You might also like
- FulltextDocument19 pagesFulltextibrahimNo ratings yet
- artikel baruDocument13 pagesartikel baruErni DiahNo ratings yet
- s12884-014-0398-7.pdf 10Document13 pagess12884-014-0398-7.pdf 10Erni DiahNo ratings yet
- Willie & Callands - 2018 - Reproductive Coercion and Prenatal Distress Among Young Pregnant Women in Monrovia, LiberiaDocument8 pagesWillie & Callands - 2018 - Reproductive Coercion and Prenatal Distress Among Young Pregnant Women in Monrovia, LiberiaHerbert AmbesiNo ratings yet
- Factors Affecting Antenatal Care in EthiopiaDocument7 pagesFactors Affecting Antenatal Care in EthiopiaNuridha FauziyahNo ratings yet
- 20604-Article Text-65316-2-10-20180726 PDFDocument8 pages20604-Article Text-65316-2-10-20180726 PDFMALIK MANASRAHNo ratings yet
- fmsc110s Final PaperDocument11 pagesfmsc110s Final Paperapi-353430488No ratings yet
- Access To Childbirth CareDocument67 pagesAccess To Childbirth CareemeNo ratings yet
- Factors Influencing Breastfeeding Practices Among Mothers in Lafia LocalDocument13 pagesFactors Influencing Breastfeeding Practices Among Mothers in Lafia LocalCha Tozenity ChieNo ratings yet
- Grant ProposalDocument19 pagesGrant Proposalapi-439038470No ratings yet
- Assessment of Knowledge, Attitude and Practice Towards Anc Services Among Reproductive Age Group Women at DR Khalid MCH, in 26 June District, Hargeisa-SomalilandDocument29 pagesAssessment of Knowledge, Attitude and Practice Towards Anc Services Among Reproductive Age Group Women at DR Khalid MCH, in 26 June District, Hargeisa-SomalilandSuleekha CabdiNo ratings yet
- Utilization of Health Care Services Complete ProjectDocument54 pagesUtilization of Health Care Services Complete ProjectusmansgiremawaNo ratings yet
- Women Autonomy and Maternal Healthcare Services Utilization Among Young Ever-Married Women in NigeriaDocument12 pagesWomen Autonomy and Maternal Healthcare Services Utilization Among Young Ever-Married Women in NigeriaPi PoNo ratings yet
- CHN Reportfinalllledited2023 MmmmmvsvlatestDocument19 pagesCHN Reportfinalllledited2023 MmmmmvsvlatestShahbaz aliNo ratings yet
- Health Info Libraries J - 2017 - Kamali - Health Information Needs of Pregnant Women Information Sources Motives andDocument14 pagesHealth Info Libraries J - 2017 - Kamali - Health Information Needs of Pregnant Women Information Sources Motives andNor Hafidza Abdul HalimNo ratings yet
- Pendarahan PostpartumDocument8 pagesPendarahan PostpartumsulviNo ratings yet
- Transcultural ChildbearingDocument11 pagesTranscultural ChildbearingVerysa MaurentNo ratings yet
- Women's Perceptions of Husband Support in PregnancyDocument50 pagesWomen's Perceptions of Husband Support in Pregnancyمالك مناصرة100% (1)
- KNOWLEDGE, ATTITUDE AND PRACTICE OF FAMILY PLANNING AMONG MENDocument12 pagesKNOWLEDGE, ATTITUDE AND PRACTICE OF FAMILY PLANNING AMONG MENAmirah Mohamad SaidiNo ratings yet
- Examining The Unresolved Conundrum of Traditional Birth Attendants' Involvement in Maternal and Child Health Care Delivery in GhanaDocument20 pagesExamining The Unresolved Conundrum of Traditional Birth Attendants' Involvement in Maternal and Child Health Care Delivery in GhanafuziNo ratings yet
- Knowledge on Janani Suraksha Yojana among antenatal mothersDocument18 pagesKnowledge on Janani Suraksha Yojana among antenatal motherspallavi sharmaNo ratings yet
- Factors for Low Patronage of Healthcare Services among Women in IkoroduDocument48 pagesFactors for Low Patronage of Healthcare Services among Women in IkoroduDOYINSOLA ADENUGANo ratings yet
- Unplanned Pregnancy and Its Associated FactorsDocument11 pagesUnplanned Pregnancy and Its Associated Factorskenny. hyphensNo ratings yet
- Brenna Daly Health Research Lit ReviewDocument27 pagesBrenna Daly Health Research Lit Reviewapi-664989573No ratings yet
- 1.fp JurnalDocument14 pages1.fp Jurnal13 NOR HAZALINDA BINTI MUHAMADNo ratings yet
- Chapters 1 To 2. Incomplete. Please Double CheckDocument19 pagesChapters 1 To 2. Incomplete. Please Double CheckajdgafjsdgaNo ratings yet
- Artigo Carlota de F. Lelis Et All - 04 - 09 - 2023 - ENG - VERSIONDocument20 pagesArtigo Carlota de F. Lelis Et All - 04 - 09 - 2023 - ENG - VERSIONSilvio Omar Macedo PrietschNo ratings yet
- Epidemiology and StatisticsDocument18 pagesEpidemiology and Statisticsyatta yattaNo ratings yet
- Research Paper On Birth Preparedness and Complication ReadinessDocument10 pagesResearch Paper On Birth Preparedness and Complication ReadinesswlyxiqrhfNo ratings yet
- Ej997351 PDFDocument9 pagesEj997351 PDFSuhada AkmalNo ratings yet
- Adolescent in South AfricaDocument12 pagesAdolescent in South AfricaYoonaas AT DeebisaaNo ratings yet
- Alphatemplate ThesisDocument32 pagesAlphatemplate ThesisAizelle MangawitNo ratings yet
- Health Policy Plan. 2009 Kruk 279 88Document10 pagesHealth Policy Plan. 2009 Kruk 279 88jlventiganNo ratings yet
- Addressing Menstrual Health and Gender EquityDocument52 pagesAddressing Menstrual Health and Gender EquityShelly BhattacharyaNo ratings yet
- Timely Utilization of Parental Care For Young WomenDocument17 pagesTimely Utilization of Parental Care For Young Womenyatta yattaNo ratings yet
- Disrupting The Pathways of Social Determinants ofDocument10 pagesDisrupting The Pathways of Social Determinants ofIGA ABRAHAMNo ratings yet
- 2017 Patricia Temple Gabbe Improving Maternal and Infant Child Health Outcomes With Community Based Pregnancy Support GroupsDocument10 pages2017 Patricia Temple Gabbe Improving Maternal and Infant Child Health Outcomes With Community Based Pregnancy Support Groupsadni halianieNo ratings yet
- Teen Pregnancy Prevention Programs in Tabaco CityDocument11 pagesTeen Pregnancy Prevention Programs in Tabaco CityKevin de VeraNo ratings yet
- Pialee_Roy_Publications April 2024 (1)Document2 pagesPialee_Roy_Publications April 2024 (1)pialee royNo ratings yet
- Research PartialDocument8 pagesResearch PartialAmie VNo ratings yet
- Literature Review On Exclusive Breastfeeding in GhanaDocument8 pagesLiterature Review On Exclusive Breastfeeding in GhanaafmzxutkxdkdamNo ratings yet
- Continuing With " A Heavy Heart" - Consequences of Maternal Death in Rural KenyaDocument12 pagesContinuing With " A Heavy Heart" - Consequences of Maternal Death in Rural KenyaRayssa BrumNo ratings yet
- Journal: University of Port Harcourt of Nigeria Association For Phys Ical, HealthDocument14 pagesJournal: University of Port Harcourt of Nigeria Association For Phys Ical, Healthlivesource technologyNo ratings yet
- The Accessibility of Contraceptives and Programs - Perspectives of Employees at Rural Health Unit Barangay Poblacion, Dinalupihan BataanDocument64 pagesThe Accessibility of Contraceptives and Programs - Perspectives of Employees at Rural Health Unit Barangay Poblacion, Dinalupihan BataanAfshan HusnainNo ratings yet
- CHAPTER ONE by MohamedDocument10 pagesCHAPTER ONE by Mohamedibrahimkulow999No ratings yet
- Perception of Pregnant Women On Their Male PartnersDocument11 pagesPerception of Pregnant Women On Their Male PartnersPeteNo ratings yet
- Final CnaDocument7 pagesFinal Cnaapi-484488659No ratings yet
- Ijerph 15 02450 PDFDocument14 pagesIjerph 15 02450 PDFDeby WicaksonoNo ratings yet
- An-Najah National University: Prepared By:-1 - Bilal Mwas 2 - Omar Abureesh 3 - Yahia AbusafiDocument47 pagesAn-Najah National University: Prepared By:-1 - Bilal Mwas 2 - Omar Abureesh 3 - Yahia Abusafiمالك مناصرةNo ratings yet
- Adolescent Pregnancy in Indonesian A Literature ReviewDocument5 pagesAdolescent Pregnancy in Indonesian A Literature ReviewafmzmxkayjyosoNo ratings yet
- Utilization and Effect of Traditional Birth Attendants Among The Pregnant Women in Kahoora Division Hoima DistrictDocument13 pagesUtilization and Effect of Traditional Birth Attendants Among The Pregnant Women in Kahoora Division Hoima DistrictKIU PUBLICATION AND EXTENSIONNo ratings yet
- Jurnal Ebn 2Document9 pagesJurnal Ebn 2siska khairNo ratings yet
- 147 328 1 SMDocument7 pages147 328 1 SMAlmaisa Kinudung SalsabilaNo ratings yet
- Jurnal Inter Tanda Bahaya KehamilanDocument8 pagesJurnal Inter Tanda Bahaya Kehamilanrina astutiNo ratings yet
- Yahaya Mohammed Research 2024Document6 pagesYahaya Mohammed Research 2024emidibo4503No ratings yet
- 2019 Article 729Document18 pages2019 Article 729api-625120170No ratings yet
- Final Sima Research File (Autorecovered)Document13 pagesFinal Sima Research File (Autorecovered)Devendra MallaNo ratings yet
- Catherine ProposalDocument10 pagesCatherine ProposalAlphajor JallohNo ratings yet
- ThesissssDocument30 pagesThesissssPearl Joy Villagomeza IINo ratings yet
- Chelsea Ruthrauff: RN, BSN, PHNDocument1 pageChelsea Ruthrauff: RN, BSN, PHNChelsea RuthrauffNo ratings yet
- Case Study 10Document3 pagesCase Study 10Chelsea RuthrauffNo ratings yet
- Letter of Rec Sherri BrownDocument1 pageLetter of Rec Sherri BrownChelsea RuthrauffNo ratings yet
- Sentinel Event PaperDocument18 pagesSentinel Event PaperChelsea RuthrauffNo ratings yet
- Diabetic Ketoacidosis (DKA) : Cindy, Chelsea, Kim, JessaDocument11 pagesDiabetic Ketoacidosis (DKA) : Cindy, Chelsea, Kim, JessaChelsea RuthrauffNo ratings yet
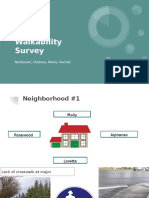
- Ceres Walkability Survey: Nathaniel, Chelsea, Maria, RachelDocument13 pagesCeres Walkability Survey: Nathaniel, Chelsea, Maria, RachelChelsea RuthrauffNo ratings yet
- Preventative Teach ProjectDocument15 pagesPreventative Teach ProjectChelsea RuthrauffNo ratings yet
- Group Lit Rev PaperDocument15 pagesGroup Lit Rev PaperChelsea RuthrauffNo ratings yet
- Mental Health Case StudyDocument24 pagesMental Health Case StudyChelsea RuthrauffNo ratings yet
- Anorexia Brochure - OutsideDocument2 pagesAnorexia Brochure - OutsideChelsea RuthrauffNo ratings yet
- Hand Hygiene: By: Chelsea RuthrauffDocument9 pagesHand Hygiene: By: Chelsea RuthrauffChelsea RuthrauffNo ratings yet
- Nurs 4400 CH Worksheet 9 Global HealthDocument3 pagesNurs 4400 CH Worksheet 9 Global HealthChelsea RuthrauffNo ratings yet
- Transcultural InterviewDocument13 pagesTranscultural InterviewChelsea RuthrauffNo ratings yet
- Case Study 24Document6 pagesCase Study 24Chelsea RuthrauffNo ratings yet
- DKA Paper PDFDocument8 pagesDKA Paper PDFChelsea RuthrauffNo ratings yet
- CertificatesDocument7 pagesCertificatesChelsea RuthrauffNo ratings yet
- Care Plan 4Document31 pagesCare Plan 4Chelsea RuthrauffNo ratings yet
- Case Study 45Document5 pagesCase Study 45Chelsea RuthrauffNo ratings yet
- Teaching Project-Hand Hygiene in Elementary Schools PDFDocument6 pagesTeaching Project-Hand Hygiene in Elementary Schools PDFChelsea RuthrauffNo ratings yet
- Beliefs and EthicsDocument5 pagesBeliefs and EthicsChelsea RuthrauffNo ratings yet
- M Flores - InNOut PDFDocument1 pageM Flores - InNOut PDFChelsea RuthrauffNo ratings yet
- Ceres Windshield SurveyDocument13 pagesCeres Windshield SurveyChelsea Ruthrauff100% (1)
- Global Health Paper 2Document18 pagesGlobal Health Paper 2Chelsea RuthrauffNo ratings yet
- Care Plan 3Document30 pagesCare Plan 3Chelsea RuthrauffNo ratings yet
- Letter of Rec Sherri BrownDocument1 pageLetter of Rec Sherri BrownChelsea RuthrauffNo ratings yet
- Running Head: Family/Child Assessment 1Document18 pagesRunning Head: Family/Child Assessment 1Chelsea RuthrauffNo ratings yet
- Maternal Mortality in Sierra LeoneDocument15 pagesMaternal Mortality in Sierra LeoneChelsea RuthrauffNo ratings yet
- Sentinel Event PaperDocument18 pagesSentinel Event PaperChelsea RuthrauffNo ratings yet
- Case Study 10Document3 pagesCase Study 10Chelsea RuthrauffNo ratings yet
- Mental Health Case StudyDocument24 pagesMental Health Case StudyChelsea RuthrauffNo ratings yet
- Culture Level On Patient Safety in Nursing StaffDocument13 pagesCulture Level On Patient Safety in Nursing StaffInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Water Stories - Expanding Opportunities in Small Scale Water and Sanitation Projects - WicsDocument98 pagesWater Stories - Expanding Opportunities in Small Scale Water and Sanitation Projects - WicsritaffgNo ratings yet
- Kair Profile DressCompanyDocument24 pagesKair Profile DressCompanySreenivas Chowdary VaddineniNo ratings yet
- CPE5601 Diagnosis and Treatment of Feeding and Eating DisordersDocument16 pagesCPE5601 Diagnosis and Treatment of Feeding and Eating DisordersSiti MuslihaNo ratings yet
- Iep Worksheet ActivitiesDocument7 pagesIep Worksheet Activitiesapi-346406650No ratings yet
- Health Care, Management & Entrepreneurship: A Report Submitted To Prof. Ratan JalanDocument4 pagesHealth Care, Management & Entrepreneurship: A Report Submitted To Prof. Ratan JalanDEEPANSHU SINGHNo ratings yet
- PBL and NDXDocument15 pagesPBL and NDXJasmin AdoraNo ratings yet
- Harry Guess, Linda Engel, Arthur Kleinman, John Kusek Science of The Placebo Toward An Interdisciplinanary Research Agenda Evidence-Based Medicine Workbks. 2002Document345 pagesHarry Guess, Linda Engel, Arthur Kleinman, John Kusek Science of The Placebo Toward An Interdisciplinanary Research Agenda Evidence-Based Medicine Workbks. 2002rockspirit02No ratings yet
- Bwcs Feedback Final September 2023Document56 pagesBwcs Feedback Final September 2023Babloo50% (2)
- Cases On InflammationDocument3 pagesCases On InflammationAijan Murzalieva0% (1)
- Ulkus DekubitusDocument33 pagesUlkus DekubitusNurul FadilahNo ratings yet
- Dysfunctional Uterine Bleeding History CollectionDocument4 pagesDysfunctional Uterine Bleeding History CollectionAnitha BalakrishnanNo ratings yet
- Report To The New York City Board of CorrectionDocument20 pagesReport To The New York City Board of CorrectionGotham GazetteNo ratings yet
- OR 01a FCDocument12 pagesOR 01a FCfritzrose50% (2)
- Ncp. Pedia.Document2 pagesNcp. Pedia.Czarina MayoNo ratings yet
- Fast Food Nation EssayDocument5 pagesFast Food Nation EssayBen SmithNo ratings yet
- Dakota Horizons BrochureDocument2 pagesDakota Horizons Brochurekatie_krebsbach_1No ratings yet
- American Medical AbbreviationDocument11 pagesAmerican Medical AbbreviationJacquelineNo ratings yet
- Module 7: Stating The Biopsychosocial Theories of Crime CausationDocument13 pagesModule 7: Stating The Biopsychosocial Theories of Crime CausationNADAL NICA JOY L.100% (1)
- Autosomal Recessive InheritanceDocument8 pagesAutosomal Recessive InheritanceShatasree MazumdarNo ratings yet
- Aubf Lab 7Document1 pageAubf Lab 7Regina SalazarNo ratings yet
- Assignment-I Business Statistics: TOPIC: Abbott India LTDDocument14 pagesAssignment-I Business Statistics: TOPIC: Abbott India LTDAbhishek MohanpuriaNo ratings yet
- Preparing For Face-To-Face Classes: Better DaysDocument3 pagesPreparing For Face-To-Face Classes: Better DaysMaria Cristina LolosNo ratings yet
- Nepal 3 Year Interim Plan EngDocument42 pagesNepal 3 Year Interim Plan Engparbatdhungana100% (1)
- ReferenceDocument4 pagesReferenceStephani LeticiaNo ratings yet
- By: Dr. Ayman Bukhari House Officer Obstetrics & GynaecologyDocument54 pagesBy: Dr. Ayman Bukhari House Officer Obstetrics & GynaecologyBharat ThapaNo ratings yet
- Pharma Sales Crediting Incentives For Accurate and Compliant Processes Codex3444Document11 pagesPharma Sales Crediting Incentives For Accurate and Compliant Processes Codex3444pranali100% (2)
- Details of Indian companies incorporated between 13 February and 13 March 2020Document1,620 pagesDetails of Indian companies incorporated between 13 February and 13 March 2020GorrillaNo ratings yet
- Social Media For Health Promotion and Weight Management: A Critical DebateDocument7 pagesSocial Media For Health Promotion and Weight Management: A Critical Debateasep9ustomNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)