You might also like
- Hunger: Mentalization-based Treatments for Eating DisordersFrom EverandHunger: Mentalization-based Treatments for Eating DisordersRating: 1 out of 5 stars1/5 (1)
- 2022 (A) - The Effect of Change in PA Behaviour On DS Among European Older Adults (Human Movement) PDFDocument7 pages2022 (A) - The Effect of Change in PA Behaviour On DS Among European Older Adults (Human Movement) PDFPriscila PintoNo ratings yet
- Body Mass IndexDocument6 pagesBody Mass Indexayu yuliantiNo ratings yet
- 2009 Can Cognitive Exercise Prevent The Onset of Dementia Systematic Review of Randomized Clinical Trials With Longitudinal Follow UpDocument9 pages2009 Can Cognitive Exercise Prevent The Onset of Dementia Systematic Review of Randomized Clinical Trials With Longitudinal Follow UpSergio Machado NeurocientistaNo ratings yet
- ReviewDocument10 pagesReviewCristina Fernández DíazNo ratings yet
- Gender Differences in Major Depressive Disorder: Findings From The Singapore Mental Health StudyDocument7 pagesGender Differences in Major Depressive Disorder: Findings From The Singapore Mental Health StudyFelisia OngNo ratings yet
- Psychiatric and Medical Correlates of DSM-5 Eating Disorders in A Nationally Representative Sample of Adults in The United StatesDocument9 pagesPsychiatric and Medical Correlates of DSM-5 Eating Disorders in A Nationally Representative Sample of Adults in The United StatesManny RosengallegosNo ratings yet
- A-Hudson, Hall & Harkness (2019)Document11 pagesA-Hudson, Hall & Harkness (2019)Jordanitha BhsNo ratings yet
- Relationships Between Obesity, Bipolar Spectrum Features, and Personality Traits: A Case-Control StudyDocument6 pagesRelationships Between Obesity, Bipolar Spectrum Features, and Personality Traits: A Case-Control Studygrymberg5No ratings yet
- JCPP 12590Document15 pagesJCPP 12590Javier CáceresNo ratings yet
- Evaluation of Covid-19 Pandemic - Related Depression in Geriatric Patients at PRH, Loni: A Cross Sectional StudyDocument8 pagesEvaluation of Covid-19 Pandemic - Related Depression in Geriatric Patients at PRH, Loni: A Cross Sectional StudyIJAR JOURNALNo ratings yet
- Journal 2Document8 pagesJournal 2pososuperNo ratings yet
- Quality of Life in Patients With Neurogenic DysphagiaDocument8 pagesQuality of Life in Patients With Neurogenic DysphagiaDaniela OrtizNo ratings yet
- Cognitive Impairment in Late-Life Generalized Anxiety DisorderDocument7 pagesCognitive Impairment in Late-Life Generalized Anxiety DisorderAnais UrdanetaNo ratings yet
- 70490Document22 pages70490alexandra rivasNo ratings yet
- Depression and Its Associated Factors in Older Indians: A Study Based On Study of Global Aging and Adult Health (SAGE) - 2007Document28 pagesDepression and Its Associated Factors in Older Indians: A Study Based On Study of Global Aging and Adult Health (SAGE) - 2007Adina MicuNo ratings yet
- 2022 Teng - Effect of AD On Functioning and Quality of LifeDocument9 pages2022 Teng - Effect of AD On Functioning and Quality of LifeMaria Fernanda AbrahamNo ratings yet
- 2017 Geriatrics&Gerontology International Spanish Traslation of The Kihon ChecklistDocument3 pages2017 Geriatrics&Gerontology International Spanish Traslation of The Kihon ChecklistDanielaa ZapataNo ratings yet
- General Hospital Psychiatry: SciencedirectDocument7 pagesGeneral Hospital Psychiatry: SciencedirectULA HOFINo ratings yet
- Insight and Symptom Severity in An Inpatient Psychiatric SampleDocument12 pagesInsight and Symptom Severity in An Inpatient Psychiatric SamplealejandraNo ratings yet
- Diabetik Dan KelainannyaDocument11 pagesDiabetik Dan Kelainannyalatifah zahrohNo ratings yet
- Long-Term Follow-Up Ofthe Tips Early Detection in Psychosisstudy:Effectson 10-YearoutcomeDocument7 pagesLong-Term Follow-Up Ofthe Tips Early Detection in Psychosisstudy:Effectson 10-YearoutcomeELvine GunawanNo ratings yet
- 08.06.09 - Psychosocial Impact of Dysthymia A Study Among Married PatientsDocument6 pages08.06.09 - Psychosocial Impact of Dysthymia A Study Among Married PatientsRiham AmmarNo ratings yet
- Depression in Adolescents With ASD: A Pilot RCT of A Group InterventionDocument18 pagesDepression in Adolescents With ASD: A Pilot RCT of A Group InterventionyofitaNo ratings yet
- Attendance and Mental Health ProblemsDocument9 pagesAttendance and Mental Health ProblemsgabrielionitamitranNo ratings yet
- Exploring The Clinical Utility of The DSM-5 Conduct Disorder Specifier of With Limited Prosocial Emotions' in An Adolescent Inpatient SampleDocument16 pagesExploring The Clinical Utility of The DSM-5 Conduct Disorder Specifier of With Limited Prosocial Emotions' in An Adolescent Inpatient SampleRicardo EscNo ratings yet
- Content ServerDocument15 pagesContent ServerMárcia SoaresNo ratings yet
- Cognitive Impairment, Behavioral Impairment, Depression, and Wish To Die in An ALS CohortDocument11 pagesCognitive Impairment, Behavioral Impairment, Depression, and Wish To Die in An ALS Cohortjonniwal sanusiNo ratings yet
- Moffitt2015 PDFDocument11 pagesMoffitt2015 PDFRaul Morales VillegasNo ratings yet
- Bell 2019Document12 pagesBell 2019yalocim666No ratings yet
- Progressive Multiple Sclerosis, Cognitive Function, and Quality of LifeDocument7 pagesProgressive Multiple Sclerosis, Cognitive Function, and Quality of LifePaulinhoNo ratings yet
- Brain Sciences: Jean Gagnon, Joséphine Aldebert, Gasser Saleh and Wan Seo KimDocument23 pagesBrain Sciences: Jean Gagnon, Joséphine Aldebert, Gasser Saleh and Wan Seo KimChrysoula GkaniNo ratings yet
- 2021-Young Adult Mental Health Sequelae of Eating and Body Image Disturbances in AdolescenceDocument9 pages2021-Young Adult Mental Health Sequelae of Eating and Body Image Disturbances in AdolescenceMarietta_MonariNo ratings yet
- Generalized Anxiety Disorder in Adults - Epidemiology, Pathogenesis, Clinical Manifestations, Course, Assessment, and Diagnosis - UpToDateDocument17 pagesGeneralized Anxiety Disorder in Adults - Epidemiology, Pathogenesis, Clinical Manifestations, Course, Assessment, and Diagnosis - UpToDateThaiane BarcelosNo ratings yet
- 130 494 1 PB PDFDocument9 pages130 494 1 PB PDFhfathiardiNo ratings yet
- Ni Hms 857824Document18 pagesNi Hms 857824SelyfebNo ratings yet
- Psy Mock Exam NoteDocument8 pagesPsy Mock Exam NoteIssac LiNo ratings yet
- Accepted VersionDocument50 pagesAccepted VersionLautaro FerreiraNo ratings yet
- Effectiveness of Group Reminiscence Therapy On Depression Among The Institutionalized ElderlyDocument8 pagesEffectiveness of Group Reminiscence Therapy On Depression Among The Institutionalized ElderlyIJAR JOURNALNo ratings yet
- Symptoms of Depression and Quality of Life in Functional Dyspepsia PatientsDocument6 pagesSymptoms of Depression and Quality of Life in Functional Dyspepsia PatientsReza Ridho PahleviNo ratings yet
- Depression Predicts Global Functional Outcomes inDocument9 pagesDepression Predicts Global Functional Outcomes inifclarinNo ratings yet
- 2022 The Best Decreasing Prevalence ADHD LifespanDocument4 pages2022 The Best Decreasing Prevalence ADHD LifespanJessica WathierNo ratings yet
- Health Literacy and Ethnic Disparities in Health-Related Quality of Life Among Rural Women: Results From A Chinese Poor Minority AreaDocument9 pagesHealth Literacy and Ethnic Disparities in Health-Related Quality of Life Among Rural Women: Results From A Chinese Poor Minority AreaAndriani SittiNo ratings yet
- Cognitive Functioning in Adolescents With SelfReported ADHD and Depression Results From A Population-Based StudyDocument14 pagesCognitive Functioning in Adolescents With SelfReported ADHD and Depression Results From A Population-Based StudyJesúsCoyacNo ratings yet
- Yoa15011 827 837Document11 pagesYoa15011 827 837Junior BonfáNo ratings yet
- Decision MakingDocument8 pagesDecision Makingroshanak zareiNo ratings yet
- QOL CopingDocument10 pagesQOL CopingNisa PradityaNo ratings yet
- Mental HealthDocument8 pagesMental HealthJohn TelekNo ratings yet
- Full TextDocument10 pagesFull Textammarashor78No ratings yet
- JoHM 03 2018 ADHD KiGGS-Wave2Document8 pagesJoHM 03 2018 ADHD KiGGS-Wave2C ANo ratings yet
- Studyprotocol Open AccessDocument13 pagesStudyprotocol Open AccessGabrielDosAnjosNo ratings yet
- A Randomized Controlled Trial of Group Reality TheDocument6 pagesA Randomized Controlled Trial of Group Reality TheValentina Arias MesaNo ratings yet
- Jurnal DepresiDocument15 pagesJurnal DepresiDesi PratiwiNo ratings yet
- Epidemiology of Apathy in Older Adults. The Cache County StudyDocument11 pagesEpidemiology of Apathy in Older Adults. The Cache County StudyJuanNo ratings yet
- JOURNAL CLUB NewDocument61 pagesJOURNAL CLUB Newaastha panthNo ratings yet
- Diff Erences in Cognitive Function and Daily Living Skills Between Early-And Late-Stage SchizophreniaDocument8 pagesDiff Erences in Cognitive Function and Daily Living Skills Between Early-And Late-Stage SchizophreniaRenny TjahjaNo ratings yet
- Journal DM Pada LansiiaaDocument9 pagesJournal DM Pada Lansiiaaayu maulidaNo ratings yet
- Cognitive TreatmentDocument12 pagesCognitive TreatmentSaul MorenoNo ratings yet
- Compulsive Sexual Behavior in Young AdultsDocument8 pagesCompulsive Sexual Behavior in Young AdultsFestijo , Kenneth100% (1)
- Duration of Untreated Eating Disorder and Relationship To Outcomes, A Systematic Review of The LiteratureDocument17 pagesDuration of Untreated Eating Disorder and Relationship To Outcomes, A Systematic Review of The Literatureobservacionfray23No ratings yet
- Neurobiological Theories of ConsciousnessDocument14 pagesNeurobiological Theories of ConsciousnessRodrigo Aguirre BáezNo ratings yet
- Neurobiological Theories of ConsciousnessDocument14 pagesNeurobiological Theories of ConsciousnessRodrigo Aguirre BáezNo ratings yet
- Prefrontal Contributions To Metacognition in Perceptual Decision MakingDocument9 pagesPrefrontal Contributions To Metacognition in Perceptual Decision MakingRodrigo Aguirre BáezNo ratings yet
- Integrative Systematic Review of Psychodrama Psychotherapy Research Trends and Methodological Implications PDFDocument26 pagesIntegrative Systematic Review of Psychodrama Psychotherapy Research Trends and Methodological Implications PDFRodrigo Aguirre BáezNo ratings yet
- Social Cognitive Neuroscience A Review of Core ProcessesDocument35 pagesSocial Cognitive Neuroscience A Review of Core ProcessesRodrigo Aguirre BáezNo ratings yet
- Knowing Your Own Heart Distinguishing Interoceptive Accuracy From Interoceptive AwarenessDocument10 pagesKnowing Your Own Heart Distinguishing Interoceptive Accuracy From Interoceptive AwarenessRodrigo Aguirre BáezNo ratings yet
- Human Prefrontal Cortex - Processind and Representational PerspectivesDocument9 pagesHuman Prefrontal Cortex - Processind and Representational PerspectivesRodrigo Aguirre BáezNo ratings yet
- C Uestion RioDocument8 pagesC Uestion RioLuisanaMoralesNo ratings yet
- How The Visual Brain Encodes and Keeps Track of TimeDocument8 pagesHow The Visual Brain Encodes and Keeps Track of TimeRodrigo Aguirre BáezNo ratings yet
- Intelectual Test de MatricesDocument26 pagesIntelectual Test de MatricesMauricio PalaciosNo ratings yet
- Depression and Cognitive Impairment in Older Adults: Geriatric Disorders (DC Steffens, Section Editor)Document9 pagesDepression and Cognitive Impairment in Older Adults: Geriatric Disorders (DC Steffens, Section Editor)Rodrigo Aguirre BáezNo ratings yet
- Late-Life Depression, Mild Cognitive Impairment, and DementiaDocument7 pagesLate-Life Depression, Mild Cognitive Impairment, and DementiaRodrigo Aguirre BáezNo ratings yet
- The Patterns of Cognitive and Functional Impairment in Amnestic and Non-Amnestic MCI in Geriatric Depression. ReinliebDocument14 pagesThe Patterns of Cognitive and Functional Impairment in Amnestic and Non-Amnestic MCI in Geriatric Depression. ReinliebRodrigo Aguirre BáezNo ratings yet
- Polifarmacia ActualizacionDocument10 pagesPolifarmacia ActualizacionMiguelySusy Ramos-RojasNo ratings yet
- Screening Performance of The 15-Item Geriatric Depression Scale in A Diverse Elderly Home Care PopulationDocument8 pagesScreening Performance of The 15-Item Geriatric Depression Scale in A Diverse Elderly Home Care PopulationRodrigo Aguirre BáezNo ratings yet
- Integrative Systematic Review of Psychodrama Psychotherapy Research Trends and Methodological Implications PDFDocument26 pagesIntegrative Systematic Review of Psychodrama Psychotherapy Research Trends and Methodological Implications PDFRodrigo Aguirre BáezNo ratings yet
- Liang Kung Chen 2020Document13 pagesLiang Kung Chen 2020Rodrigo Aguirre BáezNo ratings yet
- Greenberg 2007Document10 pagesGreenberg 2007Rodrigo Aguirre BáezNo ratings yet
- Determinants of Cognitive Performance and Decline in 20 Diverse Ethno-Regional Groups: A COSMIC Collaboration Cohort StudyDocument27 pagesDeterminants of Cognitive Performance and Decline in 20 Diverse Ethno-Regional Groups: A COSMIC Collaboration Cohort StudyRodrigo Aguirre BáezNo ratings yet
- Accepted Manuscript: MaturitasDocument18 pagesAccepted Manuscript: MaturitasRodrigo Aguirre BáezNo ratings yet
- Heser 2016Document15 pagesHeser 2016Rodrigo Aguirre BáezNo ratings yet
- Issue 4 PDFDocument2 pagesIssue 4 PDFNa DilanNo ratings yet
- JNEUROSCIENCEDocument40 pagesJNEUROSCIENCERodrigo Aguirre BáezNo ratings yet
- Integrative Systematic Review of Psychodrama Psychotherapy Research Trends and Methodological Implications PDFDocument26 pagesIntegrative Systematic Review of Psychodrama Psychotherapy Research Trends and Methodological Implications PDFRodrigo Aguirre BáezNo ratings yet
- Microstates As Disease and Progression Markers in Patients With Mild Cognitive ImpairmentDocument11 pagesMicrostates As Disease and Progression Markers in Patients With Mild Cognitive ImpairmentRodrigo Aguirre BáezNo ratings yet
- Attachment 8 LAST REVISED 20/04/2018: PHD in Neural and Cognitive Sciences in BriefDocument3 pagesAttachment 8 LAST REVISED 20/04/2018: PHD in Neural and Cognitive Sciences in BriefRodrigo Aguirre BáezNo ratings yet
- Cronicon: Letter To Editor Neuropsychological Impairment in Major Depressive DisorderDocument2 pagesCronicon: Letter To Editor Neuropsychological Impairment in Major Depressive DisorderRodrigo Aguirre BáezNo ratings yet
- JNEUROSCIENCEDocument40 pagesJNEUROSCIENCERodrigo Aguirre BáezNo ratings yet
- Adoçante e Resistência À Insulina - Nature PDFDocument17 pagesAdoçante e Resistência À Insulina - Nature PDFMell FalcãoNo ratings yet
- Medical Examination Certificate: ConfidentialDocument2 pagesMedical Examination Certificate: ConfidentialVioletaNo ratings yet
- Nutritional Prehabilitation Program and Cardiac Surgery Outcome in PediatricsDocument15 pagesNutritional Prehabilitation Program and Cardiac Surgery Outcome in PediatricsIOSRjournalNo ratings yet
- Healthy Breakfast FoodsDocument3 pagesHealthy Breakfast FoodsChenNo ratings yet
- Efficacy and Safety of A Combined Aerobic, Strength and Flexibility Exercise Training Program in Patients With Implantable Cardiac Devices-2022Document10 pagesEfficacy and Safety of A Combined Aerobic, Strength and Flexibility Exercise Training Program in Patients With Implantable Cardiac Devices-2022Josemi Del Castillo MolinaNo ratings yet
- CAS 740 Service Manual - Eng - 21!02!0174 REV000Document110 pagesCAS 740 Service Manual - Eng - 21!02!0174 REV000Serginho HenriqueNo ratings yet
- 2012 Wilderness Basics Course NotebookDocument90 pages2012 Wilderness Basics Course NotebookU8x58No ratings yet
- MCN CH 17Document14 pagesMCN CH 17Kristine KrisNo ratings yet
- Reviewer For Management of Common IllnessDocument27 pagesReviewer For Management of Common Illnessmarie vennis hamchawanNo ratings yet
- International JournalDocument5 pagesInternational JournalPutri Nur HandayaniNo ratings yet
- Community Oriented Primary Care: Meaning and Scope: General ConsiderationsDocument33 pagesCommunity Oriented Primary Care: Meaning and Scope: General ConsiderationsShams JailaniNo ratings yet
- DrugsDocument7 pagesDrugsEloisa Abarintos RacalNo ratings yet
- Virtual Care HFDocument14 pagesVirtual Care HFTom BiusoNo ratings yet
- Normal Vital Signs Guidelines For EmsDocument2 pagesNormal Vital Signs Guidelines For Emsisabelo_laguraNo ratings yet
- Direction: Read The Questions Carefully. Shade The Letter of Your Answer On The Answer SheetDocument6 pagesDirection: Read The Questions Carefully. Shade The Letter of Your Answer On The Answer SheetReizle TinazaNo ratings yet
- مزاولةDocument226 pagesمزاولةyaraikhlayelNo ratings yet
- BP Monitoring Log BookDocument2 pagesBP Monitoring Log Bookroland acacioNo ratings yet
- Recavery After Anasthesia PDFDocument3 pagesRecavery After Anasthesia PDFYudionoNo ratings yet
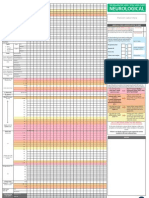
- Adult Early Warning Score Observation Chart For Neurosurgical UnitDocument1 pageAdult Early Warning Score Observation Chart For Neurosurgical UnitalexipsNo ratings yet
- Endocrine Response To Masturbation-Induced Orgasm in Healthy Men Following A 3-Week Sexual AbstinenceDocument6 pagesEndocrine Response To Masturbation-Induced Orgasm in Healthy Men Following A 3-Week Sexual AbstinenceAziz Bin ThaniNo ratings yet
- Cardiovascular Hypertensive Crisis Recent EvidenceDocument6 pagesCardiovascular Hypertensive Crisis Recent Evidenceagustinaw1981No ratings yet
- PeKa B40 Health Screening Form 3 - First Consultation - 201902Document4 pagesPeKa B40 Health Screening Form 3 - First Consultation - 201902Ezanii ShaharuddinNo ratings yet
- Diabetic Neuropathies. 2023Document17 pagesDiabetic Neuropathies. 2023Arbey Aponte PuertoNo ratings yet
- Q2 GPA Blood Vessels IIDocument7 pagesQ2 GPA Blood Vessels IIAdrian CaballesNo ratings yet
- Fresenius Manual 4008B PDFDocument4 pagesFresenius Manual 4008B PDFAlexander Villa100% (1)
- 15 PharmacologyDocument15 pages15 PharmacologySpy HanNo ratings yet
- NCM 103 Rle NotesDocument8 pagesNCM 103 Rle Notesgallardo.bettinarose.iNo ratings yet
- 01 Hyp 1 3 287 PDFDocument5 pages01 Hyp 1 3 287 PDFAndrea ForcinitiNo ratings yet
- HET Digital Thermometer DT-11A & BP Meter MB300ADocument2 pagesHET Digital Thermometer DT-11A & BP Meter MB300AFerdinand EstanislaoNo ratings yet
- Discharge Planning PaperDocument5 pagesDischarge Planning Paperapi-398485408No ratings yet
- Nursing Diagnosis: May Be Related To: Fluid Volume Deficit (Isotonic)Document26 pagesNursing Diagnosis: May Be Related To: Fluid Volume Deficit (Isotonic)Ric Nacional75% (4)