You might also like
- Health Related Quality of Life, Depression and Anxiety Among People With Type 2 Diabetes Mellitus in BangladeshDocument26 pagesHealth Related Quality of Life, Depression and Anxiety Among People With Type 2 Diabetes Mellitus in BangladeshGhanva KhanNo ratings yet
- A Study On Depression Among Patient With Type 2 Diabetes Mellitus in North-Eastcoast MalaysiaDocument12 pagesA Study On Depression Among Patient With Type 2 Diabetes Mellitus in North-Eastcoast Malaysiayeremias setyawanNo ratings yet
- Comorbidity of Fetal Alcohol Spectrum Disorder A SystematicDocument10 pagesComorbidity of Fetal Alcohol Spectrum Disorder A SystematicAriNo ratings yet
- Erectile Dysfunction and Comorbid Diseases, Androgen Deficiency, and Diminished Libido in MenDocument7 pagesErectile Dysfunction and Comorbid Diseases, Androgen Deficiency, and Diminished Libido in MenAfif Al FatihNo ratings yet
- A Study of Depression in Diabetes Mellitus: Analysis From Rural Hospital, India 1Document6 pagesA Study of Depression in Diabetes Mellitus: Analysis From Rural Hospital, India 1International Medical PublisherNo ratings yet
- Schizophrenia Research: ArticleinfoDocument5 pagesSchizophrenia Research: ArticleinfojhuNo ratings yet
- Ajol File Journals - 75 - Articles - 155877 - Submission - Proof - 155877 889 406908 1 10 20170511Document6 pagesAjol File Journals - 75 - Articles - 155877 - Submission - Proof - 155877 889 406908 1 10 20170511Reni Tri AstutiNo ratings yet
- Research Letter: Risk of Depression Among Patients With Acne in The U.K.: A Population-Based Cohort StudyDocument2 pagesResearch Letter: Risk of Depression Among Patients With Acne in The U.K.: A Population-Based Cohort StudyadhastriNo ratings yet
- Sexual Dysfunction Among Women With Diabetes in A Primary Health Care at Semarang, Central Java Province, IndonesiaDocument8 pagesSexual Dysfunction Among Women With Diabetes in A Primary Health Care at Semarang, Central Java Province, IndonesiaTantonio Tri PutraNo ratings yet
- Erectile FactorDocument6 pagesErectile FactorRidha MardiyaniNo ratings yet
- Karakteristik Penderita Diabetes Mellitus Dengan Komplikasi Yang Di Rawat Inap Di RSUD Deli Serdang Tahun 2012 Fitriana Butarbutar, Hiswani, JemadiDocument10 pagesKarakteristik Penderita Diabetes Mellitus Dengan Komplikasi Yang Di Rawat Inap Di RSUD Deli Serdang Tahun 2012 Fitriana Butarbutar, Hiswani, JemadiEstiPramestiningtyasNo ratings yet
- Gender Differences in Major Depressive Disorder: Findings From The Singapore Mental Health StudyDocument7 pagesGender Differences in Major Depressive Disorder: Findings From The Singapore Mental Health StudyFelisia OngNo ratings yet
- 4851-Article Text-14655-2-10-20170116 PDFDocument14 pages4851-Article Text-14655-2-10-20170116 PDFKIMNo ratings yet
- Kaur PDFDocument13 pagesKaur PDFAtikaWidyaSyariNo ratings yet
- International Journal of Health Sciences and Research: Stress and Diabetes MellitusDocument8 pagesInternational Journal of Health Sciences and Research: Stress and Diabetes Mellitusamalia dikaNo ratings yet
- International Journal of Health Sciences and Research: Stress and Diabetes MellitusDocument8 pagesInternational Journal of Health Sciences and Research: Stress and Diabetes MellitusmariahelenaneiNo ratings yet
- Geriatrics: Memory and Learning Complaints in Relation To Depression Among Elderly People With MultimorbidityDocument9 pagesGeriatrics: Memory and Learning Complaints in Relation To Depression Among Elderly People With MultimorbidityPutri AyuningtyasNo ratings yet
- Prevalence of Depression Among Diabetic Patient Attendingprimary Health Care Centers in Almadinah AlmunawaraDocument14 pagesPrevalence of Depression Among Diabetic Patient Attendingprimary Health Care Centers in Almadinah AlmunawaraIJAR JOURNALNo ratings yet
- Biology - Down Syndrome Literature ReviewDocument8 pagesBiology - Down Syndrome Literature ReviewAllyssa RuiNo ratings yet
- The Costs of Depression - Kessler2012Document14 pagesThe Costs of Depression - Kessler2012chen eliseNo ratings yet
- Migraine: Epidemiology, Burden, and ComorbidityDocument19 pagesMigraine: Epidemiology, Burden, and ComorbidityDhruvin KapadiaNo ratings yet
- Association Between Generalized Anxiety Disorder and Premenstrual Dysphoric Disorder in A Diagnostic Interviewing StudyDocument11 pagesAssociation Between Generalized Anxiety Disorder and Premenstrual Dysphoric Disorder in A Diagnostic Interviewing StudyRebecaNo ratings yet
- Comorbid Mental Disorders in Children and Adolescents With Attention-Deficit:hyperactivity Disorder in A Large Nationwide StudyDocument12 pagesComorbid Mental Disorders in Children and Adolescents With Attention-Deficit:hyperactivity Disorder in A Large Nationwide StudyMarina HeinenNo ratings yet
- v15n3 Original Article 4Document8 pagesv15n3 Original Article 4Shazwani KKTSNo ratings yet
- 17 PDFDocument6 pages17 PDFGinsha Audia KusumoNo ratings yet
- Prevalence of Depression Symptoms in Diabetes Mellitus: Salih EkerDocument4 pagesPrevalence of Depression Symptoms in Diabetes Mellitus: Salih EkerNathayaNeilaVarneliaNo ratings yet
- Prevalence and Its Associated Determinants of Diabetic Peripheral Neuropathy (DPN) in Individuals Having Type-2 Diabetes Mellitus in Rural South India _[PAUTHORS], Indian Journal of Community Medicine (IJCM)Document3 pagesPrevalence and Its Associated Determinants of Diabetic Peripheral Neuropathy (DPN) in Individuals Having Type-2 Diabetes Mellitus in Rural South India _[PAUTHORS], Indian Journal of Community Medicine (IJCM)Michael SelvarajNo ratings yet
- Cognitive Impairment and Its Associated Risk Factors in The Elderly With Type 2 Diabetes MellitusDocument7 pagesCognitive Impairment and Its Associated Risk Factors in The Elderly With Type 2 Diabetes MellitusFera EyFeraNo ratings yet
- SAJPsy 25 1382 PDFDocument7 pagesSAJPsy 25 1382 PDFNix SantosNo ratings yet
- Rheumatic Heart Disease Anno 2020. Impacts of Gender and Migration On Epidemiology and Management (2020)Document9 pagesRheumatic Heart Disease Anno 2020. Impacts of Gender and Migration On Epidemiology and Management (2020)7 MNTNo ratings yet
- Comparative Analysis of Self-Injury in People With Psychopathology or Neurodevelopmental DisordersDocument13 pagesComparative Analysis of Self-Injury in People With Psychopathology or Neurodevelopmental Disordersme13No ratings yet
- Epidemiology of Eating Disorders: Incidence, Prevalence and Mortality RatesDocument9 pagesEpidemiology of Eating Disorders: Incidence, Prevalence and Mortality RatesVictória NamurNo ratings yet
- Jurnal DiabetesDocument50 pagesJurnal DiabetesYusmiyati YusmiyatiNo ratings yet
- Prevalence and Determinants of Depression Among Communitydwelling Older Adults With Chronic DiseasesDocument7 pagesPrevalence and Determinants of Depression Among Communitydwelling Older Adults With Chronic DiseasesIJPHSNo ratings yet
- 7418 26240 1 PBDocument7 pages7418 26240 1 PBPattra KeeratibharatNo ratings yet
- BMJ Risk Fall On Neuro DiseaseDocument17 pagesBMJ Risk Fall On Neuro DiseaseAmaliFaizNo ratings yet
- Lancet ADHD Submission March 2017 - No HighlightsDocument35 pagesLancet ADHD Submission March 2017 - No HighlightsDanna OleaNo ratings yet
- Brasil, Campeão Mundial de DepressãoDocument16 pagesBrasil, Campeão Mundial de DepressãoValéria AlmeidaNo ratings yet
- Diabetic Retinopathy 2013 ArticleDocument3 pagesDiabetic Retinopathy 2013 ArticleRe-zha 'Putra'No ratings yet
- 33 Jan2013 006 240425 090126Document3 pages33 Jan2013 006 240425 090126drsjkianiNo ratings yet
- Sex Differences in Predicting ADHD Clinical Diagnosis and Pharmacological TreatmentDocument9 pagesSex Differences in Predicting ADHD Clinical Diagnosis and Pharmacological TreatmentLiesth YaninaNo ratings yet
- Jurnal PsikoDocument8 pagesJurnal PsikoruryNo ratings yet
- 1 s2.0 S1751991818300032 MainDocument7 pages1 s2.0 S1751991818300032 MainArthur EntwhistleNo ratings yet
- Prevalence 2013 AlemaniDocument9 pagesPrevalence 2013 AlemanitxankleroNo ratings yet
- Research Article Females With Type 2 Diabetes Mellitus Are Prone To Diabetic Retinopathy: A Twelve-Province Cross-Sectional Study in ChinaDocument9 pagesResearch Article Females With Type 2 Diabetes Mellitus Are Prone To Diabetic Retinopathy: A Twelve-Province Cross-Sectional Study in ChinaM FATHUL BARINo ratings yet
- Comorbidity of Borderline 2018Document11 pagesComorbidity of Borderline 2018Dhino Armand Quispe SánchezNo ratings yet
- Mccoy Document 2019Document59 pagesMccoy Document 2019Masih LoghmaniNo ratings yet
- Introduction-WPS OfficeDocument21 pagesIntroduction-WPS Officemadanfalah11No ratings yet
- Rajiv Gandhi University of Health Sciences, Bangalore, Karnataka Proforma For Registration of Subject For DissertationDocument16 pagesRajiv Gandhi University of Health Sciences, Bangalore, Karnataka Proforma For Registration of Subject For DissertationAngel SethNo ratings yet
- 1 s2.0 S016557282100196X MainDocument5 pages1 s2.0 S016557282100196X MainXimena VNo ratings yet
- 23 Rajeshkanna EtalDocument8 pages23 Rajeshkanna EtaleditorijmrhsNo ratings yet
- Journal 2Document8 pagesJournal 2pososuperNo ratings yet
- Evaluation of Covid-19 Pandemic - Related Depression in Geriatric Patients at PRH, Loni: A Cross Sectional StudyDocument8 pagesEvaluation of Covid-19 Pandemic - Related Depression in Geriatric Patients at PRH, Loni: A Cross Sectional StudyIJAR JOURNALNo ratings yet
- Depresion JurnalDocument10 pagesDepresion JurnalPaskalia ChristinNo ratings yet
- Parkinson en Hombres y MujeresDocument15 pagesParkinson en Hombres y MujeresAbigail RamosNo ratings yet
- Dry EyeDocument11 pagesDry EyeFriedi Kristian Carlos100% (1)
- Role and Position of International Environmental Institutions in Environmental ManagementDocument13 pagesRole and Position of International Environmental Institutions in Environmental ManagementIJAR JOURNALNo ratings yet
- Prevalence of Depression Among Primary Health Care Attendees Using PHQ 9 in Al Madinah, Saudi ArabiaDocument13 pagesPrevalence of Depression Among Primary Health Care Attendees Using PHQ 9 in Al Madinah, Saudi ArabiaIJAR JOURNALNo ratings yet
- 82264-Article Text-197411-1-10-20121015 PDFDocument6 pages82264-Article Text-197411-1-10-20121015 PDFJamesNo ratings yet
- Experiences of Adolescents Living with Type 1 Diabetes Mellitus whilst Negotiating with the Society: Submitted as part of the MSc degree in diabetes University of Surrey, Roehampton, 2003From EverandExperiences of Adolescents Living with Type 1 Diabetes Mellitus whilst Negotiating with the Society: Submitted as part of the MSc degree in diabetes University of Surrey, Roehampton, 2003No ratings yet
- Module 2 OB Ward CLMMRHDocument5 pagesModule 2 OB Ward CLMMRHKristil ChavezNo ratings yet
- Guideline of Record-KeepingDocument9 pagesGuideline of Record-KeepingGen LCNo ratings yet
- Breast Cancer Medical Surgical NursingDocument5 pagesBreast Cancer Medical Surgical NursingKath RubioNo ratings yet
- Bovine Mastitis PDFDocument34 pagesBovine Mastitis PDFMamtaNo ratings yet
- EpinephrineDocument16 pagesEpinephrineBrad Pitt-HongNo ratings yet
- OEC Chapter 1-5Document20 pagesOEC Chapter 1-5Phil McLeanNo ratings yet
- Attention-Deficit/Hyperactivity Disorder in The Depressed AdultDocument10 pagesAttention-Deficit/Hyperactivity Disorder in The Depressed AdultasclepiuspdfsNo ratings yet
- 2-5 Slideshow MOOC MID How To Write A Deterministic Model BasedDocument7 pages2-5 Slideshow MOOC MID How To Write A Deterministic Model Basedkonemina85No ratings yet
- 1.facies R Flores B N PDFDocument16 pages1.facies R Flores B N PDFDenys PQNo ratings yet
- 2008Document1,696 pages2008Ann Arbor Government DocumentsNo ratings yet
- Pes Planus by MIDocument36 pagesPes Planus by MIUbaid AzherNo ratings yet
- Cambridge IGCSE: Biology 0610/32Document20 pagesCambridge IGCSE: Biology 0610/32K KNo ratings yet
- Written Report For SyphilisDocument7 pagesWritten Report For SyphilisDavid ValbuenaNo ratings yet
- Management of Congenital Aural AtresiaDocument22 pagesManagement of Congenital Aural AtresiamelaniNo ratings yet
- Calcifications of The Urinary TractDocument44 pagesCalcifications of The Urinary Tractadhik_deepakNo ratings yet
- ISHRS 21st Abstract Book 2013 SanFran DR Alan Bauman FinalDocument542 pagesISHRS 21st Abstract Book 2013 SanFran DR Alan Bauman FinalAlan J Bauman MDNo ratings yet
- Prevention of Foot Ulcer 2020Document22 pagesPrevention of Foot Ulcer 2020Devi SiswaniNo ratings yet
- What Is Asthenopia?: EyestrainDocument6 pagesWhat Is Asthenopia?: EyestrainAnkita GoswamiNo ratings yet
- Pursed Lip BreathingDocument4 pagesPursed Lip BreathingDinesh KumarNo ratings yet
- Notes FileDocument78 pagesNotes FileSEIYADU IBRAHIM K100% (1)
- The Evaluation and Management of An Incessantly Crying InfantDocument3 pagesThe Evaluation and Management of An Incessantly Crying InfantZīshān FārūqNo ratings yet
- Histopathology PrelimsDocument2 pagesHistopathology PrelimscassseeeyyyNo ratings yet
- Demodectic Mange and Inexpensive TreatmentDocument3 pagesDemodectic Mange and Inexpensive Treatmentcigar77No ratings yet
- pdf2 PDFDocument125 pagespdf2 PDFsushma shresthaNo ratings yet
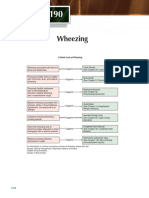
- Wheezing: A Quick Look at WheezingDocument1 pageWheezing: A Quick Look at WheezingpelinNo ratings yet
- Lecture N4 Breast-Feeding. Value and Advantages of Breast-Feeding. Methods of Calculation of Daily Volume of Feeding. Weaning at Breast FeedingDocument7 pagesLecture N4 Breast-Feeding. Value and Advantages of Breast-Feeding. Methods of Calculation of Daily Volume of Feeding. Weaning at Breast FeedingAVINASH PvkNo ratings yet
- AppendicitisDocument3 pagesAppendicitisPrince Jhessie L. AbellaNo ratings yet
- MCQ On Bleeding in Early Pregnancy: DR Manal Behery Zagazig University 2013Document36 pagesMCQ On Bleeding in Early Pregnancy: DR Manal Behery Zagazig University 2013joseph0% (1)
- TMS Special Edition 17 0821webDocument52 pagesTMS Special Edition 17 0821webalinaNo ratings yet
- BSL 2Document30 pagesBSL 2Shafira Nurianti salimNo ratings yet


























![Prevalence and Its Associated Determinants of Diabetic Peripheral Neuropathy (DPN) in Individuals Having Type-2 Diabetes Mellitus in Rural South India _[PAUTHORS], Indian Journal of Community Medicine (IJCM)](https://imgv2-2-f.scribdassets.com/img/document/527040009/149x198/b045f9b0ff/1632384843?v=1)