You might also like
- Female Genitalia - Physical ExaminationDocument33 pagesFemale Genitalia - Physical Examinationmulatumelese67% (3)
- DC Osce ScriptDocument5 pagesDC Osce ScriptKaren GumabonNo ratings yet
- Perineal and Cervical TearsDocument43 pagesPerineal and Cervical TearsN. SivaNo ratings yet
- Rupture PerineumDocument26 pagesRupture PerineumMarcellRaymondNo ratings yet
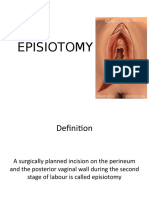
- EPISIOTOMY FinalDocument30 pagesEPISIOTOMY FinalBindu PhilipNo ratings yet
- Genital Tract InjuriesDocument19 pagesGenital Tract InjuriesMarvella Nongkhar100% (1)
- Actual Birth SimulationDocument47 pagesActual Birth SimulationBSN 1A- Serrano Evytte Joy B.No ratings yet
- Newborn Assessment and CareDocument17 pagesNewborn Assessment and CareMatthew Lee100% (1)
- EINC RetdemDocument11 pagesEINC RetdemKENSEY MOORE EBROLENo ratings yet
- Female GenitaliaDocument96 pagesFemale GenitaliaJopaii TanakaNo ratings yet
- Manual Removal of PlacentaDocument12 pagesManual Removal of PlacentaBhawna JoshiNo ratings yet
- ANA.S4.CA21.Female Reproductive SystempdfDocument6 pagesANA.S4.CA21.Female Reproductive SystempdfCazz HeyNo ratings yet
- Gynecological History Taking and ExaminationDocument17 pagesGynecological History Taking and Examinationnmsiswaridewi100% (1)
- Manual Removal of PlacentaDocument10 pagesManual Removal of PlacentaSanthosh.S.UNo ratings yet
- Einc NotesDocument6 pagesEinc NotesMaria Ivy Rochelle TanNo ratings yet
- Edited Maternal ProcedureDocument45 pagesEdited Maternal ProcedureClare Alcober100% (1)
- Cord Care ProceduresDocument3 pagesCord Care ProceduresJasmin AdoraNo ratings yet
- Pelvic Examination: Liezel B. Cauilan MSN, MSTDocument25 pagesPelvic Examination: Liezel B. Cauilan MSN, MSTSIR ONENo ratings yet
- FundamentalsDocument34 pagesFundamentalsColleen CalditoNo ratings yet
- Retdem ReviewerDocument2 pagesRetdem Reviewerjustinejeon6No ratings yet
- This Information Sheet Aims To Answer Some Commonly Asked Questions About Perineal Tears. Ask Your Doctor or Midwife About What Care Is Right For YouDocument2 pagesThis Information Sheet Aims To Answer Some Commonly Asked Questions About Perineal Tears. Ask Your Doctor or Midwife About What Care Is Right For YouFarida ParvinNo ratings yet
- Episiotomy Repair GuideDocument5 pagesEpisiotomy Repair GuideAnila SajeshNo ratings yet
- Pelvic ExamDocument6 pagesPelvic ExamJaigurudev Ashi SanskarNo ratings yet
- Physical Assessment of The GentialiaDocument48 pagesPhysical Assessment of The GentialiaWilliam Lim100% (2)
- Episiotomy TeachingDocument16 pagesEpisiotomy TeachingkamalbakshirNo ratings yet
- Procedure On Peforming and Suturing EpisiotomyDocument2 pagesProcedure On Peforming and Suturing Episiotomyshivani dasNo ratings yet
- Retained PlacentaDocument30 pagesRetained PlacentaNejib M/AminNo ratings yet
- Suturing Perineal LacerationsDocument49 pagesSuturing Perineal LacerationsOfel Santillan100% (2)
- H, A Hernia AssmntDocument11 pagesH, A Hernia AssmntromaaNo ratings yet
- Female Reproductive System Assessment22Document12 pagesFemale Reproductive System Assessment22pravina praviNo ratings yet
- Tucking HandoutDocument2 pagesTucking HandoutWilma PurwaniNo ratings yet
- Mannual Removal of Placenta: Presented By-Bhawna Joshi MSC. (N) 2 YearDocument23 pagesMannual Removal of Placenta: Presented By-Bhawna Joshi MSC. (N) 2 YearBhawna JoshiNo ratings yet
- Abortion HandoutDocument9 pagesAbortion HandoutVICTORIA KWAYNo ratings yet
- NCM101RLE Gribador Jayne Feline JDocument7 pagesNCM101RLE Gribador Jayne Feline JJAYNE FELINE GRIBADORNo ratings yet
- MINOR SX 2 Clinical Breast ExaminationDocument18 pagesMINOR SX 2 Clinical Breast ExaminationVinna AlvarezNo ratings yet
- BandagingDocument14 pagesBandagingRitaNo ratings yet
- Wound Care Signs, Treatment and Home CareDocument3 pagesWound Care Signs, Treatment and Home CareMa Corazon MelecioNo ratings yet
- Digital Rectal ExaminationDocument21 pagesDigital Rectal Examinationmegahed7320000No ratings yet
- Discharge Planning EnglishDocument11 pagesDischarge Planning Englishrahmat hidayatNo ratings yet
- Birth Canal Injuries Final LectureDocument63 pagesBirth Canal Injuries Final Lecturepeter njoguNo ratings yet
- Manual Removal of Retained Placenta GuideDocument25 pagesManual Removal of Retained Placenta GuideLoorthu Selvi M0% (1)
- Episiotomyprocedure 220126053356Document45 pagesEpisiotomyprocedure 220126053356nellius mutindiNo ratings yet
- 2 Skin Preparation and DrapingDocument34 pages2 Skin Preparation and Drapingclaire yowsNo ratings yet
- Checklist - Catheterization 1Document4 pagesChecklist - Catheterization 1Carlyn AguasNo ratings yet
- Mastectomy: Prepared By: Hilario, Eunice Lamoste, Jenebelle Lopez, Maria SofiaDocument34 pagesMastectomy: Prepared By: Hilario, Eunice Lamoste, Jenebelle Lopez, Maria SofiaSofia LopezNo ratings yet
- Wound Types and Treatment GuideDocument4 pagesWound Types and Treatment GuideNikki Ann Kanapi FernandezNo ratings yet
- Gynaecology Exam GuideDocument15 pagesGynaecology Exam GuidePraveena MoganNo ratings yet
- BSSC - IndonesiaDocument84 pagesBSSC - IndonesiaInomy ClaudiaNo ratings yet
- Introduction To First AidDocument61 pagesIntroduction To First AidLim Jun BinNo ratings yet
- Splinting Techniques: by Madhumitha M, Aruna G, Abi P, Sakthivelayudham G, Sujidha R, Srivignesh MDocument99 pagesSplinting Techniques: by Madhumitha M, Aruna G, Abi P, Sakthivelayudham G, Sujidha R, Srivignesh MSakthivelayudhamganesanNo ratings yet
- Pelvic ExaminationDocument24 pagesPelvic ExaminationVictor SantawiNo ratings yet
- EPISIOTOMYDocument9 pagesEPISIOTOMYkailash chand atal100% (1)
- First Aid KitDocument18 pagesFirst Aid KitGianni100% (1)
- First Aid Dressing BandagesDocument23 pagesFirst Aid Dressing BandagesLawrence cruzanaNo ratings yet
- Using The Canister MethodDocument4 pagesUsing The Canister MethodcodytlseNo ratings yet
- Suturing Perineal Lacerations EditedDocument5 pagesSuturing Perineal Lacerations EditedJanzell Anne Borja AlbaniaNo ratings yet
- Perineal TearsDocument44 pagesPerineal TearsMagic_OverNo ratings yet
- MDWF 3030 Practice Guideline Intrahepatic Cholestasis in Pregnancy Icp 2Document3 pagesMDWF 3030 Practice Guideline Intrahepatic Cholestasis in Pregnancy Icp 2api-442131145No ratings yet
- MDWF 3030 Emergency Care PlanDocument2 pagesMDWF 3030 Emergency Care Planapi-442131145No ratings yet
- Practice Guideline Vaginal BleedingDocument3 pagesPractice Guideline Vaginal Bleedingapi-442131145No ratings yet
- MDWF 3030 Practice Guideline Chorioamnionitis 1Document3 pagesMDWF 3030 Practice Guideline Chorioamnionitis 1api-442131145No ratings yet
- MDWF 3030 Urinary Catheterization Intrapartum PostpartumDocument2 pagesMDWF 3030 Urinary Catheterization Intrapartum Postpartumapi-442131145No ratings yet
- MDWF 3010 3Document15 pagesMDWF 3010 3api-442131145No ratings yet
- MDWF 2070 - 12Document4 pagesMDWF 2070 - 12api-442131145No ratings yet
- Biol 2050 8Document1 pageBiol 2050 8api-442131145No ratings yet
- Taylor Rackey ResumeDocument3 pagesTaylor Rackey Resumeapi-442131145No ratings yet
- MDWF 2060 - Intrahepatic Cholestasis of Pregnancy IcpDocument1 pageMDWF 2060 - Intrahepatic Cholestasis of Pregnancy Icpapi-442131145No ratings yet
- CLNC 2040 Reflection of Assistant ExperiencesDocument4 pagesCLNC 2040 Reflection of Assistant Experiencesapi-442131145No ratings yet
- MDWF 2050 9Document2 pagesMDWF 2050 9api-442131145No ratings yet
- CLNC 3010 Reflection of Primary ExperiencesDocument3 pagesCLNC 3010 Reflection of Primary Experiencesapi-442131145No ratings yet
- Stat 2050 Assignment 3 Data AnalysisDocument4 pagesStat 2050 Assignment 3 Data Analysisapi-442131145No ratings yet
- MDWF 2020 4Document4 pagesMDWF 2020 4api-442131145No ratings yet
- MDWF 3060 15Document8 pagesMDWF 3060 15api-442131145No ratings yet
- MDWF 2040 Practice Guideline Postpartum AnemiaDocument4 pagesMDWF 2040 Practice Guideline Postpartum Anemiaapi-442131145No ratings yet
- CLNC 2030 Reflection of Assistance ExperiencesDocument3 pagesCLNC 2030 Reflection of Assistance Experiencesapi-442131145No ratings yet
- MDWF 2070 Drug Protocol ErthyromycinDocument1 pageMDWF 2070 Drug Protocol Erthyromycinapi-442131145No ratings yet
- MDWF 2100 Practice Guideline ChlamydiaDocument3 pagesMDWF 2100 Practice Guideline Chlamydiaapi-442131145No ratings yet
- MDWF 2070 Drug Protocol Vitamin KDocument1 pageMDWF 2070 Drug Protocol Vitamin Kapi-442131145No ratings yet
- MDWF 2090 - Ongoing PP Support Care For The PerineumDocument4 pagesMDWF 2090 - Ongoing PP Support Care For The Perineumapi-442131145No ratings yet
- Comm 2010 - 3Document2 pagesComm 2010 - 3api-442131145No ratings yet
- MDWF 2030 Assignment 2Document1 pageMDWF 2030 Assignment 2api-442131145No ratings yet
- CLNC 2020 Reflection On Assistant ExperiencesDocument3 pagesCLNC 2020 Reflection On Assistant Experiencesapi-442131145No ratings yet
- MDWF 2030 Assignment 2Document6 pagesMDWF 2030 Assignment 2api-442131145No ratings yet
- MDWF 2090 How To Perform 2nd Degree RepairsDocument3 pagesMDWF 2090 How To Perform 2nd Degree Repairsapi-442131145No ratings yet
- MDWF 2010 3Document3 pagesMDWF 2010 3api-442131145No ratings yet
- CLNC 2010 Reflection of Assist ExperiencesDocument4 pagesCLNC 2010 Reflection of Assist Experiencesapi-442131145No ratings yet
- Pelvic ExaminationDocument24 pagesPelvic ExaminationVictor SantawiNo ratings yet
- Asuhan Keperawatan Di Instalasi Gawat DaruratDocument5 pagesAsuhan Keperawatan Di Instalasi Gawat DaruratDyah PerwaNo ratings yet
- Perineum & Urogenital TriangleDocument3 pagesPerineum & Urogenital TriangleameerabestNo ratings yet
- Obstetrical Anal Sphincter Injuries (Oasis) : A Repair GuideDocument30 pagesObstetrical Anal Sphincter Injuries (Oasis) : A Repair GuideKenneth SyNo ratings yet
- FDARDocument2 pagesFDARrodolfo opido100% (2)
- Pelvic and PerineumDocument20 pagesPelvic and PerineumRahaf MajadlyNo ratings yet
- Rovielyn P. Ogayre Pt-11 Anaphy: Scalp Muscles Scalp MuscleDocument45 pagesRovielyn P. Ogayre Pt-11 Anaphy: Scalp Muscles Scalp MuscleRovielyn P OgayreNo ratings yet
- 300 LevelDocument4 pages300 LevelAkinsola AyomidotunNo ratings yet
- GENITAL PROLAPSE GUIDEDocument58 pagesGENITAL PROLAPSE GUIDEsushma nakkinaNo ratings yet
- Anatomy in Practice: The Ischiorectal FossaeDocument4 pagesAnatomy in Practice: The Ischiorectal FossaeAjay Pal NattNo ratings yet
- Acu YogaDocument7 pagesAcu YogaB107 Luh Putu Heppy IndrawatiNo ratings yet
- Birth Is Not An IllnessDocument13 pagesBirth Is Not An IllnessacebanditsNo ratings yet
- 51episiotomyDocument21 pages51episiotomyJay SeetohulNo ratings yet
- Everything You Need to Know About EpisiotomiesDocument18 pagesEverything You Need to Know About EpisiotomiesAnnapurna DangetiNo ratings yet
- Genital Trauma - Dr. IndriDocument40 pagesGenital Trauma - Dr. IndriIzar AzwarNo ratings yet
- Grade Ruptur RosadeDocument31 pagesGrade Ruptur RosadeAntoniusNo ratings yet
- NCM 107 SKL FinalsDocument33 pagesNCM 107 SKL FinalsCyriz Ann Mae PacisNo ratings yet
- Tobias 94 - The Rectum - Part 3 - QuestionsDocument2 pagesTobias 94 - The Rectum - Part 3 - QuestionsCarlos Rubiños AlonsoNo ratings yet
- EPISIOTOMYDocument1 pageEPISIOTOMYmealiellaNo ratings yet
- Episiotomy ACOG PDFDocument29 pagesEpisiotomy ACOG PDFFebyan AbotNo ratings yet
- Pelvic Bone MCQDocument6 pagesPelvic Bone MCQWan Ahmad FaizFaizalNo ratings yet
- Clinical Anatomy of The Vulva, Vagina, Lower Pelvis, and PerineumDocument20 pagesClinical Anatomy of The Vulva, Vagina, Lower Pelvis, and PerineumJacobMsangNo ratings yet
- Instructions: Soothes - Moisturizes - ProtectsDocument2 pagesInstructions: Soothes - Moisturizes - ProtectsNoor ElbadriNo ratings yet
- Perineal TearsDocument49 pagesPerineal TearsvisakhaNo ratings yet
- Perineal RuptureDocument24 pagesPerineal RuptureIzz ShuhaimiNo ratings yet
- PERINEAL FLUSHINGrev 3Document34 pagesPERINEAL FLUSHINGrev 3Michelle FactoNo ratings yet
- Approach To Episiotomy - UpToDateDocument13 pagesApproach To Episiotomy - UpToDatePedro Vilches Polaina100% (1)
- Urology NotesDocument811 pagesUrology Notes1cmNo ratings yet
- Cloacal Malformation Variant in A Male Neonate: Case ReportDocument3 pagesCloacal Malformation Variant in A Male Neonate: Case ReportIndra JayaNo ratings yet
- WHO Recommendation On Techniques For Preventing Perineal Trauma During Labour - RHL PDFDocument19 pagesWHO Recommendation On Techniques For Preventing Perineal Trauma During Labour - RHL PDFsaksNo ratings yet