You might also like
- The Number of Displaced Rib Fractures Is More Predictive For Complications in Chest Trauma PatientsDocument10 pagesThe Number of Displaced Rib Fractures Is More Predictive For Complications in Chest Trauma PatientsNhi NhiNo ratings yet
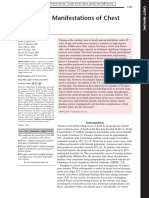
- Imaging Manifestations of Chest TraumaDocument14 pagesImaging Manifestations of Chest TraumaHana SulistiaNo ratings yet
- Acute Stroke Management in the Era of ThrombectomyFrom EverandAcute Stroke Management in the Era of ThrombectomyEdgar A. SamaniegoNo ratings yet
- Chest TraumaDocument28 pagesChest TraumaGitaAmeliaTurnipNo ratings yet
- Acetabular Fractures in Older Patients: Assessment and ManagementFrom EverandAcetabular Fractures in Older Patients: Assessment and ManagementTheodore T. MansonNo ratings yet
- Management Flail ChestDocument13 pagesManagement Flail ChestLuthfi UtamiNo ratings yet
- Clinical Handbook of Cardiac ElectrophysiologyFrom EverandClinical Handbook of Cardiac ElectrophysiologyBenedict M. GloverNo ratings yet
- 1. watcout the early killerDocument9 pages1. watcout the early killerfikryahNo ratings yet
- Metastatic Spine Disease: A Guide to Diagnosis and ManagementFrom EverandMetastatic Spine Disease: A Guide to Diagnosis and ManagementRex A. W. MarcoNo ratings yet
- Emergency Chest ImagingDocument156 pagesEmergency Chest ImagingAshutosh KafleNo ratings yet
- Thoracic Vascular TraumaDocument24 pagesThoracic Vascular TraumaKezia TambunanNo ratings yet
- Thoracic Trauma in Small AnimalsDocument5 pagesThoracic Trauma in Small AnimalsCabinet VeterinarNo ratings yet
- Minimally invasive treatment of hemothoraxDocument8 pagesMinimally invasive treatment of hemothoraxBenny KurniawanNo ratings yet
- Evaluation of The Patient With Blunt Chest Trauma - An Evidence Based ApproachDocument22 pagesEvaluation of The Patient With Blunt Chest Trauma - An Evidence Based Approachjorgeroca2009No ratings yet
- Penetrating Chest Trauma PDFDocument5 pagesPenetrating Chest Trauma PDFFerina FernandaNo ratings yet
- Chest Radiography Thoracic PolytraumaDocument14 pagesChest Radiography Thoracic PolytraumaPaola SanchezNo ratings yet
- Practice Management Guidelines For Management of Hemothorax and Occult PneumothoraxDocument9 pagesPractice Management Guidelines For Management of Hemothorax and Occult PneumothoraxPretty PuspitasariNo ratings yet
- PnemotoraksDocument4 pagesPnemotoraksGung Citra PratikaNo ratings yet
- Anesthesia For Thoracic Trauma - OpenAnesthesiaDocument7 pagesAnesthesia For Thoracic Trauma - OpenAnesthesiaReddyNo ratings yet
- HematopneumothoraxDocument13 pagesHematopneumothoraxtri_budi_20No ratings yet
- Thoracic Trauma № 7Document25 pagesThoracic Trauma № 7zerish0208No ratings yet
- EJTCM 2020 3 1 LasekDocument8 pagesEJTCM 2020 3 1 LasekRobert ChristevenNo ratings yet
- Pulmonary Trauma Emergency Department Evaluation and ManagementDocument23 pagesPulmonary Trauma Emergency Department Evaluation and ManagementPq PrissNo ratings yet
- Criem2018 4328704Document4 pagesCriem2018 4328704IthaaNo ratings yet
- Thoracic Trauma - Principals of Surgical Management: Jerzy Lasek, Eugeniusz JadczukDocument9 pagesThoracic Trauma - Principals of Surgical Management: Jerzy Lasek, Eugeniusz JadczukAnangova PradiptaNo ratings yet
- 6 Lethal DeathsDocument4 pages6 Lethal Deathslina_m354No ratings yet
- Lower Extremity Fasciotomy Indications and TechniqDocument11 pagesLower Extremity Fasciotomy Indications and TechniqbbkdabdfaNo ratings yet
- Analysis of Risk Factors in Thoracic Trauma Patients With A Comparison of A Modern Trauma Centre: A Mono-Centre StudyDocument10 pagesAnalysis of Risk Factors in Thoracic Trauma Patients With A Comparison of A Modern Trauma Centre: A Mono-Centre StudyWahyu SholekhuddinNo ratings yet
- Go To:: Respiratory ImpairmentDocument18 pagesGo To:: Respiratory ImpairmentNanik LestariNo ratings yet
- Usg PneumotoraksDocument7 pagesUsg Pneumotoraksdicky wahyudiNo ratings yet
- Pneumocephalus Mount Fuji SignDocument2 pagesPneumocephalus Mount Fuji SignSujith AyyappanNo ratings yet
- Diagnosis and Treatment of Thoracic In-Juries and Traumatic HemopneumothoraxDocument4 pagesDiagnosis and Treatment of Thoracic In-Juries and Traumatic HemopneumothoraxAnangova PradiptaNo ratings yet
- Early and Persistent Hemothorax and PneumothoraxDocument7 pagesEarly and Persistent Hemothorax and Pneumothoraxtri_budi_20No ratings yet
- Occult Pneumothorax, Revisited: Review Open AccessDocument6 pagesOccult Pneumothorax, Revisited: Review Open AccessRendy NunuhituNo ratings yet
- Thoracic Trauma Imaging TechniquesDocument37 pagesThoracic Trauma Imaging TechniquesAnwar pratama putraNo ratings yet
- PPK Bedah Luka BakarDocument7 pagesPPK Bedah Luka BakarBellaNo ratings yet
- Forensic Significance of Lesions Induced by Cardiopulmonary ResuscitationDocument6 pagesForensic Significance of Lesions Induced by Cardiopulmonary Resuscitationsukoco adi negoroNo ratings yet
- Pulmonary Contusions: AuthorsDocument13 pagesPulmonary Contusions: AuthorsRicardo HemurNo ratings yet
- TX CuelloDocument16 pagesTX CuelloStephany RodriguezNo ratings yet
- European Course Trauma CareDocument7 pagesEuropean Course Trauma CareYaclinNo ratings yet
- Flail Chest ReportDocument4 pagesFlail Chest ReportMiggsNo ratings yet
- PULMONARY CONTUSION AND FLAIL CHEST - Clinical GateDocument6 pagesPULMONARY CONTUSION AND FLAIL CHEST - Clinical GateRENATO ALONSO PACHECO ROSALESNo ratings yet
- Blunt Chest TraumaDocument14 pagesBlunt Chest TraumaAlya RahmadaniNo ratings yet
- Blunt Thoracic Trauma - Role of Chest Radiography and Comparison With CT - Fndings and Literature ReviewDocument13 pagesBlunt Thoracic Trauma - Role of Chest Radiography and Comparison With CT - Fndings and Literature Revieworalposter PIPKRA2023No ratings yet
- 31990-PB3-7415-R3Document7 pages31990-PB3-7415-R3Rolando Miranda PeñaNo ratings yet
- Interpretasi CT ScanDocument19 pagesInterpretasi CT ScanAB KristiadiNo ratings yet
- Trauma de Cuello 2007Document73 pagesTrauma de Cuello 2007Frank J. Cárdenas GándaraNo ratings yet
- Evaluation of Blunt Chest Trauma With Multidetector Computed TomographyDocument4 pagesEvaluation of Blunt Chest Trauma With Multidetector Computed TomographyasclepiuspdfsNo ratings yet
- Treatment of Hemothorax in The Era of The MinimalyDocument8 pagesTreatment of Hemothorax in The Era of The MinimalyFiska FianitaNo ratings yet
- 2019 Unusual Cavitary Lesions of The Lung Analysis ofDocument6 pages2019 Unusual Cavitary Lesions of The Lung Analysis ofLexotanyl LexiNo ratings yet
- 1229 6490 1 PB PDFDocument10 pages1229 6490 1 PB PDFSitti_HazrinaNo ratings yet
- Pneumonectomy 2Document7 pagesPneumonectomy 2jeanelineNo ratings yet
- Acute Respiratory Failure and Chest PainDocument20 pagesAcute Respiratory Failure and Chest Paink ucheNo ratings yet
- Femoral Shaft Fractures in Adults Treatment Options and ControversiesDocument11 pagesFemoral Shaft Fractures in Adults Treatment Options and ControversiesDiego BellingNo ratings yet
- Thoracic Trauma Injuries Evaluation and TreatmentDocument17 pagesThoracic Trauma Injuries Evaluation and Treatmentnageur2017No ratings yet
- Depiction Control: ECG Prognostic Significance of ECG Changes in Acute PneumoniaDocument5 pagesDepiction Control: ECG Prognostic Significance of ECG Changes in Acute PneumoniaAudrey Martin RañisesNo ratings yet
- Blunt Thoracic TraumaDocument3 pagesBlunt Thoracic TraumaNetta LionoraNo ratings yet
- 2Document17 pages2fikryahNo ratings yet
- Samrt 2Document9 pagesSamrt 2Zai RojasNo ratings yet
- Nonconvulsive Status EpilepticusDocument24 pagesNonconvulsive Status EpilepticusZai RojasNo ratings yet
- Identificacion Choque Cardiogenico ERDocument9 pagesIdentificacion Choque Cardiogenico ERZai RojasNo ratings yet
- Inotropicos ChoqueDocument11 pagesInotropicos ChoqueZai RojasNo ratings yet
- Imaging Findings of Blunt Chest TraumaDocument24 pagesImaging Findings of Blunt Chest TraumaZai RojasNo ratings yet
- A Systematic Review and Meta-Analysis of The Use of ResuscitativeDocument16 pagesA Systematic Review and Meta-Analysis of The Use of ResuscitativeZai RojasNo ratings yet
- Role of Clamping Tube Thoracostomy Prior To RemovalDocument4 pagesRole of Clamping Tube Thoracostomy Prior To RemovalZai RojasNo ratings yet
- Platz2017 PDFDocument17 pagesPlatz2017 PDFDharsheena Seshadri ManogaranNo ratings yet
- Lgu CaDocument70 pagesLgu CaMENRO GENERAL NATIVIDADNo ratings yet
- Self Love Inner Child Healing With EFTDocument11 pagesSelf Love Inner Child Healing With EFTAnonymous fUL4SPRsAf100% (1)
- S.B.D.S. College of Nursing Aherwan (Ratia) Advance Nursing Practice Lesson Plan Topic: - CommunicationDocument72 pagesS.B.D.S. College of Nursing Aherwan (Ratia) Advance Nursing Practice Lesson Plan Topic: - CommunicationAnand BhawnaNo ratings yet
- Retdem Part 2Document4 pagesRetdem Part 2gave maternityNo ratings yet
- Child Safety PresentationDocument19 pagesChild Safety Presentationalabama_medic100% (1)
- Wa0033Document10 pagesWa0033Obrian RobinsonNo ratings yet
- Boys WH Swim Results 9.14Document4 pagesBoys WH Swim Results 9.14The LedgerNo ratings yet
- Respostas Homework Wizard w6Document8 pagesRespostas Homework Wizard w6afnabiweqnksfvNo ratings yet
- Hip Pain in Pregnancy GTPS - Oct19-1Document3 pagesHip Pain in Pregnancy GTPS - Oct19-1Ryan CrossNo ratings yet
- Weight World: 1) Organic TurmericDocument6 pagesWeight World: 1) Organic TurmericGANESWAR BARIKNo ratings yet
- HDI Year 2018 Annual ReportDocument14 pagesHDI Year 2018 Annual ReportHuman Development Initiatives HdiNo ratings yet
- QUIZ 3 Disaster Readiness and Risk ReductionDocument5 pagesQUIZ 3 Disaster Readiness and Risk ReductionRain Gamboa100% (1)
- Au 31 Februari 2017Document149 pagesAu 31 Februari 2017Agnes CynthiaNo ratings yet
- Narayana HrudayalayaDocument20 pagesNarayana HrudayalayaVivek Sinha100% (1)
- Evaluation of The Mechanical PropertiesDocument237 pagesEvaluation of The Mechanical PropertiesGeorgiana IlincaNo ratings yet
- Chapter 28: Nutrition and Fluids Student Assignment: Match Each Nutrient With Its Function in The BodyDocument2 pagesChapter 28: Nutrition and Fluids Student Assignment: Match Each Nutrient With Its Function in The BodyMA. OLIVIA LINAONo ratings yet
- Girela-Lopez, Et Al (2022) Epidemiology and Autopsy Findings of 500 Drowning DeathsDocument6 pagesGirela-Lopez, Et Al (2022) Epidemiology and Autopsy Findings of 500 Drowning DeathsFilbert TandeanNo ratings yet
- 8501-00-2200 GentleMAX PRO Operators Manual RevADocument160 pages8501-00-2200 GentleMAX PRO Operators Manual RevAgamal elhanafeyNo ratings yet
- Tomczyk Dominika Resume 0812-2020Document1 pageTomczyk Dominika Resume 0812-2020api-535602662No ratings yet
- Life Saving Rules Poster in EnglishDocument11 pagesLife Saving Rules Poster in Englishkumalk3815No ratings yet
- Hema I Chapter 12 - ESRDocument30 pagesHema I Chapter 12 - ESRTesfaNo ratings yet
- NaOCL AccidentDocument2 pagesNaOCL AccidentElaf AlBoloshiNo ratings yet
- Suicide Ideation and Attempts in A Pediatric Emergency Department Before and During COVID-19Document8 pagesSuicide Ideation and Attempts in A Pediatric Emergency Department Before and During COVID-19mikoNo ratings yet
- De-Escalation in Health Care. Quick Safety. The Joint Commission, Division of Healthcare Improvement Issue 47 - January 2019Document4 pagesDe-Escalation in Health Care. Quick Safety. The Joint Commission, Division of Healthcare Improvement Issue 47 - January 2019Urgencias HorwitzNo ratings yet
- Benefits of Pet S Ownership A Review Based On Health Perspectives - 1626185594Document10 pagesBenefits of Pet S Ownership A Review Based On Health Perspectives - 1626185594ljkbbNo ratings yet
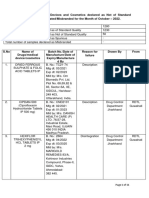
- Drug Alert List of Oct - 2022Document11 pagesDrug Alert List of Oct - 2022Gopal RaoNo ratings yet
- V. The Sexual Self. Lecture Summary (Acquire)Document7 pagesV. The Sexual Self. Lecture Summary (Acquire)Jozel ValenzuelaNo ratings yet
- References FinalDocument7 pagesReferences FinalFlourence ZafranNo ratings yet
- Unmanned Systems in Support of Future Medical Operations in Dense Urban EnvironmentsDocument28 pagesUnmanned Systems in Support of Future Medical Operations in Dense Urban EnvironmentsEdy JjNo ratings yet
- LECT 8 ColorsDocument29 pagesLECT 8 ColorsRojayneNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Recovering from Emotionally Immature Parents: Practical Tools to Establish Boundaries and Reclaim Your Emotional AutonomyFrom EverandRecovering from Emotionally Immature Parents: Practical Tools to Establish Boundaries and Reclaim Your Emotional AutonomyRating: 4.5 out of 5 stars4.5/5 (201)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)