You might also like
- Magic Frequencies: Excerpted From The Mixing Engineer's HandbookDocument5 pagesMagic Frequencies: Excerpted From The Mixing Engineer's HandbookmehmetkurtulusNo ratings yet
- Invertebrate ZoologyDocument1,016 pagesInvertebrate ZoologyRACHANA PURKAYASTHA 2140623No ratings yet
- Permaculture - Plants Suitable For Ground Cover (P) - Plants For A FutureDocument2 pagesPermaculture - Plants Suitable For Ground Cover (P) - Plants For A Futurecontadino_impazzitoNo ratings yet
- Toxicological Stability of Drugs: de Jesus, Adia Cavrinni G. Manalo, Alyssa ADocument42 pagesToxicological Stability of Drugs: de Jesus, Adia Cavrinni G. Manalo, Alyssa AAlyssa ManaloNo ratings yet
- Computer-Assisted Craniomaxillofacial Surgery: Sean P. EdwardsDocument18 pagesComputer-Assisted Craniomaxillofacial Surgery: Sean P. Edwardshasan nazzalNo ratings yet
- 01-System Devices Configuration - Rev GDocument36 pages01-System Devices Configuration - Rev GPABITRA PATRANo ratings yet
- Heat Sink Capacity Mesurment in Inservice PipelineDocument13 pagesHeat Sink Capacity Mesurment in Inservice PipelineSomeshNo ratings yet
- 5276Document52 pages5276Sean PorterNo ratings yet
- CardiomyopathyDocument1 pageCardiomyopathyTrisha VergaraNo ratings yet
- Casas-Murillo2021 Article 3D-printedAnatomicalModelsOfThDocument8 pagesCasas-Murillo2021 Article 3D-printedAnatomicalModelsOfThVicente Bruno GuimaraesNo ratings yet
- 3D Reconstruction of Coronary Arteries and Atherosclerotic Plaques Based On Computed Tomography Angiography ImagesDocument9 pages3D Reconstruction of Coronary Arteries and Atherosclerotic Plaques Based On Computed Tomography Angiography ImagesAndres VeLandiaNo ratings yet
- Medical Engineering and PhysicsDocument12 pagesMedical Engineering and PhysicsKain SmithNo ratings yet
- Retrolaparoscopic Adrenalectomy Assisted by Three-Dimensional Reconstructed Digital Model in A Patient With Situs Inversus TotalisDocument5 pagesRetrolaparoscopic Adrenalectomy Assisted by Three-Dimensional Reconstructed Digital Model in A Patient With Situs Inversus Totalisyerich septaNo ratings yet
- Sicotj 3 16Document10 pagesSicotj 3 16OstazNo ratings yet
- Implications of 3-Dimensional Printed Spinal Implants On The Outcomes in Spine SurgeryDocument10 pagesImplications of 3-Dimensional Printed Spinal Implants On The Outcomes in Spine SurgeryOstazNo ratings yet
- Three-Dimensional Computerized Orthognathic Surgical Treatment PlanningDocument10 pagesThree-Dimensional Computerized Orthognathic Surgical Treatment PlanningRajan KarmakarNo ratings yet
- 2018 Article 546Document7 pages2018 Article 546giuseppelombard1984No ratings yet
- 1 s2.0 S2352914820301969 MainDocument11 pages1 s2.0 S2352914820301969 MainSINGSTONNo ratings yet
- Marsupialization of Keratocystic Odontogenic Tumors of The Mandible: Longitudinal Image Analysis of Tumor Size Via 3D Visualized CT ScansDocument14 pagesMarsupialization of Keratocystic Odontogenic Tumors of The Mandible: Longitudinal Image Analysis of Tumor Size Via 3D Visualized CT ScansAndreas SimamoraNo ratings yet
- Lower Leg Reconstruction After Resection of A Squamous Cell CarcinomaDocument7 pagesLower Leg Reconstruction After Resection of A Squamous Cell CarcinomaOli BotaNo ratings yet
- Barber 2018Document4 pagesBarber 2018Boris CanahuireNo ratings yet
- Semi Automated Three Dimensional Condylar Reconstruction.Document5 pagesSemi Automated Three Dimensional Condylar Reconstruction.tamisatnamNo ratings yet
- Journal of Orthopaedic Translation: Lin Xu, Hao Qin, Jia Tan, Zhilin Cheng, Xiang Luo, Haitao Tan, Wenhua HuangDocument7 pagesJournal of Orthopaedic Translation: Lin Xu, Hao Qin, Jia Tan, Zhilin Cheng, Xiang Luo, Haitao Tan, Wenhua HuangLeiNo ratings yet
- Thoracoabdominal Aortic Aneurysms Open RepairDocument13 pagesThoracoabdominal Aortic Aneurysms Open RepairJonathan Frimpong AnsahNo ratings yet
- Development of A Patient-Specific 3D-Printed Liver Model For Preoperative PlanningDocument6 pagesDevelopment of A Patient-Specific 3D-Printed Liver Model For Preoperative PlanningDaniel PredaNo ratings yet
- Virtual Surgical Planning in Craniofacial Surgery: Harvey Chim, MBBS Nicholas Wetjen, MD Samir Mardini, MDDocument8 pagesVirtual Surgical Planning in Craniofacial Surgery: Harvey Chim, MBBS Nicholas Wetjen, MD Samir Mardini, MDR KNo ratings yet
- Automatic Tool Segmentation and Tracking During Robotic Intravascular Catheterization For Cardiac InterventionsDocument23 pagesAutomatic Tool Segmentation and Tracking During Robotic Intravascular Catheterization For Cardiac InterventionsNishant UzirNo ratings yet
- Stereolithographic Surgical Template: A Review: Abst TDocument3 pagesStereolithographic Surgical Template: A Review: Abst Tairtifa1No ratings yet
- Klatt 2013Document4 pagesKlatt 2013Sung Soon ChangNo ratings yet
- Bmri2021 5018791Document15 pagesBmri2021 5018791OstazNo ratings yet
- Three-Dimensional Imaging in Orthodontics: ReviewDocument9 pagesThree-Dimensional Imaging in Orthodontics: Reviewdrzana78No ratings yet
- Numerical Study of The Fluid-Dynamics in Coronary Artery Bypass GraftsDocument5 pagesNumerical Study of The Fluid-Dynamics in Coronary Artery Bypass GraftsRiccardo FerreroNo ratings yet
- An Automatic Virtual Patient Reconstruction From CT Scan For Hepatic Surgical PlanningDocument7 pagesAn Automatic Virtual Patient Reconstruction From CT Scan For Hepatic Surgical Planningles7evaNo ratings yet
- Accuracy of Using Computer-Aided Rapid Prototyping Templates For Mandible Reconstruction With An Iliac Crest GraftDocument9 pagesAccuracy of Using Computer-Aided Rapid Prototyping Templates For Mandible Reconstruction With An Iliac Crest GraftHương LanNo ratings yet
- Comparison of Cone-Beam Imaging With Orthopantomography and Computerized Tomography For Assessment in Presurgical Implant DentistryDocument10 pagesComparison of Cone-Beam Imaging With Orthopantomography and Computerized Tomography For Assessment in Presurgical Implant DentistryMihai DascalescuNo ratings yet
- Virtual PDF Gaya3 AkkaDocument12 pagesVirtual PDF Gaya3 AkkaVahini Benna100% (1)
- Advanced Applications of Cone Beam Computed Tomography in OrthodonticsDocument15 pagesAdvanced Applications of Cone Beam Computed Tomography in Orthodonticsaung NaingmyoNo ratings yet
- 3D Reconstruction of Coronary Arteries From Angiographic Images: A SurveyDocument6 pages3D Reconstruction of Coronary Arteries From Angiographic Images: A SurveyijcsnNo ratings yet
- Ghid Plex Brahial Conturaj PDFDocument7 pagesGhid Plex Brahial Conturaj PDFMiruna MafteiNo ratings yet
- Cohen2019 Atualização Sobre Os Aspectos Atuais Da Imagem Orbital .Tomografia Computadorizada, Ressonância Magnética e UltrassonografiaDocument11 pagesCohen2019 Atualização Sobre Os Aspectos Atuais Da Imagem Orbital .Tomografia Computadorizada, Ressonância Magnética e Ultrassonografiaana clara scopelNo ratings yet
- Diagnosticc in Many WaysDocument5 pagesDiagnosticc in Many WaysTudor DumitrascuNo ratings yet
- Video-Atlas of Open Thoracoabdominal Aortic Aneurysm RepairDocument6 pagesVideo-Atlas of Open Thoracoabdominal Aortic Aneurysm Repairvan le hoangNo ratings yet
- Video-Atlas of Open Thoracoabdominal Aortic Aneurysm RepairDocument6 pagesVideo-Atlas of Open Thoracoabdominal Aortic Aneurysm Repairvan le hoangNo ratings yet
- 3dprinting in Orthopedic OncologyDocument26 pages3dprinting in Orthopedic OncologyAnto Anand GopurathingalNo ratings yet
- Computer TomographyDocument4 pagesComputer TomographysujithasNo ratings yet
- 1 s2.0 S0167814022001529 MainDocument6 pages1 s2.0 S0167814022001529 MainnimaelhajjiNo ratings yet
- Conebeam CT of The Head and Neck, Part 2: Clinical ApplicationsDocument8 pagesConebeam CT of The Head and Neck, Part 2: Clinical ApplicationshaneefmdfNo ratings yet
- 61073Document12 pages61073Mohamed AhmedNo ratings yet
- 135-Full Paper For Regular Journal Issue-800-2-10-20211115Document2 pages135-Full Paper For Regular Journal Issue-800-2-10-20211115chn millamaNo ratings yet
- Automatic Segmentation of Liver Tumor in CT ImagesDocument6 pagesAutomatic Segmentation of Liver Tumor in CT Imagesmanju.dsatmNo ratings yet
- 1 s2.0 S0278239118303045 MainDocument11 pages1 s2.0 S0278239118303045 Mainfabian hernandez medinaNo ratings yet
- Robot-Assisted Microwave Thermoablation of Liver Tumors: A Single-Center ExperienceDocument9 pagesRobot-Assisted Microwave Thermoablation of Liver Tumors: A Single-Center ExperienceMamanya Fadhil HaniNo ratings yet
- Base Segudo Caso ClinicoDocument6 pagesBase Segudo Caso Clinicogatos965669988No ratings yet
- Reducing The Model Variance of A Rectal Cancer Segmentation NetworkDocument9 pagesReducing The Model Variance of A Rectal Cancer Segmentation NetworkDiego Marcelino Santos SilvaNo ratings yet
- Journal Pone 0269931Document13 pagesJournal Pone 0269931Abdelali MoufidiNo ratings yet
- AJNR - Conebeam CT of The Head and Neck, Part 2 - Clinical ApplicationsDocument9 pagesAJNR - Conebeam CT of The Head and Neck, Part 2 - Clinical ApplicationslmcgarethNo ratings yet
- AngioNet A Convolutional Neural Network For VesselDocument14 pagesAngioNet A Convolutional Neural Network For VesselFederico WeckesserNo ratings yet
- Encoder Decoder With Dense Dilated Spatial Pyramid Pooling For Prostate MRDocument8 pagesEncoder Decoder With Dense Dilated Spatial Pyramid Pooling For Prostate MRSatyaNurAnggaNo ratings yet
- 2415 14725 4 PBDocument13 pages2415 14725 4 PBFree Escort ServiceNo ratings yet
- Eano GlioblastomaDocument10 pagesEano GlioblastomaMEILYN MEDINA FAÑANo ratings yet
- ASME IMECE2019 CuttingGuides RevisedDocument7 pagesASME IMECE2019 CuttingGuides Revisedalexis jonathanNo ratings yet
- 268 2007 Article 9197Document7 pages268 2007 Article 9197Virgília GomesNo ratings yet
- Three-Dimensional Cone Beam Computed Tomography Analysis of Temporomandibular Joint Response To The Twin-Block Functional ApplianceDocument12 pagesThree-Dimensional Cone Beam Computed Tomography Analysis of Temporomandibular Joint Response To The Twin-Block Functional AppliancealejandroNo ratings yet
- Computer Methods and Programs in Biomedicine: Xiliang Zhu, Zhaoyun Cheng, Sheng Wang, Xianjie Chen, Guoqing LuDocument8 pagesComputer Methods and Programs in Biomedicine: Xiliang Zhu, Zhaoyun Cheng, Sheng Wang, Xianjie Chen, Guoqing LuTuan PhanNo ratings yet
- Use of Computer Navigation in Orthopedic OncologyDocument8 pagesUse of Computer Navigation in Orthopedic OncologyFrontiersNo ratings yet
- Image Guided Oral Implantology and Its Application in The Placement of Zygoma ImplantsDocument12 pagesImage Guided Oral Implantology and Its Application in The Placement of Zygoma ImplantsDenisa CorneaNo ratings yet
- Journal of Oral Biology and Craniofacial Research: U. Vignesh, Divya Mehrotra, Dichen, Vaibhav Anand, Debraj HowladerDocument7 pagesJournal of Oral Biology and Craniofacial Research: U. Vignesh, Divya Mehrotra, Dichen, Vaibhav Anand, Debraj Howladerlowjy119411No ratings yet
- Atlas of CT Angiography: Normal and Pathologic FindingsFrom EverandAtlas of CT Angiography: Normal and Pathologic FindingsNo ratings yet
- Amotec 12864Q DisplayDocument17 pagesAmotec 12864Q DisplayEdgarNo ratings yet
- Lighting Movements-The Fox On The FairwayDocument1 pageLighting Movements-The Fox On The FairwayabneypaigeNo ratings yet
- Our Changing WorldDocument3 pagesOur Changing Worlddinesh869863% (8)
- EmpathyDocument5 pagesEmpathyHijaab KhaanNo ratings yet
- Op CdmaDocument19 pagesOp Cdmarosev15No ratings yet
- Hydrogen Codes and Standards Workshop: Naser ChowdhuryDocument24 pagesHydrogen Codes and Standards Workshop: Naser ChowdhuryDiana DhominicNo ratings yet
- Thank You For Your Order: Power & Signal Group PO BOX 856842 MINNEAPOLIS, MN 55485-6842Document1 pageThank You For Your Order: Power & Signal Group PO BOX 856842 MINNEAPOLIS, MN 55485-6842RuodNo ratings yet
- GFB V2 - VNT Boost Controller: (Part # 3009)Document2 pagesGFB V2 - VNT Boost Controller: (Part # 3009)blumng100% (1)
- Cause and Effect PowerpointDocument20 pagesCause and Effect PowerpointSherly V.LizardoNo ratings yet
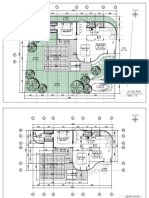
- 2023.01.25 Plan Pecatu Villa - FinishDocument3 pages2023.01.25 Plan Pecatu Villa - FinishTika AgungNo ratings yet
- Mesoamerica: Where Civilizations Flourished, and Crashed, RepeatedlyDocument8 pagesMesoamerica: Where Civilizations Flourished, and Crashed, RepeatedlyEnvyAmarr •No ratings yet
- IM300-20 (LCMass RHE 14) PDFDocument40 pagesIM300-20 (LCMass RHE 14) PDFLazzarus Az GunawanNo ratings yet
- Apple Computer Inc. v. Burst - Com, Inc. - Document No. 146Document39 pagesApple Computer Inc. v. Burst - Com, Inc. - Document No. 146Justia.comNo ratings yet
- Installation 3G Network ElementsDocument108 pagesInstallation 3G Network ElementsSDE RF WESTNo ratings yet
- Training Schedule April 2021 To March 22 - 0Document18 pagesTraining Schedule April 2021 To March 22 - 0sanrexiNo ratings yet
- Theoretical Foundations of Nursing - Review MaterialDocument10 pagesTheoretical Foundations of Nursing - Review MaterialKennethNo ratings yet
- Embryo AssignmentDocument2 pagesEmbryo AssignmentA.j. MasagcaNo ratings yet
- Animal 1414Document6 pagesAnimal 1414trialink minsanNo ratings yet
- Appendix 2-4.ep31422 - g-16Document15 pagesAppendix 2-4.ep31422 - g-16bsnegi111No ratings yet
- Case How Innovation Drives Research and DevelopmentDocument4 pagesCase How Innovation Drives Research and DevelopmentMohit KumarNo ratings yet
- CekocideDocument1 pageCekocideKaren Claire HorcaNo ratings yet
- Farm Size Factor Productivity and Returns To ScaleDocument8 pagesFarm Size Factor Productivity and Returns To ScaleAkshay YadavNo ratings yet