You might also like
- JMRH Volume 4 Issue 2 Pages 592-599Document8 pagesJMRH Volume 4 Issue 2 Pages 592-599Rafidah HelmiNo ratings yet
- Oxytocin IVDocument7 pagesOxytocin IVAnamika LinggaNo ratings yet
- Sciencedirect: Sara Dokuhaki, Maryam Heidary, Marzieh AkbarzadehDocument8 pagesSciencedirect: Sara Dokuhaki, Maryam Heidary, Marzieh AkbarzadehRatrika SariNo ratings yet
- Bersalin IngDocument6 pagesBersalin IngIngca ClaudiaNo ratings yet
- The Effect of Maternal - Fetal Attachment Education On Maternal MenDocument7 pagesThe Effect of Maternal - Fetal Attachment Education On Maternal MenNadia RifeldaNo ratings yet
- Effectiveness of childbirth educationDocument10 pagesEffectiveness of childbirth educationpoongodi cNo ratings yet
- Mindfulness-Based InterventionsDocument17 pagesMindfulness-Based InterventionsdinaaNo ratings yet
- Manuscript UlfaDocument10 pagesManuscript UlfaANDIS SHAFANo ratings yet
- The Effect of Maternal-Fetal Attachment Education On Maternal Mental HealthDocument6 pagesThe Effect of Maternal-Fetal Attachment Education On Maternal Mental HealthrutnomleniNo ratings yet
- The Relationship Between Maternal-Fetal Attachment and Maternal Self-Efficacy in Iranian Women: A Prospective StudyDocument11 pagesThe Relationship Between Maternal-Fetal Attachment and Maternal Self-Efficacy in Iranian Women: A Prospective StudyNadia RifeldaNo ratings yet
- Analisis HypnoDocument5 pagesAnalisis Hypnosalsabila.asyifaNo ratings yet
- Mental HealthDocument7 pagesMental HealthMirjana14No ratings yet
- GHDocument9 pagesGHReginald JuliaNo ratings yet
- The Effects of Baby Massage On AttachmenDocument7 pagesThe Effects of Baby Massage On AttachmenKhurram MalikNo ratings yet
- Jurnal Back MassageDocument9 pagesJurnal Back MassageVikaniikhaNo ratings yet
- The Effect of Baby Massage On Attachment Between Mother and Their InfantsDocument7 pagesThe Effect of Baby Massage On Attachment Between Mother and Their InfantsAnonymous jmc9IzFNo ratings yet
- The Effectiveness of Hypnobirthing in Reducing Anxiety Level During DeliveryDocument8 pagesThe Effectiveness of Hypnobirthing in Reducing Anxiety Level During DeliveryDitha FauziahNo ratings yet
- Background: The Effect of Slow-Stroke Back Massage On The Anxiety Levels of Iranian Women On The First Postpartum DayDocument6 pagesBackground: The Effect of Slow-Stroke Back Massage On The Anxiety Levels of Iranian Women On The First Postpartum DayWidya NingrumNo ratings yet
- Arum Hastuti Dwi Sofiati Jurnal Persalinan B.inggrisDocument5 pagesArum Hastuti Dwi Sofiati Jurnal Persalinan B.inggrisArum HastutiNo ratings yet
- Breastfeeding Self EfficacyDocument18 pagesBreastfeeding Self EfficacyFitri Wahyuni PutriNo ratings yet
- 10 Sreeja GangadharanDocument12 pages10 Sreeja GangadharanSreeja GangaNo ratings yet
- Article - Tired Moody and Pregnant Exercise May Be The AnswerDocument18 pagesArticle - Tired Moody and Pregnant Exercise May Be The AnswerRegina PhalangeNo ratings yet
- Faktor yang Mempengaruhi Lama Kala I PersalinanDocument15 pagesFaktor yang Mempengaruhi Lama Kala I PersalinanEl LyNo ratings yet
- 4 - Educación y GestaciónDocument5 pages4 - Educación y GestaciónSharon Lisbeth Ovalle MazoNo ratings yet
- Effectiveness of Yoga Video Assisted Teaching Among Antenatal MothersDocument4 pagesEffectiveness of Yoga Video Assisted Teaching Among Antenatal MothersSelvin Tody LantiungaNo ratings yet
- Efektivitas SnoezelenDocument8 pagesEfektivitas SnoezelenFahmi RizqiNo ratings yet
- Validation of A Short Form Three Facet Mindfulness Questionnaire (TFMQ-SF) in Pregnant Women.Document7 pagesValidation of A Short Form Three Facet Mindfulness Questionnaire (TFMQ-SF) in Pregnant Women.Gabriella DivaNo ratings yet
- Synth Final2Document10 pagesSynth Final2api-679675055No ratings yet
- 10 53424-Balikesirsbd 1029908-2104936Document8 pages10 53424-Balikesirsbd 1029908-2104936obenimNo ratings yet
- Annotated Bibliography For Postartum DepressionDocument7 pagesAnnotated Bibliography For Postartum Depressionjeremiah tawandaNo ratings yet
- Waldenstrom 2004Document11 pagesWaldenstrom 2004andrea azevedoNo ratings yet
- Jurnal 3Document7 pagesJurnal 3Richa FarellaNo ratings yet
- Chou 2008Document7 pagesChou 2008Jaydwin LabianoNo ratings yet
- Fear of Childbirth: Mothers' Experiences of Team-Midwifery Care - A Follow-Up StudyDocument8 pagesFear of Childbirth: Mothers' Experiences of Team-Midwifery Care - A Follow-Up Studyyayusuk desamtaNo ratings yet
- Clinical StudyDocument8 pagesClinical StudyFatimatus ZahroNo ratings yet
- Prevalence and Determinants of Postpartum Depression in Sukoharjo District, Central JavaDocument14 pagesPrevalence and Determinants of Postpartum Depression in Sukoharjo District, Central Javasuci triana putriNo ratings yet
- IJN - Volume 9 - Issue 3 - Pages 26-34 PDFDocument9 pagesIJN - Volume 9 - Issue 3 - Pages 26-34 PDFSyarifah Rahmawati30No ratings yet
- IJN - Volume 9 - Issue 3 - Pages 26-34Document9 pagesIJN - Volume 9 - Issue 3 - Pages 26-34Syarifah Rahmawati30No ratings yet
- Sharkey 2015Document10 pagesSharkey 2015Juanda RaynaldiNo ratings yet
- Effect of Yoga On Duration of The Second Stage of Labor and Perineal Rupture in Primigravida MothersDocument5 pagesEffect of Yoga On Duration of The Second Stage of Labor and Perineal Rupture in Primigravida MothersDellaTaurusNo ratings yet
- 1799 7257 1 PBDocument15 pages1799 7257 1 PBIne RenggoNo ratings yet
- Review of Literature MAILDocument12 pagesReview of Literature MAILShebin Shebi EramangalathNo ratings yet
- Boyea Walter FinalproposalDocument13 pagesBoyea Walter Finalproposalapi-346484816No ratings yet
- Running Head: Depression Screening 1Document26 pagesRunning Head: Depression Screening 1api-456313554No ratings yet
- Ijcmr 1247 Feb 29 PDFDocument4 pagesIjcmr 1247 Feb 29 PDFabdullah khalidNo ratings yet
- Kecemasan Ibu HamilDocument10 pagesKecemasan Ibu HamilRobby RNo ratings yet
- Positive Negative Affect and Teen Pregnancy: Afek Positif Negatif Dan Kehamilan RemajaDocument6 pagesPositive Negative Affect and Teen Pregnancy: Afek Positif Negatif Dan Kehamilan RemajaYoung JaeNo ratings yet
- Teen Pregnancy Affect and DemographicsDocument6 pagesTeen Pregnancy Affect and DemographicsYoung JaeNo ratings yet
- Non-Pharmaceutical Labor Pain Relief and Postpartum DepressionDocument9 pagesNon-Pharmaceutical Labor Pain Relief and Postpartum DepressionDesi PratiwiNo ratings yet
- Effect of Music On Immediately Postpartum Lactation by Term Mothers After Giving Birth: A Randomized Controlled TrialDocument9 pagesEffect of Music On Immediately Postpartum Lactation by Term Mothers After Giving Birth: A Randomized Controlled TrialMari FeNo ratings yet
- Bimbingan RohaniDocument7 pagesBimbingan RohaniPhyan HyunNo ratings yet
- Factors Influencing Contraceptive Uptake Among Lactating Mothers (6-24 Months) - A Case Study of 2medical Reception Station (2MRS)Document7 pagesFactors Influencing Contraceptive Uptake Among Lactating Mothers (6-24 Months) - A Case Study of 2medical Reception Station (2MRS)NanaKarikariMintahNo ratings yet
- A Review of The Effects of Anxiety During Pregnancy On Children's HealthDocument3 pagesA Review of The Effects of Anxiety During Pregnancy On Children's HealthChandra Dwi FitrianiNo ratings yet
- The Effects of Infant Massage On Weight, PDFDocument9 pagesThe Effects of Infant Massage On Weight, PDFFebryLasantiNo ratings yet
- Pregnancy-Related Anxiety, Perceived Parental Self-E: Fficacy and The Influence of Parity and AgeDocument17 pagesPregnancy-Related Anxiety, Perceived Parental Self-E: Fficacy and The Influence of Parity and AgedyahNo ratings yet
- KJWHN 2022 12 16 PDFDocument10 pagesKJWHN 2022 12 16 PDFDede AddinulNo ratings yet
- Pengaruh Peran Suami Terhadap Tingkat Kecemasan Ibu Hamil Dalam Menghadapi Proses Persalinan Di Puskesmas Harapan Raya PekanbaruDocument13 pagesPengaruh Peran Suami Terhadap Tingkat Kecemasan Ibu Hamil Dalam Menghadapi Proses Persalinan Di Puskesmas Harapan Raya PekanbaruNovrida YantiNo ratings yet
- Prenatal Psychosocial DisordersDocument18 pagesPrenatal Psychosocial DisordersHari Putra PetirNo ratings yet
- First-time Mothers' Social Support, Self-Efficacy and Postnatal DepressionDocument10 pagesFirst-time Mothers' Social Support, Self-Efficacy and Postnatal Depressionmotanul2No ratings yet
- Psychopharmacology and Pregnancy: Treatment Efficacy, Risks, and GuidelinesFrom EverandPsychopharmacology and Pregnancy: Treatment Efficacy, Risks, and GuidelinesNo ratings yet
- D3kepma2a - Zumrotul Alfiyah Wardani - P17210181030Document15 pagesD3kepma2a - Zumrotul Alfiyah Wardani - P17210181030mufid dodyNo ratings yet
- Complementary Therapies in Clinical PracticeDocument17 pagesComplementary Therapies in Clinical Practicemufid dodyNo ratings yet
- D3 Kepma 2a - Sony Irawan - P17210181006Document15 pagesD3 Kepma 2a - Sony Irawan - P17210181006mufid dodyNo ratings yet
- D3kepma2a - Adela Tri Kurniawati - P17210183063Document13 pagesD3kepma2a - Adela Tri Kurniawati - P17210183063mufid dodyNo ratings yet
- D3kepma2a - Maudy Mila Fadhila - P17210181029Document11 pagesD3kepma2a - Maudy Mila Fadhila - P17210181029mufid dodyNo ratings yet
- D3kepma2a - Nurmaya Apriliani S - P17210181011Document7 pagesD3kepma2a - Nurmaya Apriliani S - P17210181011mufid dodyNo ratings yet
- D3kepma2a - Reza Fani Bachtiar - P17210181018Document8 pagesD3kepma2a - Reza Fani Bachtiar - P17210181018mufid dodyNo ratings yet
- D3kepma2a - Dewi Yuli Astutik - P17210181022Document19 pagesD3kepma2a - Dewi Yuli Astutik - P17210181022mufid dodyNo ratings yet
- Individu: D3 Kepma 2A - Rahmita Mulia Putri - P17210183064 Pair: D3Kepma2A - Rahmita Mulia Putri and D3Kepma2A - Dini HAIRUN - P17210181005Document5 pagesIndividu: D3 Kepma 2A - Rahmita Mulia Putri - P17210183064 Pair: D3Kepma2A - Rahmita Mulia Putri and D3Kepma2A - Dini HAIRUN - P17210181005mufid dodyNo ratings yet
- D3kepma2a - Putri Winda Nathaniella - P17210183047Document13 pagesD3kepma2a - Putri Winda Nathaniella - P17210183047mufid dodyNo ratings yet
- D3kepma2a - Tika Dwi Aprilliani - P17210182044Document17 pagesD3kepma2a - Tika Dwi Aprilliani - P17210182044mufid dodyNo ratings yet
- Guided Imagery Mental Stress Management: Task 1 (Artikel)Document7 pagesGuided Imagery Mental Stress Management: Task 1 (Artikel)mufid dodyNo ratings yet
- D3kepma2a - Fristy Nur Amalia Floranti - P17210181010Document7 pagesD3kepma2a - Fristy Nur Amalia Floranti - P17210181010mufid dodyNo ratings yet
- Penugasan Bahasa Inggris Untuk Memenuhi Tugas Matakuliah Bahasa Inggris Yang Dibina Oleh Ibu Eka Wulandari, S.PD., M.PDDocument14 pagesPenugasan Bahasa Inggris Untuk Memenuhi Tugas Matakuliah Bahasa Inggris Yang Dibina Oleh Ibu Eka Wulandari, S.PD., M.PDmufid dodyNo ratings yet
- D3 Kepma2a Acik Febila Antika P17210183067Document7 pagesD3 Kepma2a Acik Febila Antika P17210183067mufid dodyNo ratings yet
- D3 Kepma 2a - Yunita Kusma Hardianti - P17210183058Document10 pagesD3 Kepma 2a - Yunita Kusma Hardianti - P17210183058mufid dodyNo ratings yet
- Individu: D3 Kepma 2A - Rahmita Mulia Putri - P17210183064 Pair: D3Kepma2A - Rahmita Mulia Putri and D3Kepma2A - Dini HAIRUN - P17210181005Document5 pagesIndividu: D3 Kepma 2A - Rahmita Mulia Putri - P17210183064 Pair: D3Kepma2A - Rahmita Mulia Putri and D3Kepma2A - Dini HAIRUN - P17210181005mufid dodyNo ratings yet
- D3 Kepma 2a - Dossy Chlismala - P17210183053Document10 pagesD3 Kepma 2a - Dossy Chlismala - P17210183053mufid dodyNo ratings yet
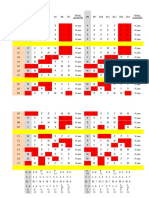
- MAN KEP Kel 2 Bu Tri (FIKS NEMEN!!) - MARI REVISI (JADWAL SEBULAN)Document6 pagesMAN KEP Kel 2 Bu Tri (FIKS NEMEN!!) - MARI REVISI (JADWAL SEBULAN)mufid dodyNo ratings yet
- D3kepma2a - Putri Winda Nathaniella - P17210183047Document13 pagesD3kepma2a - Putri Winda Nathaniella - P17210183047mufid dodyNo ratings yet
- D3kepma2a - Naulya Hapzoh A.P - P17210181002Document5 pagesD3kepma2a - Naulya Hapzoh A.P - P17210181002mufid dodyNo ratings yet
- D3kepma2a - Lailatus S - P17210181019Document16 pagesD3kepma2a - Lailatus S - P17210181019mufid dodyNo ratings yet
- D3kepma2a - Tika Dwi Aprilliani - P17210182044Document17 pagesD3kepma2a - Tika Dwi Aprilliani - P17210182044mufid dodyNo ratings yet
- Guided Imagery Mental Stress Management: Task 1 (Artikel)Document7 pagesGuided Imagery Mental Stress Management: Task 1 (Artikel)mufid dodyNo ratings yet
- D3kepma2a - Hanisa Iis Ariska - P17210182035Document8 pagesD3kepma2a - Hanisa Iis Ariska - P17210182035mufid dodyNo ratings yet
- D3kepma2a - Nia Cantika Pasaribu - P17210181020Document6 pagesD3kepma2a - Nia Cantika Pasaribu - P17210181020mufid dodyNo ratings yet
- Complementary Therapies in Clinical PracticeDocument17 pagesComplementary Therapies in Clinical Practicemufid dodyNo ratings yet
- D3kepma2a - Mia Mardiana P - P17210182046Document10 pagesD3kepma2a - Mia Mardiana P - P17210182046mufid dodyNo ratings yet
- Guided Imagery Reduces Anxiety in Cancer PatientDocument7 pagesGuided Imagery Reduces Anxiety in Cancer Patientmufid dodyNo ratings yet
- Maternal QuizDocument3 pagesMaternal QuizJeffrey ViernesNo ratings yet
- 2 Periodical Test in Mapeh-8Document38 pages2 Periodical Test in Mapeh-8Byron DizonNo ratings yet
- Preparing For A Glucose Tolerance TestDocument3 pagesPreparing For A Glucose Tolerance Testconnect.rohit85No ratings yet
- Herbs To Avoid During Pregnancy PDFDocument7 pagesHerbs To Avoid During Pregnancy PDFJNo ratings yet
- Acute Bacterial Meningitis During and After Pregnancy: CommentaryDocument3 pagesAcute Bacterial Meningitis During and After Pregnancy: CommentaryAyu Wedhani SpcNo ratings yet
- APGODocument49 pagesAPGOiamdonutNo ratings yet
- Maternity Benefit ActDocument29 pagesMaternity Benefit ActShivone DiasNo ratings yet
- CPR in Pregnancy 2Document3 pagesCPR in Pregnancy 2Fatmasari Perdana MenurNo ratings yet
- Berkah HidupDocument7 pagesBerkah HidupLaskar JuangNo ratings yet
- Seminar On AphDocument46 pagesSeminar On AphKaruna KumariNo ratings yet
- Right to Safe Abortion as a Human RightDocument15 pagesRight to Safe Abortion as a Human RightJirehPorciuncula0% (1)
- Psychiatric History Taking EssentialsDocument108 pagesPsychiatric History Taking Essentialsdev86% (37)
- AAP-Anaemia - Clinical Report-Diagnosis and Prevention of IronDocument13 pagesAAP-Anaemia - Clinical Report-Diagnosis and Prevention of Irondesai2kNo ratings yet
- Antenatal Care: Dr. Dr. I Nyoman Bayu Mahendra, Spog (K)Document38 pagesAntenatal Care: Dr. Dr. I Nyoman Bayu Mahendra, Spog (K)Anresangsya YasaNo ratings yet
- Mco 1500.52DDocument25 pagesMco 1500.52DtarunNo ratings yet
- Obstetrics Anjali Mam Pattern For Vaginal DeliveryDocument12 pagesObstetrics Anjali Mam Pattern For Vaginal DeliveryBibek PandeyNo ratings yet
- Acog Parto Vaginal QX PDFDocument11 pagesAcog Parto Vaginal QX PDFAnghelino Jesus Meza CentenoNo ratings yet
- CBTP Research PaperDocument67 pagesCBTP Research PaperEskindir Solomon100% (1)
- Baby SuppliesDocument124 pagesBaby SuppliesWell-Being per diemNo ratings yet
- Literature Review On Legalization of AbortionDocument6 pagesLiterature Review On Legalization of Abortiontkpmzasif100% (1)
- Jurnal Case Cohort Studies 2Document6 pagesJurnal Case Cohort Studies 2Dee SariNo ratings yet
- PQ 168 MMR MSD Pi July2008Document7 pagesPQ 168 MMR MSD Pi July2008Charles AnthonyNo ratings yet
- Name: Demayo, Edson John C. Year & Section: BSN - 3A: Date: MARCH 16, 2021Document10 pagesName: Demayo, Edson John C. Year & Section: BSN - 3A: Date: MARCH 16, 2021Edson John DemayoNo ratings yet
- 2019 Canadian Guideline For Physical Activity Throughout PregnancyDocument8 pages2019 Canadian Guideline For Physical Activity Throughout PregnancynirchennNo ratings yet
- Perry: Maternal Child Nursing Care, 6th Edition: Chapter 08: Nursing Care of The Family During Pregnancy Key PointsDocument2 pagesPerry: Maternal Child Nursing Care, 6th Edition: Chapter 08: Nursing Care of The Family During Pregnancy Key PointsNicole HumesNo ratings yet
- Gestational Diabetes Mellitus ReadingDocument4 pagesGestational Diabetes Mellitus ReadingHecia Gaga-aNo ratings yet
- Clinics in ObstetricsDocument770 pagesClinics in ObstetricsSAKAI69100% (3)
- Topic 1 - Introduction To Nutrition in The Life Stages 1Document7 pagesTopic 1 - Introduction To Nutrition in The Life Stages 1Aliyashir IbrahimNo ratings yet
- Care of Mother and Child at RiskDocument5 pagesCare of Mother and Child at RisknianNo ratings yet
- ICM - 2019 Essential Competencies For Midwifery PracticeDocument22 pagesICM - 2019 Essential Competencies For Midwifery Practicedyah triwidiyantari100% (4)