You might also like
- Antibiotics: Mos.: 25-50 Mg/kg/day in 3 Divided Doses. Children 3 Mos and Younger: 30Document9 pagesAntibiotics: Mos.: 25-50 Mg/kg/day in 3 Divided Doses. Children 3 Mos and Younger: 30Kath TagamolilaNo ratings yet
- Drug Monograph: Generic Name: Trade Name: Drug Class: IndicationsDocument8 pagesDrug Monograph: Generic Name: Trade Name: Drug Class: IndicationsRawan AlmutairiNo ratings yet
- Drug Study On CeftriaxoneDocument7 pagesDrug Study On CeftriaxoneleoNo ratings yet
- Taxim-O Dry Syrup: Cefixime Oral Suspension IPDocument7 pagesTaxim-O Dry Syrup: Cefixime Oral Suspension IPJudy AncyNo ratings yet
- Cephalexin Use While BreastfeedingDocument8 pagesCephalexin Use While BreastfeedingTilahun MikiasNo ratings yet
- Drug Study AGEDocument9 pagesDrug Study AGECherry Jani OlmedoNo ratings yet
- Antimicrobial Drugs FormularyDocument95 pagesAntimicrobial Drugs FormularymahamoudNo ratings yet
- Drug StudyDocument7 pagesDrug StudyJuliana LegarteNo ratings yet
- Rle Neonate DrugsDocument13 pagesRle Neonate DrugsLhara Vhaneza CuetoNo ratings yet
- Formulations of Representative Drugs From Antibiotics, Antipyretics, Steroids, Injectables and VitaminsDocument4 pagesFormulations of Representative Drugs From Antibiotics, Antipyretics, Steroids, Injectables and VitaminsChandraprakash JangidNo ratings yet
- Cefazolin AncefDocument4 pagesCefazolin AncefAmanda La SalaNo ratings yet
- Alclor: Water Used For Reconstitution Should Be Boiled and CooledDocument1 pageAlclor: Water Used For Reconstitution Should Be Boiled and CooledRubel sheikhNo ratings yet
- En Web Insert Cefaz NLDocument3 pagesEn Web Insert Cefaz NLAbdul AzizNo ratings yet
- Annex I Summary of Product CharacteristicsDocument81 pagesAnnex I Summary of Product CharacteristicsDesNo ratings yet
- Acyclovir Drug StudyDocument3 pagesAcyclovir Drug StudyJessie Cauilan Cain100% (1)
- Acyclovir Drug CardDocument3 pagesAcyclovir Drug CardLisaNo ratings yet
- IMCI UpdatesDocument5 pagesIMCI UpdatesJaypee Ravina100% (2)
- Penicillin: Libre, Princess Melanie SDocument19 pagesPenicillin: Libre, Princess Melanie SIrene Grace BalcuevaNo ratings yet
- 2nd Drug StudyDocument39 pages2nd Drug StudyYanna Habib-Mangotara100% (3)
- PBBN 1St Yr Child Health Nursing CBIMNCIDocument29 pagesPBBN 1St Yr Child Health Nursing CBIMNCIcopy smart100% (1)
- Cephalexin: Adjust-A-Dose (For All Indications)Document3 pagesCephalexin: Adjust-A-Dose (For All Indications)HannaNo ratings yet
- Ac IphinDocument5 pagesAc IphinAdittya DuttaNo ratings yet
- Nursing Care PlanDocument8 pagesNursing Care PlanVincent QuitorianoNo ratings yet
- Drug InfoDocument11 pagesDrug InfoArjun SinghNo ratings yet
- CiprofloxacinDocument5 pagesCiprofloxacinWen RodsaNo ratings yet
- Typhoid GuidelinesDocument3 pagesTyphoid GuidelinesMuthia Rahma AninditaNo ratings yet
- Abbreviated PI ABBOTIC DraftDocument2 pagesAbbreviated PI ABBOTIC Draftadani 2372No ratings yet
- FluconazoleDocument3 pagesFluconazoleapi-3797941100% (1)
- ZegenDocument9 pagesZegenJefferson ManasanNo ratings yet
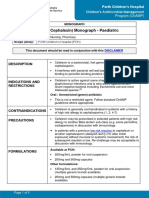
- Cefalexin (Cephalexin) Monograph - Paediatric: DescriptionDocument5 pagesCefalexin (Cephalexin) Monograph - Paediatric: Descriptioneinas omerNo ratings yet
- Urinary Tract InfectionsDocument15 pagesUrinary Tract InfectionsAnonymous elSqPhzKNo ratings yet
- Cephalexin (Drug Study)Document2 pagesCephalexin (Drug Study)Franz.thenurse688894% (17)
- Cefuroxime AxetilDocument4 pagesCefuroxime AxetilSebastian CruzNo ratings yet
- Drug Study OrthoDocument17 pagesDrug Study OrthoMc Crister SilangNo ratings yet
- Amoxicillin (Amoxycillin) : PresentationDocument4 pagesAmoxicillin (Amoxycillin) : PresentationRavikiran SuryanarayanamurthyNo ratings yet
- EPIGENTDocument3 pagesEPIGENTmahgad100% (1)
- Infectious Gastroenteritis BaDocument1 pageInfectious Gastroenteritis BafionaNo ratings yet
- Mycophenolate Mofetil (CellCept)Document16 pagesMycophenolate Mofetil (CellCept)ddandan_2No ratings yet
- HyperbilirubinemiaDocument10 pagesHyperbilirubinemiachiboogs456100% (1)
- Drug StudyDocument10 pagesDrug StudybaniniycsebNo ratings yet
- Imci UpdatesDocument37 pagesImci UpdateskristiandiorcapiliNo ratings yet
- Ciprofloxacin: A Drug Study OnDocument5 pagesCiprofloxacin: A Drug Study Onkarl montanoNo ratings yet
- Case Study 2Document6 pagesCase Study 2Princess Pearl MadambaNo ratings yet
- Meds SummaryDocument22 pagesMeds SummaryChamCham AquinoNo ratings yet
- Assignment On Drugs Used For NewbornDocument11 pagesAssignment On Drugs Used For Newbornvarshasharma05100% (1)
- Antifungal AgentsDocument42 pagesAntifungal AgentsOluwatobi AyomideNo ratings yet
- Pharmacology Obat Lepra Dan TBC Kutis: Dharma Permana, PHD, AptDocument33 pagesPharmacology Obat Lepra Dan TBC Kutis: Dharma Permana, PHD, AptanggiNo ratings yet
- CPG On Acute Infectious Diarrhea 2021Document42 pagesCPG On Acute Infectious Diarrhea 2021babbettemdNo ratings yet
- Imipenem, Cilastatin, and Relebactam - Drug Information - UpToDateDocument10 pagesImipenem, Cilastatin, and Relebactam - Drug Information - UpToDateMarius PapuricaNo ratings yet
- CeftriaxoneDocument60 pagesCeftriaxoneKazamatsu RyoNo ratings yet
- 1.3.1.1 Ireland Tavanic 500mg SMPC PDFDocument19 pages1.3.1.1 Ireland Tavanic 500mg SMPC PDFНатали КапанадзеNo ratings yet
- Drugs, Amlodipine, Cefuroxime, Drug StudyDocument8 pagesDrugs, Amlodipine, Cefuroxime, Drug StudyKevin Sam AguirreNo ratings yet
- Health Education PlanDocument5 pagesHealth Education PlancherylNo ratings yet
- Avlosef PDFDocument4 pagesAvlosef PDFAdnan Al MahmudNo ratings yet
- Health ArticlesDocument5 pagesHealth Articlesprashant_shivdas_1No ratings yet
- Amoxicillin 125 MG 250 MG 5 ML Oral SuspensionDocument16 pagesAmoxicillin 125 MG 250 MG 5 ML Oral SuspensionAshrafNo ratings yet
- Urinary Tract Infection PDFDocument9 pagesUrinary Tract Infection PDFTigerEyzNo ratings yet
- NCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!From EverandNCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!Rating: 5 out of 5 stars5/5 (4)
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- RF23BB8600 V9Document2 pagesRF23BB8600 V9JOSUE YALENo ratings yet
- Molecules 27 07102 v2Document17 pagesMolecules 27 07102 v2JOSUE YALENo ratings yet
- Cinnamon CO2 Extract All DocumentsDocument33 pagesCinnamon CO2 Extract All DocumentsJOSUE YALENo ratings yet
- WillitFit RF23BB8600 V2Document1 pageWillitFit RF23BB8600 V2JOSUE YALENo ratings yet
- Grp.3 Bio Case Study of DwarfismDocument9 pagesGrp.3 Bio Case Study of DwarfismJhovelNo ratings yet
- Key Lab Tests For A Wellness Tune - DR Wes YoungbergDocument4 pagesKey Lab Tests For A Wellness Tune - DR Wes YoungbergblancorNo ratings yet
- Adult Reference Dose/volume Limits: Structure Volume (CC) Total Dose (Gy) Max Dose (Gy) Endpoint Notes ReferenceDocument6 pagesAdult Reference Dose/volume Limits: Structure Volume (CC) Total Dose (Gy) Max Dose (Gy) Endpoint Notes ReferenceEdis Đedović100% (1)
- Research For MR DejeneDocument20 pagesResearch For MR Dejenetakele loveNo ratings yet
- NYSDOH Commissioner Howard Zucker Letter of DeterminationDocument3 pagesNYSDOH Commissioner Howard Zucker Letter of DeterminationNews10NBCNo ratings yet
- SOAP Note - ContraceptionDocument5 pagesSOAP Note - ContraceptionG. Crusor-PriceNo ratings yet
- The Case of Mr. Mohammad With Pneumonia Pleural EffusionDocument6 pagesThe Case of Mr. Mohammad With Pneumonia Pleural EffusionjanaNo ratings yet
- Chemical Toxicity Summit Day 2Document4 pagesChemical Toxicity Summit Day 2Paul Ioan PopescuNo ratings yet
- Cholel FinalDocument39 pagesCholel FinalRizza DaleNo ratings yet
- Apa - Tehnologii MedicaleDocument125 pagesApa - Tehnologii MedicaleNick OviciNo ratings yet
- Helping Pre-Teens and Teenagers Build Personal Hygiene HabitsDocument2 pagesHelping Pre-Teens and Teenagers Build Personal Hygiene HabitsMark Anthony Evangelista CabrietoNo ratings yet
- Tuberculous MeningitisDocument34 pagesTuberculous MeningitisLuvi PujiNo ratings yet
- Terapi 2Document7 pagesTerapi 2emma sitahNo ratings yet
- The Ef Cacy of Systematic Active Conservative Treatment For Patients With Severe SciaticaDocument12 pagesThe Ef Cacy of Systematic Active Conservative Treatment For Patients With Severe SciaticaTomáš KrajíčekNo ratings yet
- Exploratory Laparotomy Part 1Document3 pagesExploratory Laparotomy Part 1vishwanathNo ratings yet
- NOTES RLE - Care of Mother, Child at Risk or With Problems (Acute and Chronic)Document2 pagesNOTES RLE - Care of Mother, Child at Risk or With Problems (Acute and Chronic)SteffiNo ratings yet
- Module 7 - Health-and-Promotion-and-EducationDocument7 pagesModule 7 - Health-and-Promotion-and-EducationPascua, Aliah M.No ratings yet
- Swathi PDFDocument2 pagesSwathi PDFPalaniappan GurusamyNo ratings yet
- Infection Control in ORDocument10 pagesInfection Control in ORaaminah tariqNo ratings yet
- Vaccination CentersDocument4 pagesVaccination CentersdmonlinelkNo ratings yet
- Lesson 10 Reaching The Age of AdolescenceDocument47 pagesLesson 10 Reaching The Age of AdolescenceAvi :DNo ratings yet
- Test Bank ECGs Made Easy 5th Edition Barbara J AehlertDocument10 pagesTest Bank ECGs Made Easy 5th Edition Barbara J AehlertErnest67% (3)
- Trauma in The Aging PopulationDocument21 pagesTrauma in The Aging PopulationBruce Fredy Chino ChambillaNo ratings yet
- IV HistoryDocument2 pagesIV HistoryHilas Rosalliv KcinmorNo ratings yet
- Purpura Fulminans: Mechanism and Management of Dysregulated HemostasisDocument21 pagesPurpura Fulminans: Mechanism and Management of Dysregulated HemostasisntnquynhproNo ratings yet
- Nursing Report Of: The BurningDocument11 pagesNursing Report Of: The BurningAbbas AwfiNo ratings yet
- P7b11toc Gastroenterology and NutritionDocument19 pagesP7b11toc Gastroenterology and NutritionWidya Lestari CapawatyNo ratings yet
- Hearing-Impairment Case StudyDocument10 pagesHearing-Impairment Case StudyIrish Eunice Felix100% (1)
- Değişim Sınavı 2020Document29 pagesDeğişim Sınavı 2020Mustafa CinNo ratings yet
- En - Public Health Engineering in Precarious Situations 2010Document411 pagesEn - Public Health Engineering in Precarious Situations 2010Matteo LorenzoniNo ratings yet