You might also like
- Weaning Infants From Mechanical Ventilation: Clinics in Perinatology September 2012Document21 pagesWeaning Infants From Mechanical Ventilation: Clinics in Perinatology September 2012MALIK MANASRAHNo ratings yet
- Non InvasiveventilationDocument10 pagesNon InvasiveventilationpiusputraNo ratings yet
- Artigo 2 CinhalDocument7 pagesArtigo 2 CinhalSara PereiraNo ratings yet
- 232 FullDocument14 pages232 FullCarlos OliveiraNo ratings yet
- Pediatric Anesthesia - 2022 - Weatherall - Developing An Extubation Strategy For The Difficult Pediatric Airway Who WhenDocument8 pagesPediatric Anesthesia - 2022 - Weatherall - Developing An Extubation Strategy For The Difficult Pediatric Airway Who WhenPamela Mamani FloresNo ratings yet
- A Framework For The Management of The Pediatric AirwayDocument23 pagesA Framework For The Management of The Pediatric AirwayDaniel GallegoNo ratings yet
- Protocolos Weaining 2011Document14 pagesProtocolos Weaining 2011perla islasNo ratings yet
- Mechanical Ventilation of The Premature NeonateDocument16 pagesMechanical Ventilation of The Premature NeonateHaitham HafezNo ratings yet
- Use of a Shared Canister Protocol for the Delivery of Metereddose Inhalers in Mechanically Ventilated Subjects 2016 American Association for Respiratory CareDocument8 pagesUse of a Shared Canister Protocol for the Delivery of Metereddose Inhalers in Mechanically Ventilated Subjects 2016 American Association for Respiratory CareevyNo ratings yet
- Neoreviews 2013 Keszler E237 51Document17 pagesNeoreviews 2013 Keszler E237 51Gun HawkNo ratings yet
- Acute Respiratory Distress Syndrome (ARDS) Developed Clinical Pathway: Suggested ProtocolDocument6 pagesAcute Respiratory Distress Syndrome (ARDS) Developed Clinical Pathway: Suggested ProtocolRia sasmitaNo ratings yet
- Lost in Knowledge Translation: Time For A Map?Document12 pagesLost in Knowledge Translation: Time For A Map?Elaine SilveiraNo ratings yet
- Evidence Based Critical CareDocument6 pagesEvidence Based Critical CareSreetamSahaNo ratings yet
- Ventilator Weaning Protocols: Influencing Outcomes and Promoting SuccessDocument32 pagesVentilator Weaning Protocols: Influencing Outcomes and Promoting SuccessarinNo ratings yet
- 5 Nursing Strategies To Prevent Ventilator-Associated PneumoniaDocument5 pages5 Nursing Strategies To Prevent Ventilator-Associated PneumoniaPaulo Henrique SoaresNo ratings yet
- Paramedics and Scope of Practice: EditorialsDocument3 pagesParamedics and Scope of Practice: Editorialsbibin babuNo ratings yet
- Prevention Work AccidentDocument6 pagesPrevention Work AccidenthumairohimaniaNo ratings yet
- Rajiv Gandhi University of Health Sciences, Bangalore, Karnataka Annexure - Ii Proforma For Registration of Subject For DissertationDocument17 pagesRajiv Gandhi University of Health Sciences, Bangalore, Karnataka Annexure - Ii Proforma For Registration of Subject For DissertationyashramawatNo ratings yet
- Comparison Between Personal Protective Equipment WDocument12 pagesComparison Between Personal Protective Equipment WnalgatronNo ratings yet
- Paediatric Mechanical Ventilation in The Intensive Care UnitDocument5 pagesPaediatric Mechanical Ventilation in The Intensive Care UnitAndres RiveraNo ratings yet
- Nursing and Patient Safety in The Operating Room: Journal of Advanced Nursing February 2008Document10 pagesNursing and Patient Safety in The Operating Room: Journal of Advanced Nursing February 2008Bung HerryNo ratings yet
- Curtis - Et - Al-2017-Journal - of - Clinical - Nursing Key Principles To Building Knowledge Translation Into Research DesignDocument11 pagesCurtis - Et - Al-2017-Journal - of - Clinical - Nursing Key Principles To Building Knowledge Translation Into Research DesignAnonymous e1pLzUCMHNo ratings yet
- FasdfyDocument8 pagesFasdfyzuliamNo ratings yet
- Paediatric Mechanical Ventilation in The Intensive Care UnitDocument5 pagesPaediatric Mechanical Ventilation in The Intensive Care UnitdmallozziNo ratings yet
- 1466 FullDocument15 pages1466 FullMelvy RozaNo ratings yet
- Improving Patient Safety in Haemodialysis: Editorial CommentDocument3 pagesImproving Patient Safety in Haemodialysis: Editorial CommentNurul Maliki Rayun IttaqaNo ratings yet
- Dif Ficult Airway Society 2015 Guidelines For Management of Unanticipated Dif Ficult Intubation in AdultsDocument22 pagesDif Ficult Airway Society 2015 Guidelines For Management of Unanticipated Dif Ficult Intubation in AdultsJhonatan LadinoNo ratings yet
- Paediatric Mechanical Ventilation in The Intensive Care UnitDocument5 pagesPaediatric Mechanical Ventilation in The Intensive Care UnitImmakulata LovinaNo ratings yet
- Conti 2016Document7 pagesConti 2016Dwi Putri SekariniNo ratings yet
- Ni Hms 634302Document11 pagesNi Hms 634302fikaanugrahNo ratings yet
- Struggling For A Feasible Tool - The Process of Implementing A Clinical Pathway in Intensive Care: A Grounded Theory StudyDocument15 pagesStruggling For A Feasible Tool - The Process of Implementing A Clinical Pathway in Intensive Care: A Grounded Theory StudyHarumiNo ratings yet
- BOE & BOCP Oral Care TecnicDocument5 pagesBOE & BOCP Oral Care TecnicsarintiNo ratings yet
- Interventions To Decrease Catheter-Related Bloodstream Infections in The ICU: The Keystone Intensive Care Unit ProjectDocument5 pagesInterventions To Decrease Catheter-Related Bloodstream Infections in The ICU: The Keystone Intensive Care Unit ProjectanggitaNo ratings yet
- Airway Management in Pre-Hospital Critical Care: A Review of The Evidence For A Top Five ' Research PriorityDocument6 pagesAirway Management in Pre-Hospital Critical Care: A Review of The Evidence For A Top Five ' Research PriorityMeska AmeliaNo ratings yet
- Hagberg 2015Document3 pagesHagberg 2015fadhila_nurrahmaNo ratings yet
- Vía Aerea DificilDocument22 pagesVía Aerea Dificilcoyotito961No ratings yet
- Nursing Patient Safety in Or-With-Cover-Page-V2Document10 pagesNursing Patient Safety in Or-With-Cover-Page-V2gaynuwanketengNo ratings yet
- Weaning An Adult Patient From Invasive Mechanical VentilationDocument22 pagesWeaning An Adult Patient From Invasive Mechanical VentilationYuanda ArztNo ratings yet
- 2019 A Phase II randomized controlled trial for lung and diaphragm protective ventilationDocument7 pages2019 A Phase II randomized controlled trial for lung and diaphragm protective ventilationwilsonmauriciolozanoNo ratings yet
- Jama Blackwood 2021 Oi 210072 1635864574.9934Document10 pagesJama Blackwood 2021 Oi 210072 1635864574.9934Itzel ArredondoNo ratings yet
- Weanning EstrategiasDocument7 pagesWeanning EstrategiasterapiafisicapilaresNo ratings yet
- Nursing and Patient Safety in The Operating RoomDocument10 pagesNursing and Patient Safety in The Operating RoomJoe AbelloNo ratings yet
- Volume Targeted VentilationDocument28 pagesVolume Targeted VentilationhosnameskarNo ratings yet
- Dif Ficult Airway Society 2015 Guidelines For Management of Unanticipated Dif Ficult Intubation in AdultsDocument22 pagesDif Ficult Airway Society 2015 Guidelines For Management of Unanticipated Dif Ficult Intubation in AdultsrezaNo ratings yet
- Delerium CEA Systematic ReviewDocument30 pagesDelerium CEA Systematic ReviewK. O.No ratings yet
- An Evidence-Based Protocol For Immediate Rehabilitation of The Edentulous PatientDocument10 pagesAn Evidence-Based Protocol For Immediate Rehabilitation of The Edentulous PatientFRANCISCO JAVIER BRAVO RIVEROSNo ratings yet
- Lower Versus Higher Oxygen Concentration For Delivery Room Stabilisation of Preterm Neonates: Systematic ReviewDocument8 pagesLower Versus Higher Oxygen Concentration For Delivery Room Stabilisation of Preterm Neonates: Systematic ReviewBudi RahardjoNo ratings yet
- Areas of Research Interest in Airway Management: Direction and GapsDocument3 pagesAreas of Research Interest in Airway Management: Direction and GapsLaras Bani WasesoNo ratings yet
- Care bundles in intensive care medicineDocument4 pagesCare bundles in intensive care medicineYashoda PereraNo ratings yet
- Algorythme Airway Difficile 2015 (DAS)Document22 pagesAlgorythme Airway Difficile 2015 (DAS)Cedric VaillesNo ratings yet
- Vent Weaning Ped22Document9 pagesVent Weaning Ped22Obed AhumadaNo ratings yet
- Rajiv Gandhi University of Health Sciences, Bangalore, KarnatakaDocument17 pagesRajiv Gandhi University of Health Sciences, Bangalore, KarnatakayashramawatNo ratings yet
- Jarvis 2014Document6 pagesJarvis 2014lalaNo ratings yet
- ClinKidneyJ 2015 Marcelli CKJ - Sfu145Document7 pagesClinKidneyJ 2015 Marcelli CKJ - Sfu145Bung HerryNo ratings yet
- Articulo Hernia OriginalDocument7 pagesArticulo Hernia OriginalmelvaNo ratings yet
- 1472 6882 12 88Document9 pages1472 6882 12 88Doctora SantanaNo ratings yet
- Enhanced Recovery After Elective Caesarean A RapidDocument11 pagesEnhanced Recovery After Elective Caesarean A Rapidselfie rijalNo ratings yet
- 1fca PDFDocument13 pages1fca PDFHalim SudonoNo ratings yet
- The Vortex Approach: Management of the Unanticipated Difficult AirwayFrom EverandThe Vortex Approach: Management of the Unanticipated Difficult AirwayRating: 5 out of 5 stars5/5 (1)
- Advanced Practice and Leadership in Radiology NursingFrom EverandAdvanced Practice and Leadership in Radiology NursingKathleen A. GrossNo ratings yet
- Nermeen Statment of ProblemDocument2 pagesNermeen Statment of ProblemMALIK MANASRAHNo ratings yet
- Coronavirus Manifestaciones OcularesDocument6 pagesCoronavirus Manifestaciones OcularesJohny Marquez TrochezNo ratings yet
- AL Quads UniversityDocument108 pagesAL Quads UniversityMALIK MANASRAHNo ratings yet
- Article SummaryDocument1 pageArticle SummaryMALIK MANASRAHNo ratings yet
- Statment of Problem FeverDocument1 pageStatment of Problem FeverMALIK MANASRAHNo ratings yet
- Qualitative Research CritiqueDocument12 pagesQualitative Research CritiqueCatherine ManaloNo ratings yet
- Article SummaryDocument1 pageArticle SummaryMALIK MANASRAHNo ratings yet
- Statment Problem 2Document1 pageStatment Problem 2MALIK MANASRAHNo ratings yet
- Proforma For Registration of Subject For: DissertationDocument24 pagesProforma For Registration of Subject For: DissertationMALIK MANASRAHNo ratings yet
- Critical Appraisal Tools Will Be UsedDocument2 pagesCritical Appraisal Tools Will Be UsedMALIK MANASRAHNo ratings yet
- Introduction and Literature ReviewDocument4 pagesIntroduction and Literature ReviewMALIK MANASRAHNo ratings yet
- Proforma For Registration of Subject For DissertationDocument24 pagesProforma For Registration of Subject For DissertationMALIK MANASRAHNo ratings yet
- Faculty of Higher Education: Rawan Abu DayyahDocument31 pagesFaculty of Higher Education: Rawan Abu DayyahMALIK MANASRAHNo ratings yet
- Cyber Crime and Its Effects On Youth: An Empirical Study On MBSTU StudentsDocument55 pagesCyber Crime and Its Effects On Youth: An Empirical Study On MBSTU StudentsMALIK MANASRAHNo ratings yet
- Quality of Antnatal Care July 2018Document11 pagesQuality of Antnatal Care July 2018MALIK MANASRAHNo ratings yet
- Weaning de VM Con Protocolo Computarizado Int Care Med 2013Document7 pagesWeaning de VM Con Protocolo Computarizado Int Care Med 2013MALIK MANASRAHNo ratings yet
- Pressure Ulcer ExperiencesDocument7 pagesPressure Ulcer ExperiencesChassie BarberNo ratings yet
- Our Health Is The Most Important Thing in LifeDocument1 pageOur Health Is The Most Important Thing in LifeMALIK MANASRAHNo ratings yet
- Key Differences Between Language and MathematicsDocument1 pageKey Differences Between Language and MathematicsMALIK MANASRAHNo ratings yet
- Location vs. SizeDocument2 pagesLocation vs. Sizeisra al-awawdehNo ratings yet
- Al-Quds University Department of MidwiferyDocument7 pagesAl-Quds University Department of MidwiferyMALIK MANASRAHNo ratings yet
- Missed Ischemic Stroke Diagnosis in The Emergency Department by Emergency Medicine and Neurology ServicesDocument2 pagesMissed Ischemic Stroke Diagnosis in The Emergency Department by Emergency Medicine and Neurology ServicesMALIK MANASRAHNo ratings yet
- Comparing Teaching Methods Using BiostatisticsDocument7 pagesComparing Teaching Methods Using BiostatisticsMALIK MANASRAHNo ratings yet
- Clinical Risk Factors Associated With Extubation Failure in Ventilated NeonatesDocument4 pagesClinical Risk Factors Associated With Extubation Failure in Ventilated NeonatesMALIK MANASRAHNo ratings yet
- 20604-Article Text-65316-2-10-20180726 PDFDocument8 pages20604-Article Text-65316-2-10-20180726 PDFMALIK MANASRAHNo ratings yet
- Ed574784 PDFDocument8 pagesEd574784 PDFMALIK MANASRAHNo ratings yet
- Becoming A Graduate Professional Psychologist: in What Ways Are Professional Competences PerceivedDocument13 pagesBecoming A Graduate Professional Psychologist: in What Ways Are Professional Competences PerceivedMALIK MANASRAHNo ratings yet
- Table S1: Survey Items Used To Generate Dependent Summative Scores of Nutrition Knowledge, Health and Healthcare Knowledge, Attitudes, and Dietary DiversityDocument1 pageTable S1: Survey Items Used To Generate Dependent Summative Scores of Nutrition Knowledge, Health and Healthcare Knowledge, Attitudes, and Dietary DiversityMALIK MANASRAHNo ratings yet
- Wiring Harness Installation Instructions: For InstallersDocument12 pagesWiring Harness Installation Instructions: For Installersnirut_niceguyNo ratings yet
- 1N4001S THRU 1N4007S: General Purpose Silicon RectifierDocument2 pages1N4001S THRU 1N4007S: General Purpose Silicon RectifierBhadreshkumar SharmaNo ratings yet
- Model AnswerDocument27 pagesModel AnswerdishaNo ratings yet
- The Human BodyDocument17 pagesThe Human BodyRuthie MendozaNo ratings yet
- Mushroom Umami Taste EvaluationDocument10 pagesMushroom Umami Taste EvaluationMaryam HanifNo ratings yet
- DSBV87ALP Two-Stage Differential Pressure Control Valve SpecsDocument2 pagesDSBV87ALP Two-Stage Differential Pressure Control Valve SpecsadrianioantomaNo ratings yet
- Footing BiaxialDocument33 pagesFooting BiaxialSanthoshkumar RayavarapuNo ratings yet
- AEIOU Framework - Case Study On Agriculture Domain (Automatic Drip Tube Irrigation System)Document30 pagesAEIOU Framework - Case Study On Agriculture Domain (Automatic Drip Tube Irrigation System)Kunal TalegaonkarNo ratings yet
- LinearDocument46 pagesLinearSheikh Riasat100% (1)
- Revisiting The Irish Royal Sites: Susan A. JohnstonDocument7 pagesRevisiting The Irish Royal Sites: Susan A. JohnstonJacek RomanowNo ratings yet
- Syngo MR E11 OncoDocument64 pagesSyngo MR E11 OncoLuís GuerraNo ratings yet
- WB City GateDocument7 pagesWB City GateDiegoNo ratings yet
- MAGA Training ReportDocument56 pagesMAGA Training ReportChaturanga WagaArachchige67% (3)
- User Manual For Digital Logic Trainer KitDocument6 pagesUser Manual For Digital Logic Trainer KitHonnura HarijanaNo ratings yet
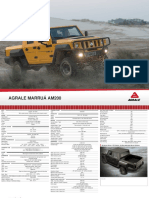
- Off Road and Military Vehicles Off Road Vehicles Agrale Marruaam200 1Document2 pagesOff Road and Military Vehicles Off Road Vehicles Agrale Marruaam200 1Victor SilvaNo ratings yet
- Basic Integration Problems #1Document4 pagesBasic Integration Problems #1John Marlo GorobaoNo ratings yet
- Profitability Analysis Report SampleDocument11 pagesProfitability Analysis Report SampleArfel Marie FuentesNo ratings yet
- MAD Magazine 001Document36 pagesMAD Magazine 001ClarkcoffeyNo ratings yet
- Aisladores Polimericos vs. Aisladores Ceramicos Unmsm PDFDocument22 pagesAisladores Polimericos vs. Aisladores Ceramicos Unmsm PDFvgcasasNo ratings yet
- 3D Bioprinting From The Micrometer To Millimete 2017 Current Opinion in BiomDocument7 pages3D Bioprinting From The Micrometer To Millimete 2017 Current Opinion in Biomrrm77No ratings yet
- SP18368 Automotive Radar Comparison 2018 Sample 2Document33 pagesSP18368 Automotive Radar Comparison 2018 Sample 2Chipisgood YuNo ratings yet
- Diagnoza Wstępna Klasa IDocument3 pagesDiagnoza Wstępna Klasa IMagda StręciwilkNo ratings yet
- Schutz - Subnotes PDFDocument47 pagesSchutz - Subnotes PDFJarryd RastiNo ratings yet
- Rectal FluidtherapyDocument7 pagesRectal FluidtherapyIan SabogalNo ratings yet
- Hoist by TechnologyDocument6 pagesHoist by TechnologyAnonymous ntE0hG2TPNo ratings yet
- Philosophical Transactions of The Royal Society of LondonDocument716 pagesPhilosophical Transactions of The Royal Society of Londonab opt100% (1)
- CompressorsDocument20 pagesCompressorsCarlos Alberto Huamaní GonzalesNo ratings yet
- 3 Uscg BWM VRPDocument30 pages3 Uscg BWM VRPdivinusdivinusNo ratings yet
- Mischel2004 - Toward An Integrative Science of The PersonDocument24 pagesMischel2004 - Toward An Integrative Science of The PersonTibor GalacziNo ratings yet
- Towards Sustainable Water Management in SoharDocument48 pagesTowards Sustainable Water Management in SoharMiss Preyashi kumarNo ratings yet