You might also like
- Arthritis and Society: The Impact of Musculoskeletal DiseasesFrom EverandArthritis and Society: The Impact of Musculoskeletal DiseasesNo ratings yet
- Association Between Low Back Pain and Various Everyday PerformancesDocument9 pagesAssociation Between Low Back Pain and Various Everyday Performancesshaik chandiniNo ratings yet
- Sample Chapter OneDocument7 pagesSample Chapter Oneaminuandanimutala112No ratings yet
- Chapter 1-IV PDFDocument76 pagesChapter 1-IV PDFJohn Gabriel SamsonNo ratings yet
- Low Back Pain (Non-Specific)Document15 pagesLow Back Pain (Non-Specific)PilatesCientfico100% (1)
- Nonespecific Low BackpainDocument8 pagesNonespecific Low BackpainleocmyNo ratings yet
- Title: Depression, Pain and Physical Function in Patients With Osteoarthritis of The KneeDocument16 pagesTitle: Depression, Pain and Physical Function in Patients With Osteoarthritis of The Kneemohamad safiiNo ratings yet
- Newest Olokode'S - Project FinalDocument59 pagesNewest Olokode'S - Project FinalOlokode OlawunmiNo ratings yet
- Ao 2Document10 pagesAo 2Ayu SuprabawatiNo ratings yet
- Fox - Treatment of Knee Osteoarthritis - ER 2010 2 PDFDocument11 pagesFox - Treatment of Knee Osteoarthritis - ER 2010 2 PDFdrksk355No ratings yet
- EJHC Volume 13 Issue 3 Pages 2100-2118Document19 pagesEJHC Volume 13 Issue 3 Pages 2100-2118احمد العايديNo ratings yet
- DR Faisal Hayat FinalDocument11 pagesDR Faisal Hayat FinalbabuhaiderkhanNo ratings yet
- Low - Back - Pain 4Document6 pagesLow - Back - Pain 4Along bangNo ratings yet
- Predictors of Health-Related Quality of Life in Patients With Non-Specific Low Back PainDocument8 pagesPredictors of Health-Related Quality of Life in Patients With Non-Specific Low Back PainAnjaswati Farida AdyanaNo ratings yet
- Terapi Farmakologi Dan Non Farmakologi Terhadap Penanganan Nyeri Osteoarthritis Pada LansiaDocument8 pagesTerapi Farmakologi Dan Non Farmakologi Terhadap Penanganan Nyeri Osteoarthritis Pada LansiaNurul Zakiah BurhanNo ratings yet
- Spinal Manipulation and Exercise For Low Back Pain in Adolescents: Study Protocol For A Randomized Controlled TrialDocument9 pagesSpinal Manipulation and Exercise For Low Back Pain in Adolescents: Study Protocol For A Randomized Controlled TrialMizan PaishalNo ratings yet
- Osteoarthritis Is A Serious DiseaseDocument4 pagesOsteoarthritis Is A Serious DiseaseSCRIBDNo ratings yet
- Hoogeboom 2012Document4 pagesHoogeboom 2012Ika KemalaNo ratings yet
- The Importance of Gender in Health ProblemsDocument6 pagesThe Importance of Gender in Health Problemsmohdisram26No ratings yet
- Jurnal Low Back PainDocument14 pagesJurnal Low Back PainHerdiana SsfcNo ratings yet
- VC1-G5-GROUP-MANUSCRIPTDocument62 pagesVC1-G5-GROUP-MANUSCRIPTljmikeefpenaNo ratings yet
- BiotekDocument12 pagesBiotekyenny handayani sihiteNo ratings yet
- 1-s2.0-S1521694210000884-Main - Epidemiology - Low Back Pain - Hoy Et Al - 2010Document13 pages1-s2.0-S1521694210000884-Main - Epidemiology - Low Back Pain - Hoy Et Al - 2010kaoxsk8No ratings yet
- Low Back Pain, 2O12Document361 pagesLow Back Pain, 2O12Bán Kata100% (4)
- Frailty SyndromeDocument2 pagesFrailty SyndromeMariaVatsolakiNo ratings yet
- Spine: Low Back and Neck PainDocument36 pagesSpine: Low Back and Neck PainhaNumzNo ratings yet
- Risk Factors Forchronic Low Back Pain 2161 0711.1000271Document4 pagesRisk Factors Forchronic Low Back Pain 2161 0711.100027155664411No ratings yet
- Faktor ResikoDocument7 pagesFaktor ResikoAnonymous hF9HwHVuqNo ratings yet
- Pereira 2015Document9 pagesPereira 2015Amalia RosaNo ratings yet
- Hsci 451 TermpaperDocument9 pagesHsci 451 Termpaperapi-241136824No ratings yet
- Outcome of DeseaseDocument8 pagesOutcome of DeseasePranjali ThakurNo ratings yet
- The Epidemiology of Low Back Pain: Best Practice & Research. Clinical Rheumatology December 2010Document14 pagesThe Epidemiology of Low Back Pain: Best Practice & Research. Clinical Rheumatology December 2010Eia RodriguezNo ratings yet
- Review of Related Literature: 2.1 Musculoskeletal ConditionsDocument21 pagesReview of Related Literature: 2.1 Musculoskeletal ConditionsJohn Gabriel SamsonNo ratings yet
- Theburdenofosteoarthritis Inolderadults: Gillian A. Hawker,, Lauren K. KingDocument12 pagesTheburdenofosteoarthritis Inolderadults: Gillian A. Hawker,, Lauren K. KingabdulfatahalhemeryNo ratings yet
- Quality of Life Patients With Ulcus DiabeticDocument4 pagesQuality of Life Patients With Ulcus DiabeticNadiaRashyaNo ratings yet
- Impact of Heart Failure On Patients Nursing EssayDocument5 pagesImpact of Heart Failure On Patients Nursing EssaySarah MasrurohNo ratings yet
- Low Back Pain in The Aging AthleteDocument12 pagesLow Back Pain in The Aging AthleteSergio Francisco Martínez Huenchullán100% (1)
- Health and Economic Costs of Physical InactivityDocument5 pagesHealth and Economic Costs of Physical InactivityLeclerc Maturana Philippe AndreNo ratings yet
- Review of Related Literature: 2.1 Musculoskeletal ConditionsDocument20 pagesReview of Related Literature: 2.1 Musculoskeletal ConditionsJohn Gabriel SamsonNo ratings yet
- Health Related Quality of Life, Depression and Anxiety Among People With Type 2 Diabetes Mellitus in BangladeshDocument26 pagesHealth Related Quality of Life, Depression and Anxiety Among People With Type 2 Diabetes Mellitus in BangladeshGhanva KhanNo ratings yet
- Relationship of Chronic LBP (Low Back Pain) With Hamstring Tightness in ProfessionalsDocument5 pagesRelationship of Chronic LBP (Low Back Pain) With Hamstring Tightness in ProfessionalsRizwan khanNo ratings yet
- Postural Imbalance in The Elderly: Main Aspects: Natália Moya Rodrigues Pereira and Marcos Eduardo ScheicherDocument19 pagesPostural Imbalance in The Elderly: Main Aspects: Natália Moya Rodrigues Pereira and Marcos Eduardo ScheicherIrvin MarcelNo ratings yet
- Movement Detection Impaired in Patients With Knee Osteoarthritis Compared To Healthy Controls: A Cross-Sectional Case-Control StudyDocument10 pagesMovement Detection Impaired in Patients With Knee Osteoarthritis Compared To Healthy Controls: A Cross-Sectional Case-Control StudyDavid SugiartoNo ratings yet
- Ijerph 14030240Document17 pagesIjerph 14030240Miss LeslieNo ratings yet
- Asociación Entre Dolor Crónico y Fragilidad Física en Adultos Mayores Que Viven en La ComunidadDocument9 pagesAsociación Entre Dolor Crónico y Fragilidad Física en Adultos Mayores Que Viven en La ComunidadmartinNo ratings yet
- Osteoarthritis MedicalDocument9 pagesOsteoarthritis Medicaldhimas satriaNo ratings yet
- Disability and DMDocument15 pagesDisability and DMCelia RodriguezNo ratings yet
- Mia Pruefer - Health Literacy and Elhers-Danlos Syndrome Hypermobility TypeDocument14 pagesMia Pruefer - Health Literacy and Elhers-Danlos Syndrome Hypermobility TypeMia PrueferNo ratings yet
- Quality of Life in Glaucoma: A Review of The LiteratureDocument23 pagesQuality of Life in Glaucoma: A Review of The LiteratureMakhda Nurfatmala LNo ratings yet
- Living Alone (Depression)Document10 pagesLiving Alone (Depression)Lidwina DewiNo ratings yet
- 1-Disease MechanismsDocument5 pages1-Disease MechanismsMarian Dane PunzalanNo ratings yet
- Research ArticleDocument11 pagesResearch ArticleMocanu ElenaNo ratings yet
- Family Medicine & Medical Science ResearchDocument9 pagesFamily Medicine & Medical Science ResearchAndhika DNo ratings yet
- Effects of Exercise and Physical Activity On Knee OsteoarthritisDocument9 pagesEffects of Exercise and Physical Activity On Knee OsteoarthritisJoseph LimNo ratings yet
- PROHEALTH: Physiotherapy Rehabilitation and Research Center For Musculoskeletal ConditionsDocument36 pagesPROHEALTH: Physiotherapy Rehabilitation and Research Center For Musculoskeletal ConditionsJohn Gabriel SamsonNo ratings yet
- Guided Imagery For Arthritis and Other Rheumatic Diseases: A Systematic Review of Randomized Controlled TrialsDocument12 pagesGuided Imagery For Arthritis and Other Rheumatic Diseases: A Systematic Review of Randomized Controlled TrialsHikmah AlamiahNo ratings yet
- Examine The Impact of Arthritis On Elderly People in Umunko Igbo Etiti Local Government Area of Enugu StateDocument39 pagesExamine The Impact of Arthritis On Elderly People in Umunko Igbo Etiti Local Government Area of Enugu Stateigweonyia gabrielNo ratings yet
- Health-Related Quality of Life in Chronic Renal Predialysis Patients Exposed To A Prevention Program - Medellín, 2007-2008Document14 pagesHealth-Related Quality of Life in Chronic Renal Predialysis Patients Exposed To A Prevention Program - Medellín, 2007-2008Alejandro Vesga VinchiraNo ratings yet
- Ijerph 19 02559Document13 pagesIjerph 19 02559Luisa BarbeitoNo ratings yet
- Health-Related Quality of Life and Its Predictors Among Outpatients With Coronary PDFDocument6 pagesHealth-Related Quality of Life and Its Predictors Among Outpatients With Coronary PDFPebri MarbunNo ratings yet
- Article SummaryDocument1 pageArticle SummaryMALIK MANASRAHNo ratings yet
- Nermeen Statment of ProblemDocument2 pagesNermeen Statment of ProblemMALIK MANASRAHNo ratings yet
- AL Quads UniversityDocument108 pagesAL Quads UniversityMALIK MANASRAHNo ratings yet
- Coronavirus Manifestaciones OcularesDocument6 pagesCoronavirus Manifestaciones OcularesJohny Marquez TrochezNo ratings yet
- Statment of Problem FeverDocument1 pageStatment of Problem FeverMALIK MANASRAHNo ratings yet
- Critical Appraisal Tools Will Be UsedDocument2 pagesCritical Appraisal Tools Will Be UsedMALIK MANASRAHNo ratings yet
- Qualitative Research CritiqueDocument12 pagesQualitative Research CritiqueCatherine ManaloNo ratings yet
- Cyber Crime and Its Effects On Youth: An Empirical Study On MBSTU StudentsDocument55 pagesCyber Crime and Its Effects On Youth: An Empirical Study On MBSTU StudentsMALIK MANASRAHNo ratings yet
- Statment Problem 2Document1 pageStatment Problem 2MALIK MANASRAHNo ratings yet
- Faculty of Higher Education: Rawan Abu DayyahDocument31 pagesFaculty of Higher Education: Rawan Abu DayyahMALIK MANASRAHNo ratings yet
- Developing A Neonatal Unit Ventilation Protocol For The Preterm BabyDocument6 pagesDeveloping A Neonatal Unit Ventilation Protocol For The Preterm BabyMALIK MANASRAHNo ratings yet
- Article SummaryDocument1 pageArticle SummaryMALIK MANASRAHNo ratings yet
- Weaning de VM Con Protocolo Computarizado Int Care Med 2013Document7 pagesWeaning de VM Con Protocolo Computarizado Int Care Med 2013MALIK MANASRAHNo ratings yet
- Proforma For Registration of Subject For: DissertationDocument24 pagesProforma For Registration of Subject For: DissertationMALIK MANASRAHNo ratings yet
- Proforma For Registration of Subject For DissertationDocument24 pagesProforma For Registration of Subject For DissertationMALIK MANASRAHNo ratings yet
- Comparing Teaching Methods Using BiostatisticsDocument7 pagesComparing Teaching Methods Using BiostatisticsMALIK MANASRAHNo ratings yet
- Al-Quds University Department of MidwiferyDocument7 pagesAl-Quds University Department of MidwiferyMALIK MANASRAHNo ratings yet
- Weaning Infants From Mechanical Ventilation: Clinics in Perinatology September 2012Document21 pagesWeaning Infants From Mechanical Ventilation: Clinics in Perinatology September 2012MALIK MANASRAHNo ratings yet
- Key Differences Between Language and MathematicsDocument1 pageKey Differences Between Language and MathematicsMALIK MANASRAHNo ratings yet
- Our Health Is The Most Important Thing in LifeDocument1 pageOur Health Is The Most Important Thing in LifeMALIK MANASRAHNo ratings yet
- Quality of Antnatal Care July 2018Document11 pagesQuality of Antnatal Care July 2018MALIK MANASRAHNo ratings yet
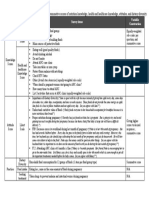
- Table S1: Survey Items Used To Generate Dependent Summative Scores of Nutrition Knowledge, Health and Healthcare Knowledge, Attitudes, and Dietary DiversityDocument1 pageTable S1: Survey Items Used To Generate Dependent Summative Scores of Nutrition Knowledge, Health and Healthcare Knowledge, Attitudes, and Dietary DiversityMALIK MANASRAHNo ratings yet
- Pressure Ulcer ExperiencesDocument7 pagesPressure Ulcer ExperiencesChassie BarberNo ratings yet
- Clinical Risk Factors Associated With Extubation Failure in Ventilated NeonatesDocument4 pagesClinical Risk Factors Associated With Extubation Failure in Ventilated NeonatesMALIK MANASRAHNo ratings yet
- Ed574784 PDFDocument8 pagesEd574784 PDFMALIK MANASRAHNo ratings yet
- Introduction and Literature ReviewDocument4 pagesIntroduction and Literature ReviewMALIK MANASRAHNo ratings yet
- Missed Ischemic Stroke Diagnosis in The Emergency Department by Emergency Medicine and Neurology ServicesDocument2 pagesMissed Ischemic Stroke Diagnosis in The Emergency Department by Emergency Medicine and Neurology ServicesMALIK MANASRAHNo ratings yet
- Location vs. SizeDocument2 pagesLocation vs. Sizeisra al-awawdehNo ratings yet
- 20604-Article Text-65316-2-10-20180726 PDFDocument8 pages20604-Article Text-65316-2-10-20180726 PDFMALIK MANASRAHNo ratings yet
- Becoming A Graduate Professional Psychologist: in What Ways Are Professional Competences PerceivedDocument13 pagesBecoming A Graduate Professional Psychologist: in What Ways Are Professional Competences PerceivedMALIK MANASRAHNo ratings yet
- Chap 20Document36 pagesChap 20kswann2No ratings yet
- Wcet2016 Programme and Abstract BookDocument64 pagesWcet2016 Programme and Abstract BookMohyuddin A MaroofNo ratings yet
- American Cancer SocietyDocument40 pagesAmerican Cancer Societybrunna_pultzNo ratings yet
- History Taking in PsychiatryDocument3 pagesHistory Taking in PsychiatryJuan Cruz FenrirNo ratings yet
- TMBU Cleaning and Disinfection Policy 2012Document10 pagesTMBU Cleaning and Disinfection Policy 2012ver_at_workNo ratings yet
- ESAP 2015 Laboratory Reference RangesDocument5 pagesESAP 2015 Laboratory Reference RangesLady Nell Descanzo100% (1)
- KyphosisDocument3 pagesKyphosismnatuelNo ratings yet
- AXA eMedic Medical Plan SummaryDocument4 pagesAXA eMedic Medical Plan SummaryAfiq de WinnerNo ratings yet
- Armfield and Heaton - 2013 - Management of Fear and Anxiety in The Dental Clinic - A ReviewDocument18 pagesArmfield and Heaton - 2013 - Management of Fear and Anxiety in The Dental Clinic - A ReviewdiegowildbergerNo ratings yet
- Plastic Wastes Management Control Recycling and DisposalDocument490 pagesPlastic Wastes Management Control Recycling and DisposalBenjamin CoatesNo ratings yet
- MHO Vision & MissionDocument10 pagesMHO Vision & MissionJoEd VillAlonNo ratings yet
- Burning Mouth Syndrome Causes & TreatmentsDocument4 pagesBurning Mouth Syndrome Causes & TreatmentsGhada AlqrnawiNo ratings yet
- VolvulusDocument20 pagesVolvulusParul VarshneyNo ratings yet
- Bell's PalsyDocument12 pagesBell's PalsyMercy nafulaNo ratings yet
- Dr. Daniel H. Bessesen: The Biology of ObesityDocument58 pagesDr. Daniel H. Bessesen: The Biology of ObesityNational Press FoundationNo ratings yet
- Colostomy CareDocument13 pagesColostomy CareLord Pozak MillerNo ratings yet
- Cramer Understanding Defense MechanismsDocument30 pagesCramer Understanding Defense MechanismsTiberiu100% (1)
- Contracted Endodontic AccessDocument48 pagesContracted Endodontic AccessSanket Pandey93% (27)
- Dermatologic Therapeutics 1Document38 pagesDermatologic Therapeutics 1Ashraf AboNo ratings yet
- WHO-GMP Guidlines For Pharmaceutical IndustriesDocument148 pagesWHO-GMP Guidlines For Pharmaceutical Industriesmoo78100% (5)
- Herbal Medicine Guide: Benefits, Uses and Safety TipsDocument12 pagesHerbal Medicine Guide: Benefits, Uses and Safety TipsVer BautistaNo ratings yet
- Scapula DyskinesiaDocument5 pagesScapula Dyskinesiamiguelax1No ratings yet
- Chapter 41 - Thoracic Outlet Syndrome SynonymsDocument8 pagesChapter 41 - Thoracic Outlet Syndrome SynonymsPiero Massafra100% (1)
- University of Santo Tomas: The Graduate SchoolDocument19 pagesUniversity of Santo Tomas: The Graduate SchoolJohn Henry ValenciaNo ratings yet
- Decentralized Waste Water TMT System - SeminarDocument25 pagesDecentralized Waste Water TMT System - SeminardhanushNo ratings yet
- BIOMEDICAL COMPETENCY ACCORDING TO COPDocument52 pagesBIOMEDICAL COMPETENCY ACCORDING TO COPMuhammad Iqwan Mustaffa100% (1)
- Book Excerpt: 'Psychology's Ghost: The Crisis in The Profession and The Way Back'Document5 pagesBook Excerpt: 'Psychology's Ghost: The Crisis in The Profession and The Way Back'WBURNo ratings yet
- HHS Pre-doctoral Internship in Clinical NeuropsychologyDocument10 pagesHHS Pre-doctoral Internship in Clinical NeuropsychologyGifuGifuNo ratings yet
- An Abusive Father and The Effects On A Young WomanDocument2 pagesAn Abusive Father and The Effects On A Young WomanJennalyn CasapaoNo ratings yet
- Pelvic Floor Exercise For Urinary Incontinence A Systematic Literature Review PDFDocument7 pagesPelvic Floor Exercise For Urinary Incontinence A Systematic Literature Review PDFAlexandra SilvaNo ratings yet
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionFrom EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNo ratings yet
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (38)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- Don't Panic: Taking Control of Anxiety AttacksFrom EverandDon't Panic: Taking Control of Anxiety AttacksRating: 4 out of 5 stars4/5 (12)
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaFrom EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaRating: 4.5 out of 5 stars4.5/5 (56)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (140)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveFrom EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveRating: 4 out of 5 stars4/5 (249)
- When Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionFrom EverandWhen Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionRating: 4 out of 5 stars4/5 (11)
- Call of the Wild: How We Heal Trauma, Awaken Our Own Power, and Use It For GoodFrom EverandCall of the Wild: How We Heal Trauma, Awaken Our Own Power, and Use It For GoodNo ratings yet
- BORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONFrom EverandBORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONRating: 4.5 out of 5 stars4.5/5 (24)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreFrom EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreRating: 5 out of 5 stars5/5 (17)
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeFrom EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeRating: 4.5 out of 5 stars4.5/5 (49)
- Overcoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsFrom EverandOvercoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsRating: 4.5 out of 5 stars4.5/5 (48)
- Insecure in Love: How Anxious Attachment Can Make You Feel Jealous, Needy, and Worried and What You Can Do About ItFrom EverandInsecure in Love: How Anxious Attachment Can Make You Feel Jealous, Needy, and Worried and What You Can Do About ItRating: 4.5 out of 5 stars4.5/5 (84)
- Fighting Words Devotional: 100 Days of Speaking Truth into the DarknessFrom EverandFighting Words Devotional: 100 Days of Speaking Truth into the DarknessRating: 5 out of 5 stars5/5 (6)
- The Somatic Psychotherapy Toolbox: A Comprehensive Guide to Healing Trauma and StressFrom EverandThe Somatic Psychotherapy Toolbox: A Comprehensive Guide to Healing Trauma and StressNo ratings yet
- Binaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationFrom EverandBinaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationRating: 5 out of 5 stars5/5 (9)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesFrom EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesRating: 5 out of 5 stars5/5 (70)
- Winning the War in Your Mind: Change Your Thinking, Change Your LifeFrom EverandWinning the War in Your Mind: Change Your Thinking, Change Your LifeRating: 5 out of 5 stars5/5 (558)
- Smart Phone Dumb Phone: Free Yourself from Digital AddictionFrom EverandSmart Phone Dumb Phone: Free Yourself from Digital AddictionRating: 5 out of 5 stars5/5 (11)
- Anxious for Nothing: Finding Calm in a Chaotic WorldFrom EverandAnxious for Nothing: Finding Calm in a Chaotic WorldRating: 4.5 out of 5 stars4.5/5 (1243)