You might also like
- Reversible and Irreversible Cell InjuryDocument55 pagesReversible and Irreversible Cell Injurygabb bbNo ratings yet
- 6 B&B CirrhosisDocument30 pages6 B&B CirrhosisSara Joseph100% (1)
- CH10Document17 pagesCH10Kim BasicNo ratings yet
- Respiratory Osce: AMSA Edinburgh X IMU Y4Document34 pagesRespiratory Osce: AMSA Edinburgh X IMU Y4Abby LiewNo ratings yet
- GI + Renal OSCE: AMSA Edinburgh X IMU Y4Document41 pagesGI + Renal OSCE: AMSA Edinburgh X IMU Y4Abby LiewNo ratings yet
- Structural Biology of HIVDocument31 pagesStructural Biology of HIVLaura TapiaNo ratings yet
- Anastomosis Left Anterior Cerebral Artery BlockageDocument5 pagesAnastomosis Left Anterior Cerebral Artery BlockagemcwnotesNo ratings yet
- Pathoma 2087m (34h47) : 1) Growth Adaptations, Cell Injury 154 MinsDocument11 pagesPathoma 2087m (34h47) : 1) Growth Adaptations, Cell Injury 154 Minsgreen mateNo ratings yet
- Brainstem NucleiDocument9 pagesBrainstem Nucleiankur_1No ratings yet
- Chapter 3 Genetic VariationDocument21 pagesChapter 3 Genetic VariationAbdulkarimNo ratings yet
- Brainstem StrokesDocument4 pagesBrainstem StrokesChandniNo ratings yet
- CerebellumDocument14 pagesCerebellumapi-508474347No ratings yet
- Cerebral Blood FlowDocument39 pagesCerebral Blood FlowRajat ThakurNo ratings yet
- Schematic Diagram Wilson'S DiseaseDocument2 pagesSchematic Diagram Wilson'S DiseaseAmira CharmaineNo ratings yet
- Cardio Block 3Document62 pagesCardio Block 3Maya LaPradeNo ratings yet
- Nose & Paranasal Sinuses 2018Document63 pagesNose & Paranasal Sinuses 2018yasrul izadNo ratings yet
- Psy101: Psychiatric Foundations and Psychological Reaction To DisabilityDocument30 pagesPsy101: Psychiatric Foundations and Psychological Reaction To DisabilityAlexia Ofel DinsonNo ratings yet
- Cytogenetics Course PackDocument29 pagesCytogenetics Course Packanonymous squashNo ratings yet
- Acute Tubular NecrosisDocument60 pagesAcute Tubular NecrosisYedesney C. LinaresNo ratings yet
- Edema Pathology by Asif AliDocument21 pagesEdema Pathology by Asif AliHassan AsifNo ratings yet
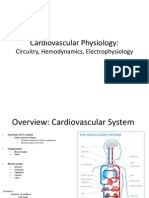
- Cardiovascular Physiology:: Circuitry, Hemodynamics, ElectrophysiologyDocument27 pagesCardiovascular Physiology:: Circuitry, Hemodynamics, Electrophysiologyrsmoney3No ratings yet
- Iron Metabolism: DR Mukhtiar BaigDocument58 pagesIron Metabolism: DR Mukhtiar BaigdrmukhtiarbaigNo ratings yet
- Nerve StructureDocument53 pagesNerve StructureMedulla Oblongata100% (1)
- Beri Beri: Water-Soluble Vitamins ThiamineDocument3 pagesBeri Beri: Water-Soluble Vitamins ThiamineLyan SamsonNo ratings yet
- CerebellumDocument22 pagesCerebellumSalman XahirNo ratings yet
- Chapter 2 - Nervous System NHR 2021Document70 pagesChapter 2 - Nervous System NHR 2021Yusman Hakim100% (1)
- Hema Lec Prefinals ExamDocument18 pagesHema Lec Prefinals ExamMark jay LlanoNo ratings yet
- Regulation of RespirationDocument48 pagesRegulation of Respirationabdullah amirNo ratings yet
- Upperlimb-Clinical CasesDocument18 pagesUpperlimb-Clinical CasesKambwe ChristopherNo ratings yet
- Cranial Nerves and BranchesDocument5 pagesCranial Nerves and Branchesballer0417No ratings yet
- Neuro Written III TablesDocument5 pagesNeuro Written III TablesSolomon Seth SallforsNo ratings yet
- Renal Function and The Significance of Non-Protein Nitrogen CompoundsDocument12 pagesRenal Function and The Significance of Non-Protein Nitrogen CompoundsSrujana BudheNo ratings yet
- Embryo NotesDocument52 pagesEmbryo NotesSharona Avgush100% (1)
- Heart FailureDocument35 pagesHeart FailureSanjeev Harry BudhooramNo ratings yet
- Diseases of Blood Vessels Dr. Fe A. Bartolome, Maed, FpasmapDocument15 pagesDiseases of Blood Vessels Dr. Fe A. Bartolome, Maed, FpasmapJayesh MahajanNo ratings yet
- Haematology-Summary My NotesDocument24 pagesHaematology-Summary My NotesToria053No ratings yet
- ImmunopathologyDocument21 pagesImmunopathologyapplesncoreNo ratings yet
- Virology NotesDocument81 pagesVirology NotesraulNo ratings yet
- Examination of The HipDocument33 pagesExamination of The HipTumbal BroNo ratings yet
- Pericardial EffusionDocument1 pagePericardial EffusionAlfrin Antony100% (1)
- Triage FormDocument2 pagesTriage FormCael LayugNo ratings yet
- Purine Metabolism de Novo Synthesis and Salvage Pathway, 2015Document28 pagesPurine Metabolism de Novo Synthesis and Salvage Pathway, 2015Tehreem NadeemNo ratings yet
- RT 105 Finals NotesDocument24 pagesRT 105 Finals NotesLouiseNo ratings yet
- Shanz - Pedia 1.03Document16 pagesShanz - Pedia 1.03Petrina XuNo ratings yet
- Benign WBC Disorders Third YaerDocument27 pagesBenign WBC Disorders Third YaerAisho KeyfNo ratings yet
- PleuraDocument6 pagesPleuraameerabest100% (1)
- Gametogenesis, Gamete Transport & FertilizationDocument56 pagesGametogenesis, Gamete Transport & FertilizationvictorNo ratings yet
- Histology of Kidney, Ureter and Urinary BladderDocument28 pagesHistology of Kidney, Ureter and Urinary Bladderkhairul_azhar_27No ratings yet
- Carbohydrate MetabolismDocument53 pagesCarbohydrate Metabolismjehram navalesNo ratings yet
- Pharmacology 1 Unit 5 Psycho Pharma Cological Agents Notes by MahendraDocument39 pagesPharmacology 1 Unit 5 Psycho Pharma Cological Agents Notes by MahendraKim Nicole Villaflores0% (1)
- Patho FEU PGI BCA Exit Exam May 2020Document34 pagesPatho FEU PGI BCA Exit Exam May 2020Sheryl Layne LaoNo ratings yet
- Revalida Review NotesDocument14 pagesRevalida Review NotesBryan Lloyd RayatNo ratings yet
- Thiamine Pyrophosphate (TTP) Thiamine Pyrophosphate (TTP)Document4 pagesThiamine Pyrophosphate (TTP) Thiamine Pyrophosphate (TTP)Lyan SamsonNo ratings yet
- Adrenal & KortisolDocument47 pagesAdrenal & KortisolPrisca AngelinaNo ratings yet
- Neisse RiaDocument49 pagesNeisse RiaSubhada GosaviNo ratings yet
- Oxfordmed CNS Examination-1Document13 pagesOxfordmed CNS Examination-1lailatul husna100% (1)
- ALaboratory Reportonthe Observed Parasitesinthe Gillsand Gutof Anabastestudineus Puyofrom Kabacan Cotabato PhilippinesDocument15 pagesALaboratory Reportonthe Observed Parasitesinthe Gillsand Gutof Anabastestudineus Puyofrom Kabacan Cotabato PhilippinesNicollo DadiavelliNo ratings yet
- Anatomy GI TractDocument54 pagesAnatomy GI TractSaran DNo ratings yet
- Cirrhosis 22008 Bajar Musica Gratis Descargar Musica Gratis Online Descargar Musica Gratis para CelularesDocument72 pagesCirrhosis 22008 Bajar Musica Gratis Descargar Musica Gratis Online Descargar Musica Gratis para CelularesYeni Chie Aneuk TuleutNo ratings yet
- With Ordinary Talent and Extraordinary Perseverance, All Things Are Attainable.Document72 pagesWith Ordinary Talent and Extraordinary Perseverance, All Things Are Attainable.Ainun JaariahNo ratings yet
- PericarditisDocument28 pagesPericarditisHATLERNo ratings yet
- DesmurgyDocument18 pagesDesmurgyHATLERNo ratings yet
- Chap 19 - The Reproductive SystemDocument46 pagesChap 19 - The Reproductive SystemHATLERNo ratings yet
- Chap 18 - The Urinary SystemDocument22 pagesChap 18 - The Urinary SystemHATLERNo ratings yet
- Exam 2 Reading Passage 2 - Sleep Should Be Prescribed What Those Late Nights Out Could Be Costing YouDocument1 pageExam 2 Reading Passage 2 - Sleep Should Be Prescribed What Those Late Nights Out Could Be Costing YouPhương Nguyễn0% (1)
- Hypnosymbolic PsychotherapyDocument8 pagesHypnosymbolic PsychotherapyZoita Mandila100% (1)
- Seerat Kaur - FEMALE - 22 Yrs +918968148007 APJ1.0020209332 5801854Document2 pagesSeerat Kaur - FEMALE - 22 Yrs +918968148007 APJ1.0020209332 5801854Seerat KaurNo ratings yet
- An Integrated Approach To Fetal Growth RestrictionDocument11 pagesAn Integrated Approach To Fetal Growth RestrictionalexandraNo ratings yet
- Indigenous Therapies - Sleep and WorkDocument13 pagesIndigenous Therapies - Sleep and WorkRaabiyaNo ratings yet
- Apnea in The NewbornDocument20 pagesApnea in The NewbornJisha Annie JohnNo ratings yet
- Children and Young People With Cancer:: A Parent's GuideDocument37 pagesChildren and Young People With Cancer:: A Parent's GuideCatarina CostaNo ratings yet
- Trends and Issues in Nursing EducationDocument3 pagesTrends and Issues in Nursing EducationAlona Beth PacañaNo ratings yet
- Cosmetic Gynecology Booklet - Dr. Michael Tahery in Los AngelesDocument16 pagesCosmetic Gynecology Booklet - Dr. Michael Tahery in Los AngelesMichael TaheryNo ratings yet
- Clinical Topic # 5: Gastric Tubes Student GuideDocument3 pagesClinical Topic # 5: Gastric Tubes Student Guidetripj33No ratings yet
- Aneurysm: Symptoms of An AneurysmDocument3 pagesAneurysm: Symptoms of An AneurysmArun MuralidharanNo ratings yet
- JOGCan 2018 Fetal Surveillance B IntrapartumDocument25 pagesJOGCan 2018 Fetal Surveillance B IntrapartumMiguel Guillermo Salazar ClavijoNo ratings yet
- Group 5 Benz Research Project Final Output 1Document61 pagesGroup 5 Benz Research Project Final Output 1Christine Mae BacomoNo ratings yet
- Resume of Neil J. GajjarDocument6 pagesResume of Neil J. GajjarNeil J. GajjarNo ratings yet
- OB Doctors Orders (Answer Key)Document3 pagesOB Doctors Orders (Answer Key)Ryan-Jay AbolenciaNo ratings yet
- CHN Post TestDocument13 pagesCHN Post TestAngel YN Patricio FlorentinoNo ratings yet
- 2016 Physical Fitness TestDocument13 pages2016 Physical Fitness TestDafchen Nio MahasolNo ratings yet
- Risk Assessment Method Statement Storage Tank PDFDocument6 pagesRisk Assessment Method Statement Storage Tank PDFNiyi Folayan100% (1)
- Infective EndocarditiDocument31 pagesInfective EndocarditiMansi DabolaNo ratings yet
- Improving The Physical Health of People With Mental Health ProblemsDocument61 pagesImproving The Physical Health of People With Mental Health ProblemsThierry UhawenimanaNo ratings yet
- Bs Aslym Seeker HealthDocument8 pagesBs Aslym Seeker HealthDeepak aggarwalNo ratings yet
- Evaluation of The Adult With Dyspnea in The Emergency DepartmentDocument16 pagesEvaluation of The Adult With Dyspnea in The Emergency DepartmentmericenteNo ratings yet
- KHADIJAHDocument35 pagesKHADIJAHshintya sebayangNo ratings yet
- Pancreatitis Case FileDocument2 pagesPancreatitis Case Filehttps://medical-phd.blogspot.comNo ratings yet
- Fungal Infection Knowledge Gap in Ethiopia: Brief CommunicationDocument3 pagesFungal Infection Knowledge Gap in Ethiopia: Brief Communicationrozina mulatNo ratings yet
- PortfolioresumeDocument1 pagePortfolioresumeapi-653800047No ratings yet
- German S3 Guidelines: Anal Abscess and Fistula (Second Revised Version)Document55 pagesGerman S3 Guidelines: Anal Abscess and Fistula (Second Revised Version)Bunga AmiliaNo ratings yet
- Preventing Relapse of Mental Illnesses: Tips ForDocument12 pagesPreventing Relapse of Mental Illnesses: Tips ForUsman Ahmad TijjaniNo ratings yet
- Content ServerDocument13 pagesContent ServerWilber Will Huillca Santa CruzNo ratings yet
- Rotary Club Varanasi EastDocument22 pagesRotary Club Varanasi Eastanish_10677953No ratings yet