You might also like
- Liver - Dr. Allam 2021 PDFDocument70 pagesLiver - Dr. Allam 2021 PDFMohammedNo ratings yet
- Differential Diagnosis of JaundiceDocument4 pagesDifferential Diagnosis of JaundiceVirag PatilNo ratings yet
- Understanding JaundiceDocument47 pagesUnderstanding JaundiceShiv PatelNo ratings yet
- Jaundice: Seminar Under The Guidance Of-Dr. Shiva NarangDocument47 pagesJaundice: Seminar Under The Guidance Of-Dr. Shiva NarangMiguel MansillaNo ratings yet
- What? Who?: DR - Mabel Sihombing Sppd-Kgeh DR - Ilhamd SPPD Dpertemen Ilmu Penyakit Dalam Rs - Ham/Fk-Usu MedanDocument45 pagesWhat? Who?: DR - Mabel Sihombing Sppd-Kgeh DR - Ilhamd SPPD Dpertemen Ilmu Penyakit Dalam Rs - Ham/Fk-Usu MedanM Rizky Assilmy LubisNo ratings yet
- Jaundice: DR Monika PathaniaDocument27 pagesJaundice: DR Monika PathaniaMuhammed al-jumailyNo ratings yet
- Approach To A Patient With JaundiceDocument33 pagesApproach To A Patient With JaundiceRahul Kumar VermaNo ratings yet
- Liver FunctionDocument90 pagesLiver Functionapi-19641337No ratings yet
- Liver Function TesDocument58 pagesLiver Function TesnoffrizalNo ratings yet
- JAUNDICE Internal Medicine PresentationDocument34 pagesJAUNDICE Internal Medicine PresentationShitanjni WatiNo ratings yet
- Major Manifestations of Hepatobiliary Diseases. JaundiceDocument11 pagesMajor Manifestations of Hepatobiliary Diseases. Jaundicehussain AltaherNo ratings yet
- Jaundice and Ascites Group ProjectDocument15 pagesJaundice and Ascites Group ProjectJosiah Noella BrizNo ratings yet
- Interpretation of LFT: A Guide to Working Up Abnormal Liver TestsDocument35 pagesInterpretation of LFT: A Guide to Working Up Abnormal Liver TestsElaineNo ratings yet
- 5 - JaundiceDocument16 pages5 - JaundiceHamzehNo ratings yet
- Pathophysiology of Laboratory Abnormalities in Liver DisordersDocument55 pagesPathophysiology of Laboratory Abnormalities in Liver DisordersYudha fedrian AKNo ratings yet
- Approach to Patients with Jaundice - Causes, Evaluation & ManagementDocument76 pagesApproach to Patients with Jaundice - Causes, Evaluation & ManagementSuresh Kubavat100% (3)
- Liver Function TestsDocument70 pagesLiver Function TestsG Venkatesh100% (5)
- GIT Cirrhosis Liver in ChildrenDocument37 pagesGIT Cirrhosis Liver in ChildrenDr.P.NatarajanNo ratings yet
- Clin PathInterns Review 2019Document33 pagesClin PathInterns Review 2019AmaetenNo ratings yet
- Liver Function Tests and How To Relate ThemDocument82 pagesLiver Function Tests and How To Relate ThemG VenkateshNo ratings yet
- Liver Function Tests: Presented By-Dr. Arshiya Kaura (JR 1)Document50 pagesLiver Function Tests: Presented By-Dr. Arshiya Kaura (JR 1)vikasNo ratings yet
- Organ Function Test: Assessment of Functions of The OrgansDocument39 pagesOrgan Function Test: Assessment of Functions of The OrgansSri Abinash MishraNo ratings yet
- JAUNDICE Internal Medicine PresentationDocument34 pagesJAUNDICE Internal Medicine PresentationNano BaddourNo ratings yet
- Hyperbilirubinemia: West Visayas State University College of Medicine Neonatal Intensive Care UnitDocument49 pagesHyperbilirubinemia: West Visayas State University College of Medicine Neonatal Intensive Care UnitDonna LabaniegoNo ratings yet
- HyperbilirubinimiaDocument7 pagesHyperbilirubinimiavonyrNo ratings yet
- Approach To Jaundice (1) .PPT ALAWAJIDocument28 pagesApproach To Jaundice (1) .PPT ALAWAJIayuNo ratings yet
- Liver Function TestsDocument35 pagesLiver Function TestsMaham RehmanNo ratings yet
- Liver Function TestsDocument48 pagesLiver Function TestsAli H. Sadiek أ.د. علي حسن صديق100% (12)
- Slides DR Ashgar Approach To LFTs 12.12.2021Document47 pagesSlides DR Ashgar Approach To LFTs 12.12.2021Maryam OmarNo ratings yet
- Bilirubin Levels and JaundiceDocument34 pagesBilirubin Levels and JaundiceKmo mastnNo ratings yet
- Liver DiseasesDocument24 pagesLiver DiseasesAbdo HaiderNo ratings yet
- Labdxtransfinals PDFDocument16 pagesLabdxtransfinals PDFSubhan Souda MangalasseryNo ratings yet
- What Are The Salient Features of The Patient? (10pts)Document7 pagesWhat Are The Salient Features of The Patient? (10pts)Aubrey Unique EvangelistaNo ratings yet
- Jaundice 1Document26 pagesJaundice 1priyanshisenjaliya095No ratings yet
- Urine Dipstick Testing + Common Renal Problem 2012Document52 pagesUrine Dipstick Testing + Common Renal Problem 2012Ainul ArinaNo ratings yet
- Approach To Neonatal JaundiceDocument73 pagesApproach To Neonatal JaundiceG Venkatesh50% (2)
- Chole Stasis GR 1Document13 pagesChole Stasis GR 1Matet MonjeNo ratings yet
- Obstructive Jaundice Group 6Document33 pagesObstructive Jaundice Group 6Qurbon AliNo ratings yet
- Final Neonatal JaundiceDocument47 pagesFinal Neonatal JaundiceArati JhaNo ratings yet
- GI Problems: Guide to Hepatomegaly, Jaundice, and HepatitisDocument86 pagesGI Problems: Guide to Hepatomegaly, Jaundice, and HepatitisThitanun TungchutworakulNo ratings yet
- Liver Function Tests ExplainedDocument20 pagesLiver Function Tests ExplainedSasi KumarNo ratings yet
- 97Document79 pages97HATLERNo ratings yet
- 4-Hepatobiliary DiseaseDocument22 pages4-Hepatobiliary Diseaseabdalmajeed alshammaryNo ratings yet
- Case of Obstructive JaundiceDocument38 pagesCase of Obstructive JaundiceadiNo ratings yet
- Liver DiagnosticsDocument10 pagesLiver DiagnosticsTiny Briones-SallomanNo ratings yet
- Morning Report 9/5/18: Adam Cardullo, MD Pgy - 2Document22 pagesMorning Report 9/5/18: Adam Cardullo, MD Pgy - 2Emily EresumaNo ratings yet
- What is Jaundice? Causes, Types and DiagnosisDocument29 pagesWhat is Jaundice? Causes, Types and DiagnosisARUSHI ARVINDNo ratings yet
- JaundiceDocument6 pagesJaundiceNiaNo ratings yet
- Jaundice - StatPearls - NCBI BookshelfDocument11 pagesJaundice - StatPearls - NCBI BookshelfCONSTANTIUS AUGUSTONo ratings yet
- T15 - Neonatal JaundiceDocument38 pagesT15 - Neonatal JaundiceMawuliNo ratings yet
- Dr. Ali Abdul Hussein's Guide to Jaundice Causes and EvaluationDocument24 pagesDr. Ali Abdul Hussein's Guide to Jaundice Causes and EvaluationPatrico Rillah SetiawanNo ratings yet
- CLD FinalDocument17 pagesCLD FinalHervis FantiniNo ratings yet
- Pemeriksaan Fungsi Hati .: Prof. Dr. Adi Koesoema Aman SPPK (KH)Document51 pagesPemeriksaan Fungsi Hati .: Prof. Dr. Adi Koesoema Aman SPPK (KH)kiki rawitriNo ratings yet
- Liver FunctionDocument24 pagesLiver FunctionramireddyNo ratings yet
- Jaundice: Presented by Dr. Pollock Prepared by Christopher Edwards Tintanalli Chapter 84, Pgs. 560-561 October 2005Document16 pagesJaundice: Presented by Dr. Pollock Prepared by Christopher Edwards Tintanalli Chapter 84, Pgs. 560-561 October 2005wiranirwanaNo ratings yet
- Approach To JaundiceDocument36 pagesApproach To JaundiceNandita ChatterjeeNo ratings yet
- 3.1 Jaundice LsyDocument25 pages3.1 Jaundice Lsymirabel IvanaliNo ratings yet
- Essential Liver Function Test GuideDocument19 pagesEssential Liver Function Test GuidevikasNo ratings yet
- Jaundice: - Yellowish Discolouration ofDocument26 pagesJaundice: - Yellowish Discolouration ofVeimern ChinNo ratings yet
- Liver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandLiver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
- 可汗语法48篇(明志教育推荐) PDFDocument163 pages可汗语法48篇(明志教育推荐) PDFtellmewhour100% (2)
- MEM Micro-ProjectDocument16 pagesMEM Micro-ProjectGanesh GoreNo ratings yet
- Anatomy of The PeriodontiumDocument46 pagesAnatomy of The PeriodontiumYunita Nitnot50% (2)
- Fault Tracing: FMI 3: Checking The Sensor CircuitDocument1 pageFault Tracing: FMI 3: Checking The Sensor Circuituser1No ratings yet
- Sibling RivalryDocument2 pagesSibling Rivalrycarlokim14No ratings yet
- 2018 Federal Income Tax Return PDFDocument8 pages2018 Federal Income Tax Return PDFBrandon BachNo ratings yet
- Altivar 71 - ATV71H037M3Document13 pagesAltivar 71 - ATV71H037M3Mite TodorovNo ratings yet
- Principle of Economics Consolidated Assignements-2 - 10th February 22Document27 pagesPrinciple of Economics Consolidated Assignements-2 - 10th February 22Mani Bhushan SinghNo ratings yet
- Cultures and Beliefs NCM 120Document13 pagesCultures and Beliefs NCM 120Melanie AnanayoNo ratings yet
- Thermogravimetric Analysis - TGA: Analyzing & TestingDocument20 pagesThermogravimetric Analysis - TGA: Analyzing & TestingRusitaDessyNo ratings yet
- Veena Singh-176-189 - Findings, Implications and ConclusionsDocument14 pagesVeena Singh-176-189 - Findings, Implications and ConclusionsValerine SNo ratings yet
- Shortened Dental Arch ConceptDocument3 pagesShortened Dental Arch ConceptVivek ShankarNo ratings yet
- Flatworms Round Worms and Anne Lids LabDocument6 pagesFlatworms Round Worms and Anne Lids LabBellaNo ratings yet
- By Pass System in The Dry ProcessDocument34 pagesBy Pass System in The Dry Processfaheemqc100% (1)
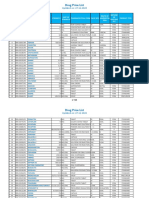
- PPR - LISTS - Registered Medicine Price List - 20221127 BahrainDocument318 pagesPPR - LISTS - Registered Medicine Price List - 20221127 BahrainvdvedNo ratings yet
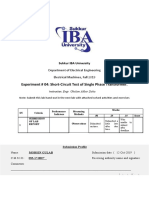
- Experiment # 04: Short-Circuit Test of Single Phase TransformerDocument5 pagesExperiment # 04: Short-Circuit Test of Single Phase TransformerNasir Ali / Lab Engineer, Electrical Engineering DepartmentNo ratings yet
- Practical-2 Simulation of ReactorsDocument2 pagesPractical-2 Simulation of ReactorsniralNo ratings yet
- MaryamDocument1 pageMaryamHAIZA FATHIMANo ratings yet
- Manual de Reparacion TXV75Document16 pagesManual de Reparacion TXV75Ovh MaquinariasNo ratings yet
- Microwave TubesDocument36 pagesMicrowave TubesHINDUSTAN KNOW 1No ratings yet
- Demand, Supply, and Market Equilibrium: Mcgraw-Hill/IrwinDocument34 pagesDemand, Supply, and Market Equilibrium: Mcgraw-Hill/IrwinLillian KobusingyeNo ratings yet
- Physical Properties of Groups 1, 17 and 18 ElementsDocument5 pagesPhysical Properties of Groups 1, 17 and 18 ElementslenovosubaNo ratings yet
- Exercise 5 - Journalizing TransactionsDocument10 pagesExercise 5 - Journalizing TransactionsMichael DiputadoNo ratings yet
- Syllabus of Modules FOR THE Electrician Domestic (ELE701)Document6 pagesSyllabus of Modules FOR THE Electrician Domestic (ELE701)udi969100% (1)
- Audi A6 Allroad Model 2013 Brochure - 2012.08Document58 pagesAudi A6 Allroad Model 2013 Brochure - 2012.08Arkadiusz KNo ratings yet
- Indian School Sohar Term II Examination 2018-19 EnglishDocument4 pagesIndian School Sohar Term II Examination 2018-19 EnglishRitaNo ratings yet
- Physical ExaminationDocument7 pagesPhysical ExaminationCha CulveraNo ratings yet
- Heavy Oil's Production ProblemsDocument22 pagesHeavy Oil's Production Problemsalfredo moran100% (1)
- PN Junction Formation and Barrier PotentialDocument9 pagesPN Junction Formation and Barrier PotentialchristlllNo ratings yet
- Klubermatic Lubricant DispensersDocument13 pagesKlubermatic Lubricant Dispenserstatankise100% (1)