You might also like
- Intermittent FastingDocument14 pagesIntermittent FastingJéssica AssisNo ratings yet
- Bodybuilding ManualDocument308 pagesBodybuilding ManualM.Emre Doğru100% (2)
- Giving and Receiving Feedback: Approximate Time To Complete Module: 10 MinutesDocument19 pagesGiving and Receiving Feedback: Approximate Time To Complete Module: 10 MinutesMarinel June PalerNo ratings yet
- Rheumatoid FactorDocument21 pagesRheumatoid FactorMuhamad Wirawan AdityoNo ratings yet
- Fast Facts: Measurable Residual Disease: A clearer picture for treatment decisionsFrom EverandFast Facts: Measurable Residual Disease: A clearer picture for treatment decisionsNo ratings yet
- Critical Appraisal EBM-Therapy Journal IDocument29 pagesCritical Appraisal EBM-Therapy Journal IJosephine IrenaNo ratings yet
- MEHLMANMEDICAL - Biostatistics ReviewDocument63 pagesMEHLMANMEDICAL - Biostatistics ReviewSamit LamichhaneNo ratings yet
- The Newborn ExaminationDocument132 pagesThe Newborn ExaminationdevilstNo ratings yet
- Civic Education PamphletDocument18 pagesCivic Education PamphletChikuta Shingalili100% (1)
- Lynn Kern KoegelDocument13 pagesLynn Kern Koegelapi-500451341No ratings yet
- Open Book API 510 Practice Exam B Do Not Mark On Your Exam, Use The Answer Sheets ProvidedDocument16 pagesOpen Book API 510 Practice Exam B Do Not Mark On Your Exam, Use The Answer Sheets ProvidedBeantickNo ratings yet
- Recall 3Document22 pagesRecall 3Christine Rodriguez-Guerrero100% (4)
- Question 36 Begins The Closed Book Portion of This ExamDocument25 pagesQuestion 36 Begins The Closed Book Portion of This ExamBeantickNo ratings yet
- 0otcw KtsifDocument28 pages0otcw KtsifHadji FaroukNo ratings yet
- PSORIASISDocument20 pagesPSORIASISMRFKJ CasanovaNo ratings yet
- Pneumoniae, Was The First Acute-Phase Protein To Be Described and Is An ExquisitelyDocument11 pagesPneumoniae, Was The First Acute-Phase Protein To Be Described and Is An ExquisitelyLabontu IustinaNo ratings yet
- Invisible TransfusionDocument6 pagesInvisible TransfusionPolishLovePoliceNo ratings yet
- CRP TestDocument2 pagesCRP Testces8bautistaNo ratings yet
- Radioimmunoassay Early Stages of Detection of CancerDocument3 pagesRadioimmunoassay Early Stages of Detection of Cancer909 Devang GawasNo ratings yet
- Laboratory Test Results: BloodDocument4 pagesLaboratory Test Results: BloodLukes GutierrezNo ratings yet
- Winda Rohmawati (20130662105)Document6 pagesWinda Rohmawati (20130662105)Faridatin NikmahNo ratings yet
- Antibodies Against A Mutated Citrullinated Vimentin in Patients With Rheumatoid ArthritisDocument17 pagesAntibodies Against A Mutated Citrullinated Vimentin in Patients With Rheumatoid ArthritisReda RamzyNo ratings yet
- Text ADocument21 pagesText AAditi ParmarNo ratings yet
- Blood Tranfusion and TestingDocument4 pagesBlood Tranfusion and Testingsilly GooseNo ratings yet
- Tests To Take Back Your Health: Appendix BDocument19 pagesTests To Take Back Your Health: Appendix BChelsea Green PublishingNo ratings yet
- Autoinmune LaboratorioDocument9 pagesAutoinmune LaboratorioJacob DavisNo ratings yet
- Reading - 3Document19 pagesReading - 3Ratnam hospitalNo ratings yet
- Reading TestDocument196 pagesReading TestKrisselle Ann TanNo ratings yet
- Complement Deficiencies: Description of The Complement System and Its PathwaysDocument5 pagesComplement Deficiencies: Description of The Complement System and Its PathwaysDrTushar GoswamiNo ratings yet
- Antigen-Antibody Reaction-Basic Immunological TechniquesDocument16 pagesAntigen-Antibody Reaction-Basic Immunological TechniquesJesuhovie Solomon OkpobrisiNo ratings yet
- Lecture 3Document17 pagesLecture 3Innocent L NdambakuwaNo ratings yet
- Group 1 BSMT 3A Act. 5.2Document7 pagesGroup 1 BSMT 3A Act. 5.2Gennelyn Ross Delos ReyesNo ratings yet
- Monoclonal Antibodies Are Immune System Proteins That Are Created in The LabDocument3 pagesMonoclonal Antibodies Are Immune System Proteins That Are Created in The Labchrist sonNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument13 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistslidawatiNo ratings yet
- SeroDocument15 pagesSeroSaid IsaqNo ratings yet
- P2.07 - SG8Document8 pagesP2.07 - SG8DeirdreNo ratings yet
- Methods For Microbiological Examination of of FoodDocument5 pagesMethods For Microbiological Examination of of Food9qdd95pw9kNo ratings yet
- CRP WorksheetDocument2 pagesCRP WorksheetSeptheia Maeith VergaraNo ratings yet
- 35 Delèvaux, 2003 PDFDocument5 pages35 Delèvaux, 2003 PDFAndi BintangNo ratings yet
- Pathogenesis and Diagnosis of Anti-GBM Antibody (Goodpasture's) DiseaseDocument18 pagesPathogenesis and Diagnosis of Anti-GBM Antibody (Goodpasture's) DiseaseDicky SangadjiNo ratings yet
- SilvermanDocument7 pagesSilvermanaldarvinNo ratings yet
- Despite ThisDocument2 pagesDespite ThisARIF AHAMMEDNo ratings yet
- Through Secondary Care: The Path To Rheumatoid Arthritis Diagnosis - Your JourneyDocument6 pagesThrough Secondary Care: The Path To Rheumatoid Arthritis Diagnosis - Your Journeyapi-284899538No ratings yet
- Kol Ditz 2016Document3 pagesKol Ditz 2016Lanna HarumiyaNo ratings yet
- MGX of SepticemiaDocument30 pagesMGX of SepticemiaAChRiS--FiTnEsSNo ratings yet
- Sepsis 2023 What Works and What Doesnt Judge Notes For DistributionDocument15 pagesSepsis 2023 What Works and What Doesnt Judge Notes For Distributionsansanee.sucNo ratings yet
- Rheumatoid Arthritis (RA) Is Derived From The Greek Word Rheuma andDocument28 pagesRheumatoid Arthritis (RA) Is Derived From The Greek Word Rheuma andSadaf JavedNo ratings yet
- Immunological Lab Diagnosis of TuberculosisDocument38 pagesImmunological Lab Diagnosis of TuberculosisRasha EmadNo ratings yet
- Complement Fixation Test: Process Testing For Antigen Semi-Quantitative Testing References External LinksDocument2 pagesComplement Fixation Test: Process Testing For Antigen Semi-Quantitative Testing References External LinksYASMINANo ratings yet
- CHAPTER 1 To 9Document42 pagesCHAPTER 1 To 9ALNATRON GROUPSNo ratings yet
- CFT Meet The Following CriteriaDocument2 pagesCFT Meet The Following Criteriappoki2802No ratings yet
- J Diabetes Sci Technol 2009 Ginsberg 903 13Document11 pagesJ Diabetes Sci Technol 2009 Ginsberg 903 13Ninosk Mendoza SolisNo ratings yet
- Erythrocyte Sedimentation Rate: Reaction, Is The Rate at WhichDocument37 pagesErythrocyte Sedimentation Rate: Reaction, Is The Rate at WhichAsmita PatilNo ratings yet
- Module - 7 - Post - Lab DiscussionDocument2 pagesModule - 7 - Post - Lab DiscussionCiara PamonagNo ratings yet
- Royal JellyDocument10 pagesRoyal JellyninukNo ratings yet
- MR Supple All 2014Document429 pagesMR Supple All 2014Regita Ayu LestariNo ratings yet
- Vera Geanella Critical Care Assignment FinalDocument8 pagesVera Geanella Critical Care Assignment Finalapi-496082089No ratings yet
- Mycobacterium Tuberculosis Thesis PDFDocument8 pagesMycobacterium Tuberculosis Thesis PDFrebeccabordescambridge100% (2)
- CHAPTER-17 NUERO MergedDocument17 pagesCHAPTER-17 NUERO MergedRyn ShadowNo ratings yet
- CHAPTER 1 To 9Document43 pagesCHAPTER 1 To 9ALNATRON GROUPSNo ratings yet
- ImmunoassayDocument8 pagesImmunoassayMuhammad AsadNo ratings yet
- Adjusted Survival CurvesDocument26 pagesAdjusted Survival CurvesJhona11anNo ratings yet
- Troponin Testing - Analytical Considerations - UpToDateDocument20 pagesTroponin Testing - Analytical Considerations - UpToDateMiguel Angel PugaNo ratings yet
- Immuno ReportDocument14 pagesImmuno Reportlenny lemoogeNo ratings yet
- Innova Biosciences Antibody Labeling GuideDocument10 pagesInnova Biosciences Antibody Labeling GuideandreaNo ratings yet
- MODULE 3, DIAGNOSTIC EVALUATION (Autosaved)Document19 pagesMODULE 3, DIAGNOSTIC EVALUATION (Autosaved)Randy Ian F. GallegoNo ratings yet
- ProcalcitoninDocument2 pagesProcalcitoninAlec SundetNo ratings yet
- Agranulocytosis, A Simple Guide to The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAgranulocytosis, A Simple Guide to The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- 5077 - Phase 1Document4 pages5077 - Phase 1BeantickNo ratings yet
- Heat Exchangers: WO# PE# Equipment Description WO# DescriptionDocument2 pagesHeat Exchangers: WO# PE# Equipment Description WO# DescriptionBeantickNo ratings yet
- Ceiling Size ViewsDocument1 pageCeiling Size ViewsBeantickNo ratings yet
- Mail Rajindra Benny Akash BalchanDocument2 pagesMail Rajindra Benny Akash BalchanBeantickNo ratings yet
- 2201J IR SurveyDocument5 pages2201J IR SurveyBeantickNo ratings yet
- By Rajindra Benny at 9:59 Am, Mar 06, 2023Document3 pagesBy Rajindra Benny at 9:59 Am, Mar 06, 2023BeantickNo ratings yet
- 5926 - 01 - 2022 - 03 - Water - Tanks - 4#Document1 page5926 - 01 - 2022 - 03 - Water - Tanks - 4#BeantickNo ratings yet
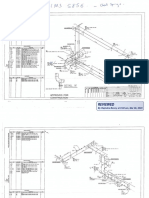
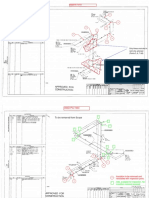
- Approved For Construction: Only Areas Encircled in Red To Be Actioned (Points 5, 6, 7 &8)Document21 pagesApproved For Construction: Only Areas Encircled in Red To Be Actioned (Points 5, 6, 7 &8)BeantickNo ratings yet
- LiclogDocument2 pagesLiclogBeantickNo ratings yet
- JayseearrDocument1 pageJayseearrBeantickNo ratings yet
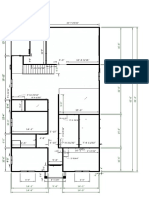
- Top Floor Plan To Mark Decking r2Document1 pageTop Floor Plan To Mark Decking r2BeantickNo ratings yet
- Aims 5006 - UtDocument17 pagesAims 5006 - UtBeantickNo ratings yet
- IX - Atlas Exercise - Rev - 2014Document10 pagesIX - Atlas Exercise - Rev - 2014BeantickNo ratings yet
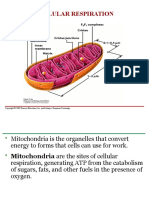
- Cellular RespirationDocument69 pagesCellular RespirationBeantickNo ratings yet
- NDE MatrixDocument1 pageNDE MatrixBeantickNo ratings yet
- Exercise Questions For Section VIII Div.1Document13 pagesExercise Questions For Section VIII Div.1BeantickNo ratings yet
- Cell BiologyDocument5 pagesCell BiologyBeantickNo ratings yet
- Closed Book API 510 Practice Exam C Do Not Mark On Your Exam, Use The Answer Sheets ProvidedDocument22 pagesClosed Book API 510 Practice Exam C Do Not Mark On Your Exam, Use The Answer Sheets ProvidedBeantickNo ratings yet
- Legal Notice No. 270-Public Health 2019 Novel Coronavirus (2019-NCoV) (No. 22) Regulations 2021Document19 pagesLegal Notice No. 270-Public Health 2019 Novel Coronavirus (2019-NCoV) (No. 22) Regulations 2021BeantickNo ratings yet
- The Cell Cycle and DivisionDocument39 pagesThe Cell Cycle and DivisionBeantickNo ratings yet
- Figure 7-1 Essential Cell Biology (© Garland Science 2010)Document32 pagesFigure 7-1 Essential Cell Biology (© Garland Science 2010)BeantickNo ratings yet
- Title: Identification of Gram Positive Organisms Using Various Techniques and Tests. ObjectivesDocument20 pagesTitle: Identification of Gram Positive Organisms Using Various Techniques and Tests. ObjectivesBeantickNo ratings yet
- 2019 DecaboDocument11 pages2019 Decabomahmoudbadr2No ratings yet
- Property Sales Ealing, Greater London 2014-2016: ID Price Paid Deed Date Year Sold Month Sold Postcode Property TypeDocument4 pagesProperty Sales Ealing, Greater London 2014-2016: ID Price Paid Deed Date Year Sold Month Sold Postcode Property TypeBeantickNo ratings yet
- Intermatting Fasting and HUman Metabolic Rate PDFDocument10 pagesIntermatting Fasting and HUman Metabolic Rate PDFsyafira emboabaNo ratings yet
- Intermittent Fasting: A Heart Healthy Dietary Pattern?: ReviewDocument7 pagesIntermittent Fasting: A Heart Healthy Dietary Pattern?: ReviewBeantickNo ratings yet
- Excel Skills For Business: Essentials: Week 6: ChartsDocument3 pagesExcel Skills For Business: Essentials: Week 6: ChartsBeantickNo ratings yet
- JIntOralHealth13110-7155632 015915Document7 pagesJIntOralHealth13110-7155632 015915amanda DhiyaNo ratings yet
- Pharmaceutical Development Q8 (R2) : International Conference On Harmonisation (ICH)Document11 pagesPharmaceutical Development Q8 (R2) : International Conference On Harmonisation (ICH)Md. Akil Mahmud100% (1)
- Background Info, Scope and LimitationsDocument3 pagesBackground Info, Scope and LimitationsSigourney MarianoNo ratings yet
- Zipper Test Purpose-To Test The Flexibility of The Shoulder Girdle. EquipmentDocument16 pagesZipper Test Purpose-To Test The Flexibility of The Shoulder Girdle. EquipmentLanny PerezNo ratings yet
- Report On Rosenberg Self Esteem Scale and Social LoafingDocument10 pagesReport On Rosenberg Self Esteem Scale and Social LoafingRahish AryalNo ratings yet
- Assessment of Health RisksDocument27 pagesAssessment of Health RisksMohamed GHAFFARNo ratings yet
- P.E 1 Module 3Document6 pagesP.E 1 Module 3Cherry lyn EnadNo ratings yet
- Religious Exemption FED-GSA19R-22Document2 pagesReligious Exemption FED-GSA19R-22dvdNo ratings yet
- Scott Floyd WorkbookDocument62 pagesScott Floyd WorkbookDistrict Secretary0% (1)
- Blue Eyes Brown Eyes Nov 10 2021Document31 pagesBlue Eyes Brown Eyes Nov 10 2021Emmy S.U.No ratings yet
- Labia Minora Reconstruction Using Clitoral Hood Flaps, Wedge Excisions, and YV Advancement FlapsDocument8 pagesLabia Minora Reconstruction Using Clitoral Hood Flaps, Wedge Excisions, and YV Advancement FlapsHazel Vivian Soliz AlconzNo ratings yet
- NCP Ineffective Cardiopulmonary PerfusionDocument3 pagesNCP Ineffective Cardiopulmonary PerfusionjamiemapanaoNo ratings yet
- Achilles Tendon Forces and Pain During Common RehabilitationDocument8 pagesAchilles Tendon Forces and Pain During Common RehabilitationIan JuanicoNo ratings yet
- Ramos Persuasive-Essay 3rdDocument3 pagesRamos Persuasive-Essay 3rdMa. Cassandra A. RamosNo ratings yet
- Evaluation of The Screw Tent Pole Technique For The Repair of Anterior MaxillaDocument7 pagesEvaluation of The Screw Tent Pole Technique For The Repair of Anterior MaxillaAna VeronicaNo ratings yet
- Inventory of Drug Taking SituationsDocument2 pagesInventory of Drug Taking SituationsMacarena Segovia ReygadasNo ratings yet
- 31 March 2014 Saudi Commission For Health Specialties PO Box 94656, Riyadh 11614, Kingdom of Saudi Arabia Dear Sir/MadamDocument1 page31 March 2014 Saudi Commission For Health Specialties PO Box 94656, Riyadh 11614, Kingdom of Saudi Arabia Dear Sir/MadamSibil DavidNo ratings yet
- Disqualifying Others - Format Translation TemplateDocument5 pagesDisqualifying Others - Format Translation TemplateclaudialogopedNo ratings yet
- Landmarks For Maxilla and MandibleDocument25 pagesLandmarks For Maxilla and Mandibleوجيه الوجيهNo ratings yet
- Confined Space Pre-Entry Checklist: Mark The Appropriate Column: X Yes, X No, or X N/A Not ApplicableDocument4 pagesConfined Space Pre-Entry Checklist: Mark The Appropriate Column: X Yes, X No, or X N/A Not Applicablereda mesbahNo ratings yet
- Zoono Fact Sheet 53 - Comparison Between Dettol Hand Sanitiser and GermF...Document2 pagesZoono Fact Sheet 53 - Comparison Between Dettol Hand Sanitiser and GermF...Eileen Le RouxNo ratings yet
- The Maudsley Model of FTDocument8 pagesThe Maudsley Model of FTCandela SánchezNo ratings yet
- Lplpo Banguntapan Iii TH 2017Document205 pagesLplpo Banguntapan Iii TH 2017herlinaNo ratings yet
- Six Main Types of Task GroupsDocument3 pagesSix Main Types of Task GroupsAlly AngNo ratings yet
- Nursing Care Plan TemplateDocument5 pagesNursing Care Plan TemplateKyle Albert EstoestaNo ratings yet