You might also like
- Urine Examination & Analysis: Assigned By: DR - Javeria Khan Presented By: DR - Noor-ul-Ain SarwarDocument123 pagesUrine Examination & Analysis: Assigned By: DR - Javeria Khan Presented By: DR - Noor-ul-Ain SarwarErenjaeger TitanNo ratings yet
- Jaundice 160318164012Document47 pagesJaundice 160318164012Ritik MishraNo ratings yet
- JaundiceDocument47 pagesJaundiceShiv PatelNo ratings yet
- Urine ExaminationDocument8 pagesUrine ExaminationAnban SureshNo ratings yet
- Urine Analysis PresentationDocument123 pagesUrine Analysis PresentationTress Lavena100% (2)
- Jaundice: Seminar Under The Guidance Of-Dr. Shiva NarangDocument47 pagesJaundice: Seminar Under The Guidance Of-Dr. Shiva NarangMiguel MansillaNo ratings yet
- Nephrology: I. ProteinuriaDocument7 pagesNephrology: I. ProteinuriaBenjamin NgNo ratings yet
- Hepatobiliary Disorders: Katrina Saludar Jimenez, R. NDocument42 pagesHepatobiliary Disorders: Katrina Saludar Jimenez, R. NreykatNo ratings yet
- Hepatobiliary Disorders: Katrina Saludar Jimenez, R. NDocument42 pagesHepatobiliary Disorders: Katrina Saludar Jimenez, R. NKatrinaJimenezNo ratings yet
- Clinical Microscopy (Fecalysis)Document2 pagesClinical Microscopy (Fecalysis)Sheng Ramos AglugubNo ratings yet
- (HANDOUT) Phar 112 Lab - Fecalysis and Fecal Occult Blood TestDocument2 pages(HANDOUT) Phar 112 Lab - Fecalysis and Fecal Occult Blood TestHan SoloNo ratings yet
- URINALYSIS Power Point PresentationDocument20 pagesURINALYSIS Power Point PresentationOlugbenga A AdetunjiNo ratings yet
- Clinical Microscopy: Definition and Volume Disease and Cause PolyuriaDocument5 pagesClinical Microscopy: Definition and Volume Disease and Cause PolyuriaJovanni andesNo ratings yet
- UrinalysisDocument67 pagesUrinalysisumairzafar5261No ratings yet
- E M C D: Valuation and Anagement of Hronic IarrheaDocument74 pagesE M C D: Valuation and Anagement of Hronic IarrheaRevila AuliaNo ratings yet
- Summary Practical Bio (Block 4) - 3Document8 pagesSummary Practical Bio (Block 4) - 3Elsayed KowaydehNo ratings yet
- Clinical MicrosDocument20 pagesClinical MicrosKG CubilNo ratings yet
- Activity 12 UrineDocument52 pagesActivity 12 UrineNoraine Princess TabangcoraNo ratings yet
- Stool Analysis: What Is The Stool or Feces?Document28 pagesStool Analysis: What Is The Stool or Feces?Annisa SafiraNo ratings yet
- I Patient Assessment Data BaseDocument12 pagesI Patient Assessment Data BaseJanice_Fernand_1603No ratings yet
- AUBFDocument32 pagesAUBFAndrei Tumarong AngoluanNo ratings yet
- GU Blackboard OutlineDocument15 pagesGU Blackboard Outlinedlneisha61No ratings yet
- Clinical Pathology Fecalysis and UrnalysisDocument16 pagesClinical Pathology Fecalysis and UrnalysisRem Alfelor100% (3)
- Evaluation and Management of Chronic Diarrhea: Joe Harkins, PA-C Gastroenterology Center of Maine EMMC Bangor, MEDocument74 pagesEvaluation and Management of Chronic Diarrhea: Joe Harkins, PA-C Gastroenterology Center of Maine EMMC Bangor, MErehan hayderNo ratings yet
- Urinalysis and Body Fluids2020Document47 pagesUrinalysis and Body Fluids2020MONFOLA100% (1)
- Chemical TestsDocument51 pagesChemical TestsNicole Jane RobesNo ratings yet
- Urine Dipstick Testing + Common Renal Problem 2012Document52 pagesUrine Dipstick Testing + Common Renal Problem 2012Ainul ArinaNo ratings yet
- 6 BodyDocument110 pages6 Bodysinte beyuNo ratings yet
- StoolDocument28 pagesStoolThampron ThongphanNo ratings yet
- c1fd6bbd Ff7a 480d A20e C93bd3a3cedfDocument35 pagesc1fd6bbd Ff7a 480d A20e C93bd3a3cedfapi-26938624No ratings yet
- Urine AnalysisDocument63 pagesUrine AnalysisAdarshBijapurNo ratings yet
- Renal FailureDocument35 pagesRenal FailureaditNo ratings yet
- Analysis of Abnormal Urine NotesDocument6 pagesAnalysis of Abnormal Urine Notesahteshammirji575No ratings yet
- Morning Report 9/5/18: Adam Cardullo, MD Pgy - 2Document22 pagesMorning Report 9/5/18: Adam Cardullo, MD Pgy - 2Emily EresumaNo ratings yet
- Disorders of The Urogenital System2020Document58 pagesDisorders of The Urogenital System2020painx7No ratings yet
- GROUP 1 - Sweat and UrineDocument9 pagesGROUP 1 - Sweat and Urinechocoholic potchiNo ratings yet
- Darunday, Als 1Document8 pagesDarunday, Als 1Ezra Miguel DarundayNo ratings yet
- Intro To Urinalysis TransDocument5 pagesIntro To Urinalysis Transapril jholynna garroNo ratings yet
- Stool ExaminationDocument82 pagesStool Examinationambadepravin100% (2)
- Urine AnalysisDocument33 pagesUrine AnalysisajaysomNo ratings yet
- Feline Infectious Peritonitis .By SivaDocument20 pagesFeline Infectious Peritonitis .By SivaR SIVA RAMANNo ratings yet
- Paeds Crack Notes-1Document111 pagesPaeds Crack Notes-1Ashutosh Krishna JadhavNo ratings yet
- USMD, CSF, SEMEN - Professor'sDocument10 pagesUSMD, CSF, SEMEN - Professor'sMartin ClydeNo ratings yet
- Pakka Pass Pediatrics TextbookDocument112 pagesPakka Pass Pediatrics TextbookPrajwal P ShetNo ratings yet
- Jaundice and AscitesDocument15 pagesJaundice and AscitesJosiah Noella BrizNo ratings yet
- GI+hemato Past YearDocument9 pagesGI+hemato Past YearThulasi tootsieNo ratings yet
- Chemical Urinalysis TransDocument8 pagesChemical Urinalysis TransIan Carlo B GalangNo ratings yet
- Clinial MicrosDocument53 pagesClinial MicrosDreyden HaloNo ratings yet
- Urine Examination New-1Document81 pagesUrine Examination New-1H GondaliyaNo ratings yet
- Albumin: Author: Carrie A. Phelps Editor: Jörg MayerDocument1 pageAlbumin: Author: Carrie A. Phelps Editor: Jörg MayerAisyah NurlanyNo ratings yet
- Biochemistry - Urine AnalysisDocument16 pagesBiochemistry - Urine Analysisislam.o.walyNo ratings yet
- Must To Know in Clinical Microscopy UrinalysisDocument43 pagesMust To Know in Clinical Microscopy UrinalysisDaniel LamasonNo ratings yet
- Carcinomas Celulas Transicionales FinalDocument25 pagesCarcinomas Celulas Transicionales FinalLeidy CriolloNo ratings yet
- Complete Urinalysis: A. Physical Characteristics of UrineDocument8 pagesComplete Urinalysis: A. Physical Characteristics of UrineKryza Dale Bunado BaticanNo ratings yet
- Clin Path Trans 3.05 Urinalysis (2b)Document6 pagesClin Path Trans 3.05 Urinalysis (2b)Reymart FernandezNo ratings yet
- Clinical Microscopy - MTDocument200 pagesClinical Microscopy - MTJihrus MendozaNo ratings yet
- Urinalysis 2Document9 pagesUrinalysis 2Dawn GonzagaNo ratings yet
- Liver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandLiver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
- Baroreflex Failure: A Neglected Type of Secondary HypertensionDocument5 pagesBaroreflex Failure: A Neglected Type of Secondary HypertensionMichel HaddadNo ratings yet
- Accepted Manuscript: 10.1016/j.joms.2015.11.025Document20 pagesAccepted Manuscript: 10.1016/j.joms.2015.11.025FelipeNobreNo ratings yet
- Nac OsceDocument1,089 pagesNac OsceVikrantNo ratings yet
- Health Screening Questionnaire Ver 1.1 - Ooi Wei ShengDocument2 pagesHealth Screening Questionnaire Ver 1.1 - Ooi Wei ShengTerry wei shengNo ratings yet
- Chapter 4 ParasitologyDocument35 pagesChapter 4 ParasitologyJuancho OsorioNo ratings yet
- Surgical Specialty Oral Q's (Somewhat Translated)Document3 pagesSurgical Specialty Oral Q's (Somewhat Translated)dNo ratings yet
- Kanski Picture TestDocument102 pagesKanski Picture TestAnas Abuseif100% (1)
- English Assigmentt .Document12 pagesEnglish Assigmentt .Fareza AkbarNo ratings yet
- Pranic Healing For Partially Blind-A Case Study: Srikanth N Jois, Nagendra K PrasadDocument5 pagesPranic Healing For Partially Blind-A Case Study: Srikanth N Jois, Nagendra K PrasadMagdalena BozinoskaNo ratings yet
- TB - SeminarDocument12 pagesTB - SeminarLaith DmourNo ratings yet
- CSC Proforma - GeneralDocument6 pagesCSC Proforma - General127 Shruthik Patel ThotaNo ratings yet
- AcetylcysteineDocument2 pagesAcetylcysteineGwyn Rosales100% (1)
- Visual Mnemonics Medicine 2e 40 Medical Mnemonics 41 40 Oct 16 2019 41 40 1700212737 41 40 Independently Published 41Document146 pagesVisual Mnemonics Medicine 2e 40 Medical Mnemonics 41 40 Oct 16 2019 41 40 1700212737 41 40 Independently Published 41El Farouk100% (1)
- Seizure Disorders: Assessment and Diagnostic FindingsDocument3 pagesSeizure Disorders: Assessment and Diagnostic FindingsBlessed GarcianoNo ratings yet
- AnemiaDocument2 pagesAnemiaLazeh MeNo ratings yet
- SS3 Biology Lesson NoteDocument64 pagesSS3 Biology Lesson Notepalmer okiemuteNo ratings yet
- Syllabus Master Tung PDFDocument25 pagesSyllabus Master Tung PDFkamran ahmadNo ratings yet
- Sepsis and Severe Pneumonia (2022)Document39 pagesSepsis and Severe Pneumonia (2022)rina delsNo ratings yet
- Pathophysiology of Cerebral EdemaDocument10 pagesPathophysiology of Cerebral Edemarifki irsyadNo ratings yet
- Previous BON Files (Medical-Surgical Nursing)Document14 pagesPrevious BON Files (Medical-Surgical Nursing)Tom CuencaNo ratings yet
- Diabetic Gastroparesis: Pathophysiology, Evaluation and ManagementDocument10 pagesDiabetic Gastroparesis: Pathophysiology, Evaluation and ManagementboomNo ratings yet
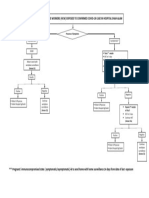
- Management of Healthcare Workers (HCW) Exposed To Confirmed Covid-19 Case in Hospital Shah AlamDocument1 pageManagement of Healthcare Workers (HCW) Exposed To Confirmed Covid-19 Case in Hospital Shah AlamNurhafizah IbrahimNo ratings yet
- 12 Physical Education English Medium Chapter PDFDocument25 pages12 Physical Education English Medium Chapter PDFANSHUL MEHROTTRANo ratings yet
- 2024.ENT - Trans03.pharmacology of ENTDocument6 pages2024.ENT - Trans03.pharmacology of ENTEADOH RO2No ratings yet
- Ebola Virus HOMEOPHATYDocument3 pagesEbola Virus HOMEOPHATYgiopscribdNo ratings yet
- Charts and Hearts PDFDocument51 pagesCharts and Hearts PDFBen ScottNo ratings yet
- Microbes and Infection: Jin-Yan Li, Zhi You, Qiong Wang, Zhi-Jian Zhou, Ye Qiu, Rui Luo, Xing-Yi GeDocument6 pagesMicrobes and Infection: Jin-Yan Li, Zhi You, Qiong Wang, Zhi-Jian Zhou, Ye Qiu, Rui Luo, Xing-Yi GeLeah StroposNo ratings yet
- Midterm PrepDocument2 pagesMidterm PrepSAKHAWAT HOSSAIN KHAN MDNo ratings yet
- Renal Disease Control/mental Health Program/community-Based Rehabilitation ProgramDocument29 pagesRenal Disease Control/mental Health Program/community-Based Rehabilitation ProgramRon Ar Ica100% (1)
- Vitamin D: Gandham. RajeevDocument66 pagesVitamin D: Gandham. Rajeevguna sundariNo ratings yet