You might also like
- The Borderline Personality Disorder Workbook by Daniel J. Fox, PHDDocument35 pagesThe Borderline Personality Disorder Workbook by Daniel J. Fox, PHDMegan Hale90% (10)
- Military Medical ManualsDocument636 pagesMilitary Medical ManualsDark MonsterNo ratings yet
- Anatomy of Brain and Function - NaemaDocument7 pagesAnatomy of Brain and Function - NaemaHana Naema ZelinNo ratings yet
- Clinician's Guide to Chronic Disease Management of Long Term Conditions, TheFrom EverandClinician's Guide to Chronic Disease Management of Long Term Conditions, TheNo ratings yet
- How To Deal With Dilemmas Hard Decisions and Tough Choices - Russ HarrisDocument10 pagesHow To Deal With Dilemmas Hard Decisions and Tough Choices - Russ HarrisYong ChenNo ratings yet
- Jurnal Kedokteran Dan Kesehatan Indonesia: Risk Factors of Stroke Survivors' Quality of LifeDocument7 pagesJurnal Kedokteran Dan Kesehatan Indonesia: Risk Factors of Stroke Survivors' Quality of LifeEster YunitaNo ratings yet
- Early Occupational Therapy Intervention in The Hospital Discharge After StrokeDocument11 pagesEarly Occupational Therapy Intervention in The Hospital Discharge After Strokeali veliNo ratings yet
- One-Year Outcomes in CaregiversDocument11 pagesOne-Year Outcomes in Caregiversgiovanni311094No ratings yet
- SurajbkanaseDocument6 pagesSurajbkanaseAnonymous Ezsgg0VSENo ratings yet
- Care Giver Burdan in ParkinsonDocument8 pagesCare Giver Burdan in ParkinsonPurnandu SharmaNo ratings yet
- Anna PIECZYŃSKA 2022Document9 pagesAnna PIECZYŃSKA 2022PPDS Rehab Medik UnhasNo ratings yet
- ARRCT - 2020 Chakrabarty Et AlDocument11 pagesARRCT - 2020 Chakrabarty Et AlMadhushree ChakrabartyNo ratings yet
- Quality of Life of Caregivers of Patients Diagnosed With SevereDocument10 pagesQuality of Life of Caregivers of Patients Diagnosed With SeverejlbermudezcNo ratings yet
- 2007 Graff EffectofcommunityoccupationaltherqualitylifemoodhealthstatusDocument9 pages2007 Graff EffectofcommunityoccupationaltherqualitylifemoodhealthstatusSamantha ColleNo ratings yet
- Impact of Cognitive Impairment On MildDocument12 pagesImpact of Cognitive Impairment On MildCristina MPNo ratings yet
- Family Medicine & Medical Science ResearchDocument9 pagesFamily Medicine & Medical Science ResearchAndhika DNo ratings yet
- 1 Effect of Mood On Long Term Disability in Younger Stroke SurvivorsDocument10 pages1 Effect of Mood On Long Term Disability in Younger Stroke SurvivorsHanin MaharNo ratings yet
- 10 JMSCRDocument10 pages10 JMSCRMultazamNo ratings yet
- Jurnal 2Document8 pagesJurnal 2FirlyyNo ratings yet
- Psychiatric Survey - IJCMPHDocument6 pagesPsychiatric Survey - IJCMPHDr Deepthi GillaNo ratings yet
- Knowledge, Attitude, and Practice in Management of Patients With Mental Health Disorders in Emergency Departments in Makkah Region of Saudi ArabiaDocument8 pagesKnowledge, Attitude, and Practice in Management of Patients With Mental Health Disorders in Emergency Departments in Makkah Region of Saudi ArabiaIJAR JOURNALNo ratings yet
- Gurr2011-Probleme Psihologice Dupa Atac CerebralDocument9 pagesGurr2011-Probleme Psihologice Dupa Atac CerebralPaulNo ratings yet
- Role of Sertraline in Posttraumatic Brain Injury Depression and Quality-Of-Life in TBIDocument7 pagesRole of Sertraline in Posttraumatic Brain Injury Depression and Quality-Of-Life in TBIFaiz NazriNo ratings yet
- Life Quality of Patients Suffering Cerebral Stroke: Sidita Haxholli, Caterina Gruosso, Gennaro Rocco, Enzo RubertiDocument10 pagesLife Quality of Patients Suffering Cerebral Stroke: Sidita Haxholli, Caterina Gruosso, Gennaro Rocco, Enzo RubertiijasrjournalNo ratings yet
- Kart Tune N 2010Document10 pagesKart Tune N 2010AndreiaNo ratings yet
- Vivir Con ParkinsonDocument22 pagesVivir Con ParkinsonAlexis Muñoz TrincadoNo ratings yet
- Body Mass IndexDocument6 pagesBody Mass Indexayu yuliantiNo ratings yet
- 1 s2.0 S0883941722000905 MainDocument11 pages1 s2.0 S0883941722000905 MainReni Tri AstutiNo ratings yet
- Plagiarism ThesisDocument36 pagesPlagiarism ThesiskhadijjatariqNo ratings yet
- 1 s2.0 S0003999320303841 MainDocument9 pages1 s2.0 S0003999320303841 MainAFRIDATUS SAFIRANo ratings yet
- Psychiatric Morbidity, Quality of Life and Caregiver Burden in Patients Undergoing HemodialysisDocument6 pagesPsychiatric Morbidity, Quality of Life and Caregiver Burden in Patients Undergoing HemodialysispriyadikkalaNo ratings yet
- Perceptions, Attitude and Practices Toward Elderly Depression Among Primary Health Care Physicians, Riyadh, Saudi Arabia 2021Document9 pagesPerceptions, Attitude and Practices Toward Elderly Depression Among Primary Health Care Physicians, Riyadh, Saudi Arabia 2021IJAR JOURNALNo ratings yet
- The Quality of Life of Breast Cancer Patients, Experience of The Mohamed 6 Center For The Treatment of Gynecological Breast CancerDocument19 pagesThe Quality of Life of Breast Cancer Patients, Experience of The Mohamed 6 Center For The Treatment of Gynecological Breast CancerIJAR JOURNALNo ratings yet
- Jurnal PD 4Document11 pagesJurnal PD 4Jay MNo ratings yet
- Functioning in Schizophrenia: A Delphi Study Covering The Perspective of PhysiotherapistsDocument9 pagesFunctioning in Schizophrenia: A Delphi Study Covering The Perspective of Physiotherapistsyalocim666No ratings yet
- The Influence of Psychological Intervention On Cognitive Appraisal and Level of Anxiety in Dialysis Patients: A Pilot StudyDocument4 pagesThe Influence of Psychological Intervention On Cognitive Appraisal and Level of Anxiety in Dialysis Patients: A Pilot StudyoanacrisNo ratings yet
- Longitudinal Impact of Depression On Quality of Life in Stroke PatientsDocument6 pagesLongitudinal Impact of Depression On Quality of Life in Stroke PatientsGeorgiana Vlad (Bisoceanu)No ratings yet
- Job Related Stress in Psychiatric NursesDocument8 pagesJob Related Stress in Psychiatric Nursesezinne obinna-umaNo ratings yet
- Nhosppsych 2020 06 017Document23 pagesNhosppsych 2020 06 017aieyha hamkaNo ratings yet
- Self-Care Self-Efficacy Correlates With Independence in Basic Activities of Daily Living in Individuals With Chronic StrokeDocument7 pagesSelf-Care Self-Efficacy Correlates With Independence in Basic Activities of Daily Living in Individuals With Chronic StrokeSitti Rosdiana YahyaNo ratings yet
- Articulo 2Document9 pagesArticulo 2Rommel AndresNo ratings yet
- TurkeyDocument10 pagesTurkeySandra RNo ratings yet
- Quality of Life in Glaucoma: A Review of The LiteratureDocument23 pagesQuality of Life in Glaucoma: A Review of The LiteratureMakhda Nurfatmala LNo ratings yet
- A Study To Assess The Quality of Life of Patients With Osteoarthritis in A Selected Hospital, Coimbatore, With A View To Develop An Informational BookletDocument5 pagesA Study To Assess The Quality of Life of Patients With Osteoarthritis in A Selected Hospital, Coimbatore, With A View To Develop An Informational BookletInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Journal Homepage: - : IntroductionDocument9 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Determinan Beban Pengasuh Pasien Stroke 07d33b9dDocument6 pagesDeterminan Beban Pengasuh Pasien Stroke 07d33b9drahmat alfi syahriNo ratings yet
- Quality-Of-Life Predictor Factors in Patients With SLE and Their Modification After Cognitive Behavioural TherapyDocument8 pagesQuality-Of-Life Predictor Factors in Patients With SLE and Their Modification After Cognitive Behavioural TherapyRiska Resty WasitaNo ratings yet
- Six-Month Neuropsychological Outcome of Medical Intensive Care Unit PatientsDocument9 pagesSix-Month Neuropsychological Outcome of Medical Intensive Care Unit PatientsYamile Cetina CaheroNo ratings yet
- Effectiveness of Vortioxetine in Patients With Major Depressive Disorder and Early-Stage Dementia - The MEMORY StudyDocument32 pagesEffectiveness of Vortioxetine in Patients With Major Depressive Disorder and Early-Stage Dementia - The MEMORY Studymalebranche18No ratings yet
- Burden and Quality of Life of Caregivers For Hemodialysis PatientsDocument8 pagesBurden and Quality of Life of Caregivers For Hemodialysis PatientsAsim EisaNo ratings yet
- Caregiver BurdenDocument17 pagesCaregiver BurdenAlam Zeb Khattak 70-FSS/PHDPSY/F18No ratings yet
- Journal Homepage: - : Manuscript HistoryDocument8 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Nishinaga CGA and Team InterventionDocument6 pagesNishinaga CGA and Team InterventioninunNo ratings yet
- Effects of Resilience On Quality of Life in Patients With Bipolar DisorderDocument8 pagesEffects of Resilience On Quality of Life in Patients With Bipolar DisorderAdina SpanacheNo ratings yet
- 16 - Gok UgurDocument12 pages16 - Gok Ugurmilan seniNo ratings yet
- Indian J Psychiatry Skizo Impact On QoLDocument12 pagesIndian J Psychiatry Skizo Impact On QoLAnonymous hvOuCjNo ratings yet
- 488-Article Text-2072-1-10-20201119Document12 pages488-Article Text-2072-1-10-20201119haslinaNo ratings yet
- Quality of Life in Caregivers of Aged Stroke Survivors in Southern BrazilDocument16 pagesQuality of Life in Caregivers of Aged Stroke Survivors in Southern BrazilDaniel M. FernandesNo ratings yet
- Diff Erences in Cognitive Function and Daily Living Skills Between Early-And Late-Stage SchizophreniaDocument8 pagesDiff Erences in Cognitive Function and Daily Living Skills Between Early-And Late-Stage SchizophreniaRenny TjahjaNo ratings yet
- Determining Factors of Quality of Life of Care Givers of Palliative Care Cancer PatientsDocument8 pagesDetermining Factors of Quality of Life of Care Givers of Palliative Care Cancer PatientsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Relationships Between Activity and Well-Being in People WithDocument8 pagesRelationships Between Activity and Well-Being in People WithDiego andisNo ratings yet
- Apd 2017022115522837Document15 pagesApd 2017022115522837Azzahra JihanNo ratings yet
- Articulo 5Document8 pagesArticulo 5Laura Ramos VieitesNo ratings yet
- A Systematic Review of Rehabilitation Interventions To Prevent and Treat Depression in Post-Stroke AphasiaDocument24 pagesA Systematic Review of Rehabilitation Interventions To Prevent and Treat Depression in Post-Stroke AphasiaJose Alonso Aguilar ValeraNo ratings yet
- Increasing Height 5 Tips To Grow Taller Even After Puberty The Times of IndiaDocument6 pagesIncreasing Height 5 Tips To Grow Taller Even After Puberty The Times of Indiawhite hatNo ratings yet
- City Ordinance No.241: An Ordinance On Rabies Control and Eradication in Zamboanga CityDocument8 pagesCity Ordinance No.241: An Ordinance On Rabies Control and Eradication in Zamboanga CityArman BentainNo ratings yet
- RMM Journal Club GuideDocument4 pagesRMM Journal Club GuideDan MateiNo ratings yet
- Current Transcriber Test TextDocument1 pageCurrent Transcriber Test TextTalking Cats PlaytimeNo ratings yet
- Toxic Positivity (An Essay)Document2 pagesToxic Positivity (An Essay)Colossal HeartNo ratings yet
- Profile PDFDocument1 pageProfile PDFAnnasai PramNo ratings yet
- New Principles in Pilon Fractres ManagementDocument17 pagesNew Principles in Pilon Fractres ManagementCamila FontechaNo ratings yet
- ResponsibleRestart Ohio: County FairsDocument2 pagesResponsibleRestart Ohio: County FairsTiffinOhio.netNo ratings yet
- EpicondilteDocument7 pagesEpicondilteRicardo fariaNo ratings yet
- Anorexia Nervosa: A Literature Review: Progress in Health Sciences December 2020Document7 pagesAnorexia Nervosa: A Literature Review: Progress in Health Sciences December 2020Rayyan TariqNo ratings yet
- En 469 Garments User Information GuideDocument4 pagesEn 469 Garments User Information GuidePricopie AlexandruNo ratings yet
- Reliability MedEl CI-3d98 PDFDocument6 pagesReliability MedEl CI-3d98 PDFneculavNo ratings yet
- Legal Medicine Notes 2020Document8 pagesLegal Medicine Notes 2020Iamharbeyy CastroNo ratings yet
- D.C. Cir. 23-05220 DCKT - 000 Filed 2024-04-15Document73 pagesD.C. Cir. 23-05220 DCKT - 000 Filed 2024-04-15charlie minatoNo ratings yet
- BiPAP Full FlowchartDocument1 pageBiPAP Full FlowchartArjun KumarNo ratings yet
- School-Based Occupational Therapy: January 2020Document33 pagesSchool-Based Occupational Therapy: January 2020purplemeraldNo ratings yet
- The French in North America Unit Chapter 2Document9 pagesThe French in North America Unit Chapter 2api-490517749No ratings yet
- Palm Beach County Student Academic Support PlanDocument29 pagesPalm Beach County Student Academic Support PlanMatt PapaycikNo ratings yet
- Hubungan Pengetahuan, Sikap, Dan Perilaku Kesehatan Gigi Dan Mulut Terhadap Status Karies Siswa SMP Negeri 1 Selogiri, WonogiriDocument4 pagesHubungan Pengetahuan, Sikap, Dan Perilaku Kesehatan Gigi Dan Mulut Terhadap Status Karies Siswa SMP Negeri 1 Selogiri, WonogiriAvina Anin NasiaNo ratings yet
- Lgu Service Delivery Baseline DataDocument1 pageLgu Service Delivery Baseline DataAahron Montoya DinauanaoNo ratings yet
- QP-005 Training ProcessDocument3 pagesQP-005 Training Processesraa asemNo ratings yet
- Đề thi TS NK Anh (chuyên) 18-19Document10 pagesĐề thi TS NK Anh (chuyên) 18-19Trung KiênNo ratings yet
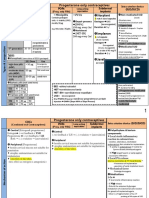
- Norplant: Progesterone Only ContraceptivesDocument9 pagesNorplant: Progesterone Only ContraceptivesFathy ElsheshtawyNo ratings yet
- 40 Radio Diagnosis P1Document6 pages40 Radio Diagnosis P1Venkata Dixit S BNo ratings yet
- Safety Data Sheet: 1. IdentificationDocument5 pagesSafety Data Sheet: 1. IdentificationOmar SaaedNo ratings yet
- You're Already: Le M Ge o M KneeDocument3 pagesYou're Already: Le M Ge o M KneeSara CoonNo ratings yet