You might also like
- Categorical Data Analysis Selected Solutions by AgrestiDocument30 pagesCategorical Data Analysis Selected Solutions by AgrestiNeil Bot67% (3)
- The Lex Repetundarum and The Political Ideas of Gaius Gracchus by Sherwin-WhiteDocument15 pagesThe Lex Repetundarum and The Political Ideas of Gaius Gracchus by Sherwin-WhiteMr SazeracNo ratings yet
- Shin 2008 - Kāmarūpa - Region - Formed - and - Imagined - ReconsideringDocument35 pagesShin 2008 - Kāmarūpa - Region - Formed - and - Imagined - ReconsideringVajradharmaNo ratings yet
- James A. Arvites, Irene Woman Emperor of Constantinople, Her Life and TimesDocument175 pagesJames A. Arvites, Irene Woman Emperor of Constantinople, Her Life and TimesGülcanGülyaprakNo ratings yet
- Diuretics - AMBOSS PDFDocument9 pagesDiuretics - AMBOSS PDFOpio Isaac100% (1)
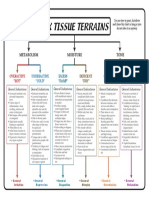
- 6 Tissue Terrains ColorDocument1 page6 Tissue Terrains Colorஆ.க.கோ. இராஜேஷ்வரக் கோன்No ratings yet
- Irving Jennifer 2012. Restituta. The Training of The Female Physician. Melbourne Historical Journal 40. Classical Re-Conceptions, 44-56 PDFDocument13 pagesIrving Jennifer 2012. Restituta. The Training of The Female Physician. Melbourne Historical Journal 40. Classical Re-Conceptions, 44-56 PDFAnonymous 3Z5YxA9pNo ratings yet
- Christians and The Roman Army A.D. 173-337 (John Helgeland)Document17 pagesChristians and The Roman Army A.D. 173-337 (John Helgeland)mallevila100% (1)
- Sinclair Bell, Teresa Ramsby - Free at Last! - The Impact of Freed Slaves On The Roman Empire-Bristol Classical Press (2012)Document225 pagesSinclair Bell, Teresa Ramsby - Free at Last! - The Impact of Freed Slaves On The Roman Empire-Bristol Classical Press (2012)Caslav Nikolic100% (1)
- The Persecution of The Jews in The Roman Empire 300-428Document96 pagesThe Persecution of The Jews in The Roman Empire 300-428Yaakov SiepmanNo ratings yet
- John Forsdyke - Greece Before HomerDocument192 pagesJohn Forsdyke - Greece Before HomerPocho Lapantera100% (2)
- Archaeology and Philology On Mons Claudianus 1987Document12 pagesArchaeology and Philology On Mons Claudianus 1987Łukasz IlińskiNo ratings yet
- Partheon in Aug RomeDocument56 pagesPartheon in Aug RomeJessica BellNo ratings yet
- Brunt (1975) - The Administrators of Roman EgyptDocument25 pagesBrunt (1975) - The Administrators of Roman EgyptJavier S.No ratings yet
- Roman Life and Manners Under The Early EmpireDocument732 pagesRoman Life and Manners Under The Early EmpireFaris Marukic100% (1)
- Doctors As Diplomats in The Sixth Century AD, Blockley 1980Document12 pagesDoctors As Diplomats in The Sixth Century AD, Blockley 1980Toddus AureliusNo ratings yet
- The Summer of Blood. The Great Massacre of 337 and The Promotion of The Sons of ConstantineDocument55 pagesThe Summer of Blood. The Great Massacre of 337 and The Promotion of The Sons of ConstantineMariusz Myjak100% (1)
- Benjamin Isaac - Empire and Ideology in The Graeco-Roman World - Selected Papers-Cambridge University Press (2017)Document380 pagesBenjamin Isaac - Empire and Ideology in The Graeco-Roman World - Selected Papers-Cambridge University Press (2017)ruja_popova1178No ratings yet
- The Role of The Pedagogue in GalatiansDocument19 pagesThe Role of The Pedagogue in Galatians31songofjoy100% (1)
- LollianosDocument28 pagesLollianosFernando PiantanidaNo ratings yet
- The Saga of The Argonauts A Reflex of TH PDFDocument11 pagesThe Saga of The Argonauts A Reflex of TH PDFruja_popova1178No ratings yet
- Dinchev 1999 Classification Late Antique Cities Thracia Dacia PDFDocument39 pagesDinchev 1999 Classification Late Antique Cities Thracia Dacia PDFbobongo9038No ratings yet
- Akarli - The Long Peace - Ottoman LebanonDocument243 pagesAkarli - The Long Peace - Ottoman LebanonvarnamalaNo ratings yet
- (Karen Lee Edwards) Captive Gods Romans and AthenDocument194 pages(Karen Lee Edwards) Captive Gods Romans and AthenRocsana RusinNo ratings yet
- The Sacred GerusiaDocument212 pagesThe Sacred GerusiaEzequiel Rivas100% (1)
- (Medieval Academy Books No. 92.) Kaminsky, Howard - Simon de Cramaud. - de Substraccione Obediencie-Medieval Academy of America (1984) - CópiaDocument262 pages(Medieval Academy Books No. 92.) Kaminsky, Howard - Simon de Cramaud. - de Substraccione Obediencie-Medieval Academy of America (1984) - CópiaLeonardo GeuburNo ratings yet
- Jones Later Roman Empire01Document269 pagesJones Later Roman Empire01Anonymous QHOyMJSrNo ratings yet
- Vol 1Document236 pagesVol 1Jose manuelNo ratings yet
- Orginality Eusebius ChronicleDocument7 pagesOrginality Eusebius ChronicleŞahin KılıçNo ratings yet
- Khatchadourian 2016 Imperial MatterDocument322 pagesKhatchadourian 2016 Imperial MatterAshley BarlowNo ratings yet
- Reinmuth - Praefectus EgyptiDocument85 pagesReinmuth - Praefectus EgyptiSidiropoulos DimitriosNo ratings yet
- Small Greek WorldDocument308 pagesSmall Greek WorlddanielweizmanNo ratings yet
- The Statuary of Asklepios From The Athenian AgoraDocument68 pagesThe Statuary of Asklepios From The Athenian AgoraEve AthanasekouNo ratings yet
- Ancient LibrariesDocument13 pagesAncient Librariesfsultana100% (1)
- Rejecting Catastrophe: The Case of The Justinianic PlagueDocument48 pagesRejecting Catastrophe: The Case of The Justinianic Plaguecarlos murciaNo ratings yet
- The Evolution of Service NobilitiesDocument27 pagesThe Evolution of Service NobilitiesHugo André Flores Fernandes AraújoNo ratings yet
- CRAWFORD How To Create A Municipium Rome and Italy After The Social WarDocument17 pagesCRAWFORD How To Create A Municipium Rome and Italy After The Social WarPablo Varona Rubio100% (1)
- Leo Wiener 1919 - History of Arabico-Gothic Culture (Vol. 2 OCR)Document420 pagesLeo Wiener 1919 - History of Arabico-Gothic Culture (Vol. 2 OCR)Anders FernstedtNo ratings yet
- Cameron, A. - The Exposure of Children and Greek Ethics - CR, 46, 3 - 1932 - 105-114Document11 pagesCameron, A. - The Exposure of Children and Greek Ethics - CR, 46, 3 - 1932 - 105-114the gatheringNo ratings yet
- Jones Later Roman Empire02Document276 pagesJones Later Roman Empire02Anonymous QHOyMJSrNo ratings yet
- Archaeological Institute of AmericaDocument30 pagesArchaeological Institute of AmericaPetrokMaloyNo ratings yet
- Leo Wiener 1920 - History of Arabico-Gothic Culture (Vol. 3 OCR)Document363 pagesLeo Wiener 1920 - History of Arabico-Gothic Culture (Vol. 3 OCR)Anders FernstedtNo ratings yet
- A Cultural History of Work in AntiquityDocument233 pagesA Cultural History of Work in AntiquitycamygutNo ratings yet
- Sherk - Chronology Governors GalatiaDocument11 pagesSherk - Chronology Governors GalatiaRadu UrloiuNo ratings yet
- Pontus and The Outside WorldDocument2 pagesPontus and The Outside Worldon77eir2No ratings yet
- Beaumonts in HistoryDocument333 pagesBeaumonts in HistoryGlen Cooper100% (1)
- Reincarnare OrfismDocument14 pagesReincarnare OrfismButnaru Ana100% (1)
- Constitutia Ateniana Dupa SullaDocument250 pagesConstitutia Ateniana Dupa SullaSteftyra100% (1)
- Fairweather-Seneca The Elder PDFDocument431 pagesFairweather-Seneca The Elder PDFlargodomingo100% (1)
- Bernard - The Greek Kingdoms of Central AsiaDocument31 pagesBernard - The Greek Kingdoms of Central AsiaJose Antonio Monje100% (1)
- Re-Evaluation of Contacts Between Cyprus and CreteDocument22 pagesRe-Evaluation of Contacts Between Cyprus and CreteMirandaFerreiraNo ratings yet
- Rustoiu 2011 Eastern CeltsDocument39 pagesRustoiu 2011 Eastern Celtsbucellarii100% (1)
- Aretaeus of Cappadocia and The First Description oDocument6 pagesAretaeus of Cappadocia and The First Description opepepartaolaNo ratings yet
- Some Manuscript Traditions of The Greek ClassicsDocument44 pagesSome Manuscript Traditions of The Greek ClassicsrmvicentinNo ratings yet
- Freedom and Unfreedom in Early Medieval France PDFDocument35 pagesFreedom and Unfreedom in Early Medieval France PDFJordi Teixidor Abelenda100% (1)
- Adiego (Hellenistic Karia)Document68 pagesAdiego (Hellenistic Karia)Ignasi-Xavier Adiego LajaraNo ratings yet
- Early Ummayad SyriaDocument370 pagesEarly Ummayad Syriafarasat latifNo ratings yet
- 2011.robinson Democracy Beyond Athens Popular Government in The Greek Classical AgeDocument285 pages2011.robinson Democracy Beyond Athens Popular Government in The Greek Classical AgeCamilo Andrés Salas SandovalNo ratings yet
- Burckhardt 1990 The Political Elite of The Roman Republic-Comments On Recent Discussion of The Concepts "Nobilitas" and "Homo Novus"Document24 pagesBurckhardt 1990 The Political Elite of The Roman Republic-Comments On Recent Discussion of The Concepts "Nobilitas" and "Homo Novus"AnneThraxNo ratings yet
- Ancient Legends of Roman History (Barnes & Noble Digital Library)From EverandAncient Legends of Roman History (Barnes & Noble Digital Library)No ratings yet
- Collapse or Survival: Micro-dynamics of crisis and endurance in the ancient central MediterraneanFrom EverandCollapse or Survival: Micro-dynamics of crisis and endurance in the ancient central MediterraneanElisa PeregoNo ratings yet
- Dwayne Meisner - Livy and The BacchanaliaDocument41 pagesDwayne Meisner - Livy and The BacchanaliaedinjuveNo ratings yet
- 21 EsplugaDocument18 pages21 EsplugaedinjuveNo ratings yet
- The Emancipation of WomenDocument15 pagesThe Emancipation of WomenedinjuveNo ratings yet
- Alojz Benac - Prediliri, Prailiri, Protoiliri - Neki Novi AspektiDocument16 pagesAlojz Benac - Prediliri, Prailiri, Protoiliri - Neki Novi AspektiVeriga100% (4)
- De Gubernatione DeiDocument201 pagesDe Gubernatione Deiedinjuve100% (1)
- Y. Hirschfeld, The Crisis of The Sixth Century. Climatic Change, Natural Disasters and The PlagueDocument8 pagesY. Hirschfeld, The Crisis of The Sixth Century. Climatic Change, Natural Disasters and The PlagueedinjuveNo ratings yet
- Behind The Times, The Life of Julian The ApostateDocument14 pagesBehind The Times, The Life of Julian The ApostateedinjuveNo ratings yet
- Trouble in The Kingdom, Church and State in The Fourth CenturyDocument17 pagesTrouble in The Kingdom, Church and State in The Fourth CenturyedinjuveNo ratings yet
- Roman Population SizeDocument37 pagesRoman Population SizeedinjuveNo ratings yet
- Birth Prevention Before The Era of Modern ContraceptionDocument4 pagesBirth Prevention Before The Era of Modern ContraceptionedinjuveNo ratings yet
- The Social Status of Physicians in Greece and RomeDocument25 pagesThe Social Status of Physicians in Greece and RomeedinjuveNo ratings yet
- Dwayne Meisner - Livy and The BacchanaliaDocument41 pagesDwayne Meisner - Livy and The BacchanaliaedinjuveNo ratings yet
- Eutropije-Breviarium Historiae RomanaeDocument95 pagesEutropije-Breviarium Historiae RomanaeedinjuveNo ratings yet
- Drug Study On CephalexinDocument3 pagesDrug Study On CephalexinPrincess C. SultanNo ratings yet
- BodyBallancer Lipo Brochure PDFDocument2 pagesBodyBallancer Lipo Brochure PDFRoss Gale100% (1)
- Booklet Development of Gir Eng LowDocument36 pagesBooklet Development of Gir Eng Lowविकास पाण्डेय100% (4)
- Answers & Solutions: NEET (UG) - 2019Document35 pagesAnswers & Solutions: NEET (UG) - 2019Gowri ShankarNo ratings yet
- 07 Pediatrics in Review July20Document65 pages07 Pediatrics in Review July20AlmaNo ratings yet
- Thesis Statement For Breast Cancer Paper PDFDocument6 pagesThesis Statement For Breast Cancer Paper PDFgcq5c1pv100% (1)
- Tesis Extraction, Identification and Antioxidant Activity of The Phenolic Secondary Metabolites Isolated From The Leaves, Stems and Fruits of Two Shrubs of The Ericaceae FamilyDocument259 pagesTesis Extraction, Identification and Antioxidant Activity of The Phenolic Secondary Metabolites Isolated From The Leaves, Stems and Fruits of Two Shrubs of The Ericaceae FamilylilisacasNo ratings yet
- Industry ProfileDocument18 pagesIndustry ProfileSreejitha ShaijuNo ratings yet
- Senator Rand Paul Letter To CDC On Weber ShandwickDocument3 pagesSenator Rand Paul Letter To CDC On Weber ShandwickZerohedge100% (1)
- Enteral and Parenteral Feeding: Mylin G. Abalus NUTN 204 LecturerDocument24 pagesEnteral and Parenteral Feeding: Mylin G. Abalus NUTN 204 Lecturerminhmap90_635122804No ratings yet
- (Req-172) Ficha Tecnica Pavs 2022 PDFDocument10 pages(Req-172) Ficha Tecnica Pavs 2022 PDFJOSUE YALENo ratings yet
- SG Clean Checklist-Cruise TerminalDocument8 pagesSG Clean Checklist-Cruise TerminallukmannyeoNo ratings yet
- NCM 106 Module 5FDocument22 pagesNCM 106 Module 5FMega SoundNo ratings yet
- Diterpenes From Gorgonian CoralsDocument30 pagesDiterpenes From Gorgonian CoralsWilberto De LimaNo ratings yet
- Kajal: Brief Overview / Career Objective / SummaryDocument3 pagesKajal: Brief Overview / Career Objective / SummaryDrSidharth MehanNo ratings yet
- Effect of Licorice Glycyhrriza Glabra Linn. A Skin Whitening Agent On BLDocument10 pagesEffect of Licorice Glycyhrriza Glabra Linn. A Skin Whitening Agent On BLArif SeptiantoNo ratings yet
- Exploratory LaparotomyDocument11 pagesExploratory LaparotomyKris TejereroNo ratings yet
- Toronto Public Health - Immunization of ChildrenDocument8 pagesToronto Public Health - Immunization of ChildrenCityNewsTorontoNo ratings yet
- Klayman ICC ComplaintDocument27 pagesKlayman ICC ComplaintLaw&Crime100% (2)
- Ilm Al UmraniyatDocument107 pagesIlm Al UmraniyatIslamiaNo ratings yet
- Febrele HemoragiceDocument21 pagesFebrele HemoragiceRotaru MihaiNo ratings yet
- ALS Severity Score of HillelDocument3 pagesALS Severity Score of HillelSlvtierra AzuNo ratings yet
- Soal Latihan Bahasa InggrisDocument12 pagesSoal Latihan Bahasa InggrisMuhamad Rizky Abrizal Lubis - X IPA 1 [27]No ratings yet
- MCN TransesDocument114 pagesMCN TransesADOLF FRUELAN HIDALGONo ratings yet
- Acute Inflammation - ChemotaxisDocument3 pagesAcute Inflammation - ChemotaxisNauzaina IjazNo ratings yet
- Efecto de La Mesoterapia Con Nano ChipDocument7 pagesEfecto de La Mesoterapia Con Nano ChipEdimarKatherineQuinteroGarcíaNo ratings yet
- Failure of Amalgam Restoration PDFDocument2 pagesFailure of Amalgam Restoration PDFJaime0% (1)