachBharat KhemaniNo ratings yet
- Vital Signs - Measurements of Basic Body FunctionsDocument27 pagesVital Signs - Measurements of Basic Body FunctionsJames Paulo AbandoNo ratings yet
- Patent Ductus ArteriosusDocument49 pagesPatent Ductus Arteriosusarchana vermaNo ratings yet
- Instruction: Select The Correct Answer For Each of The Following Questions. Mark Only One Answer byDocument7 pagesInstruction: Select The Correct Answer For Each of The Following Questions. Mark Only One Answer byEden Marie FranciscoNo ratings yet
- Ep 306 My Notes Correction Za TichaDocument138 pagesEp 306 My Notes Correction Za TichaKhalid khalifaNo ratings yet
- Newborn AssessmentDocument5 pagesNewborn Assessmentapi-503822850No ratings yet
- Introduction To Community B.SC Ii Yr CHNDocument77 pagesIntroduction To Community B.SC Ii Yr CHNJOSEPH IVO A. AGUINALDONo ratings yet
- The First Six Weeks by Midwife Cath (Extract)Document24 pagesThe First Six Weeks by Midwife Cath (Extract)Allen & Unwin14% (7)
- Gestational Diabetes Mellitus - : One Disease Two Lives at StakeDocument31 pagesGestational Diabetes Mellitus - : One Disease Two Lives at StakeSadia YousafNo ratings yet
- Ayurvedic Bhasma PDFDocument9 pagesAyurvedic Bhasma PDFFARIS NATTUKALNo ratings yet
- Annex F - Assessment of Oral Mucosal TissueDocument2 pagesAnnex F - Assessment of Oral Mucosal TissueGowriNo ratings yet
- Learning The Secret LanguageDocument89 pagesLearning The Secret LanguageArzu100% (4)
- Combined Pressure and Flow Measurements To Guide Treatment of Coronary Stenoses PDFDocument10 pagesCombined Pressure and Flow Measurements To Guide Treatment of Coronary Stenoses PDFIsfan RialdyNo ratings yet
- Pushpitakam of Charaka Indriya Sthana - An Explorative StudyDocument9 pagesPushpitakam of Charaka Indriya Sthana - An Explorative StudyPrasad MamidiNo ratings yet
- Guide To Graphene Oxide DetoxDocument5 pagesGuide To Graphene Oxide Detoxeu100% (3)
- Tapescript For Part 2.3Document2 pagesTapescript For Part 2.3Ph DiNo ratings yet
- 2021 - Safe Return To School PlanDocument7 pages2021 - Safe Return To School PlanMicah AmongoNo ratings yet
- Comparison of Kangaroo Mother Care With Conventional Method of Care in The Care of Low Birth Weight InfantsDocument58 pagesComparison of Kangaroo Mother Care With Conventional Method of Care in The Care of Low Birth Weight Infantssunny kumarNo ratings yet
- Home Remedies To Treat Dupuytren S Disease OrthoBethesda .G-Job 84Document15 pagesHome Remedies To Treat Dupuytren S Disease OrthoBethesda .G-Job 84paulsub63No ratings yet
- 8th Circuit Court of AppealsDocument11 pages8th Circuit Court of AppealsGazetteonlineNo ratings yet
- TRN2044095 7939696 Clinical ReportDocument10 pagesTRN2044095 7939696 Clinical ReportWARNET SANTONo ratings yet
- AphasiaDocument13 pagesAphasiaaamirNo ratings yet
- PharmacokineticsDocument95 pagesPharmacokineticsSonalee ShahNo ratings yet
- CHCAGE001Document30 pagesCHCAGE001Vaishali Arora100% (1)
- The Contributions of St. Cyprian: Perspectives On Epidemiology and Early ChristianityDocument15 pagesThe Contributions of St. Cyprian: Perspectives On Epidemiology and Early ChristianityLudimila Caliman CamposNo ratings yet