You might also like
- Daish 2018Document18 pagesDaish 2018dwi vaniNo ratings yet
- Prática Baseada em Evidências em ForçaDocument5 pagesPrática Baseada em Evidências em ForçaRenata SouzaNo ratings yet
- 1 s2.0 S138824571500231X MainDocument8 pages1 s2.0 S138824571500231X MainTianyi ZhengNo ratings yet
- Longlo 2021Document1 pageLonglo 2021Alonso Rodriguez EscobedoNo ratings yet
- Editorial Stress-Only Myocardial Perfusion Imaging It IS Time For A Change!Document4 pagesEditorial Stress-Only Myocardial Perfusion Imaging It IS Time For A Change!Ala PavlovNo ratings yet
- 30184-Article Text-33849-1-10-20050609Document5 pages30184-Article Text-33849-1-10-20050609Gustavo Pezzodipane PicalloNo ratings yet
- A Clinical Practice Guideline For The Use of Ankle-Foot Orthoses and Functional Electrical Stimulation Post-StrokeDocument85 pagesA Clinical Practice Guideline For The Use of Ankle-Foot Orthoses and Functional Electrical Stimulation Post-Strokecamila hernandezNo ratings yet
- High-Energy Versus Low-Energy Extracorporeal Shock Wave Therapy For Calcifying Tendinitis of The Shoulder: Which Is Superior? A Meta-AnalysisDocument10 pagesHigh-Energy Versus Low-Energy Extracorporeal Shock Wave Therapy For Calcifying Tendinitis of The Shoulder: Which Is Superior? A Meta-Analysisginamilena90No ratings yet
- Therapeutic EffectsofWhole-BodyDevices Applying Pulsed Electromagnetic Fields (PEMF)Document11 pagesTherapeutic EffectsofWhole-BodyDevices Applying Pulsed Electromagnetic Fields (PEMF)Jeroan MonteiroNo ratings yet
- A Clinical Practice Guideline For The Use Of.6Document85 pagesA Clinical Practice Guideline For The Use Of.6LEONARDO ALEX CORROTEANo ratings yet
- cellular and molecular mechanisms of action of tDCSDocument13 pagescellular and molecular mechanisms of action of tDCSlabsoneducationNo ratings yet
- Langevin Jacm 2015Document16 pagesLangevin Jacm 2015Romina DatuNo ratings yet
- Effects of Different Electrical Stimulation Currents and Phase Durations On Submaximal and Maximum TorqueDocument8 pagesEffects of Different Electrical Stimulation Currents and Phase Durations On Submaximal and Maximum TorqueMarcoNo ratings yet
- Depression and Electroconvulsive Therapy: Review of Current Anesthesia ConsiderationsDocument3 pagesDepression and Electroconvulsive Therapy: Review of Current Anesthesia ConsiderationsDwi wahyuniNo ratings yet
- Brief Comment and Review of Electroacupuncture Promotes Neuroplasticity of Central Auditory Pathway An Auditory Evoked Potentials StudyDocument3 pagesBrief Comment and Review of Electroacupuncture Promotes Neuroplasticity of Central Auditory Pathway An Auditory Evoked Potentials StudyHerald Scholarly Open AccessNo ratings yet
- Rainarli 2017 J. Phys. Conf. Ser. 824 012029Document9 pagesRainarli 2017 J. Phys. Conf. Ser. 824 012029Ednawati RainarliNo ratings yet
- The Clinical Alliance and Research in ElectroconvuDocument8 pagesThe Clinical Alliance and Research in Electroconvulydia_gayuboNo ratings yet
- TMP 3 F02Document12 pagesTMP 3 F02FrontiersNo ratings yet
- Ketofol (Mixture of Ketamine and Propofol) Administration inDocument7 pagesKetofol (Mixture of Ketamine and Propofol) Administration inM.No ratings yet
- Efficacy of Dexamethasone in Reducing The Postemobolisation Syndrome in Men Undergoing Prostatic Artery Embolisation For Benign Prostatic HyperplasiaDocument6 pagesEfficacy of Dexamethasone in Reducing The Postemobolisation Syndrome in Men Undergoing Prostatic Artery Embolisation For Benign Prostatic HyperplasiaClaudia FreyonaNo ratings yet
- BF066 TechnolRev1972Document7 pagesBF066 TechnolRev1972emeo145No ratings yet
- Cranial Electrotherapy Stimulation and TDocument8 pagesCranial Electrotherapy Stimulation and TMarcel J. SiemeNo ratings yet
- Recent Advances in Clinical Electroencephalography.134Document7 pagesRecent Advances in Clinical Electroencephalography.134yuly.gomezNo ratings yet
- Comparison of Femtosecond Laser Assisted Cataract.Document11 pagesComparison of Femtosecond Laser Assisted Cataract.Danty IndriastutyNo ratings yet
- Status of Activator Methods Chiropractic PDFDocument20 pagesStatus of Activator Methods Chiropractic PDFWanniely KussNo ratings yet
- E076538 FullDocument6 pagesE076538 FullFERNANDO ALVESNo ratings yet
- Jamie Walsh (2023)Document11 pagesJamie Walsh (2023)Елена КарпинскаяNo ratings yet
- A Systematic ReviewDocument17 pagesA Systematic Reviewjorgequintero927470No ratings yet
- Prigatano 1987Document11 pagesPrigatano 1987andromeda.godoyNo ratings yet
- Agentes ElectrofisicosDocument10 pagesAgentes Electrofisicososcar eduardo mateus ariasNo ratings yet
- Reuse Cateter SafeDocument2 pagesReuse Cateter Safegadhang dewanggaNo ratings yet
- Reviews: Brain Stimulation in Psychiatry and Its Effects On CognitionDocument10 pagesReviews: Brain Stimulation in Psychiatry and Its Effects On CognitionPeng KwanNo ratings yet
- Pap Athanasiou 2014Document48 pagesPap Athanasiou 2014Caio LeônidasNo ratings yet
- Comparison of Transcutaneous Electrical Tibial Nervestimulation for the Treatment of Overactive Bladder-A Multi-Arm Randomized Controlled Trial With BlindedassessmentDocument6 pagesComparison of Transcutaneous Electrical Tibial Nervestimulation for the Treatment of Overactive Bladder-A Multi-Arm Randomized Controlled Trial With BlindedassessmentMUHAMMMAD FAKHRINo ratings yet
- HORVATH Transcranial Direct Current Stimulation Five Important Issues We Aren't DiscussingDocument8 pagesHORVATH Transcranial Direct Current Stimulation Five Important Issues We Aren't Discussingexcelencia5No ratings yet
- Jornal 1Document8 pagesJornal 1kedawNo ratings yet
- Alagapan_JNeuralEng_2019Document13 pagesAlagapan_JNeuralEng_2019oswalt.dnNo ratings yet
- Rehabilitation of Ataxic Gait Following Cerebellar LesionsDocument9 pagesRehabilitation of Ataxic Gait Following Cerebellar LesionsresidenciailianatulaNo ratings yet
- Anaesthesia - 2021 - McLeod - Novel Approaches To Needle Tracking and Visualisation PDFDocument11 pagesAnaesthesia - 2021 - McLeod - Novel Approaches To Needle Tracking and Visualisation PDFeralp cevikkalpNo ratings yet
- Anestesia de Neuoreixo ModernaDocument22 pagesAnestesia de Neuoreixo ModernaRetina MaranhaoNo ratings yet
- Pulsed EMF (PEMF) - Physiological Response and Its Potential in Trauma TreatmentDocument23 pagesPulsed EMF (PEMF) - Physiological Response and Its Potential in Trauma TreatmentSY LodhiNo ratings yet
- (2001) Burke D. Excitability of Human AxonsDocument11 pages(2001) Burke D. Excitability of Human AxonsLucía del ValleNo ratings yet
- Horvath Et Al., 2010 (58446)Document7 pagesHorvath Et Al., 2010 (58446)Di V.No ratings yet
- Reply From The Authors - Bja - 31Document2 pagesReply From The Authors - Bja - 31RENAULTNo ratings yet
- TMP 1 CE2Document2 pagesTMP 1 CE2FrontiersNo ratings yet
- Substrate Mapping For Ventricular Tachycardia Assumptions and MisconceptionsDocument12 pagesSubstrate Mapping For Ventricular Tachycardia Assumptions and MisconceptionsTanah PantaiNo ratings yet
- Ictal Theta Power As An Electroconvulsive Therapy.6Document7 pagesIctal Theta Power As An Electroconvulsive Therapy.6helalNo ratings yet
- 20151000_0-00034Document24 pages20151000_0-00034eldem02kNo ratings yet
- 1 s2.0 S1935861X21000590 MainDocument18 pages1 s2.0 S1935861X21000590 MainGerové InvestmentsNo ratings yet
- Journal of Theoretical BiologyDocument12 pagesJournal of Theoretical BiologyFrontiersNo ratings yet
- Marchant Et Al 2014 How Electroencephalography Serves The AnesthesiologistDocument11 pagesMarchant Et Al 2014 How Electroencephalography Serves The AnesthesiologistАлександр ИвановNo ratings yet
- JournalDocument9 pagesJournalfkia2013No ratings yet
- What Is "Evidence-Based" Strength and Conditioning?Document7 pagesWhat Is "Evidence-Based" Strength and Conditioning?ok okNo ratings yet
- Wright 2012Document9 pagesWright 2012Carolina BorchesNo ratings yet
- Acupuncture For Chronic PainDocument10 pagesAcupuncture For Chronic PaindanielNo ratings yet
- Electrical Stimulation of Abdominal Muscles To Produce Cough in Spinal Cord Injury: Effect of Stimulus IntensityDocument8 pagesElectrical Stimulation of Abdominal Muscles To Produce Cough in Spinal Cord Injury: Effect of Stimulus IntensityyigoNo ratings yet
- Patient-Controlled Epidural Analgesia For Labor.: International Anesthesiology Clinics February 2007Document9 pagesPatient-Controlled Epidural Analgesia For Labor.: International Anesthesiology Clinics February 2007k3 rschNo ratings yet
- Unified EEG Terminology and Criteria For Nonconvulsive Status EpilepticusDocument2 pagesUnified EEG Terminology and Criteria For Nonconvulsive Status EpilepticusjerejerejereNo ratings yet
- Response To "Incorrect Methodology May Favor Ultrasound-Guided Needling Over Shock Wave Treatment in Calcific Tendinopathy of The Shoulder"Document2 pagesResponse To "Incorrect Methodology May Favor Ultrasound-Guided Needling Over Shock Wave Treatment in Calcific Tendinopathy of The Shoulder"ginamilena90No ratings yet
- Manual of Vibration Exercise and Vibration TherapyFrom EverandManual of Vibration Exercise and Vibration TherapyJörn RittwegerNo ratings yet
- SD Post TraumaticosDocument8 pagesSD Post TraumaticosleoNo ratings yet
- p050494 PDFDocument5 pagesp050494 PDFleoNo ratings yet
- Cabot2012 PDFDocument7 pagesCabot2012 PDFleoNo ratings yet
- Cabot2012 PDFDocument7 pagesCabot2012 PDFleoNo ratings yet
- Atomic Structure QuestionsDocument1 pageAtomic Structure QuestionsJames MungallNo ratings yet
- FacebookH Cking 1 3 (SFILEDocument10 pagesFacebookH Cking 1 3 (SFILEFitra AkbarNo ratings yet
- Red Lion Edict-97 - Manual PDFDocument282 pagesRed Lion Edict-97 - Manual PDFnaminalatrukNo ratings yet
- European Journal of Internal MedicineDocument4 pagesEuropean Journal of Internal Medicinesamer battatNo ratings yet
- DataSheet IMA18-10BE1ZC0K 6041793 enDocument8 pagesDataSheet IMA18-10BE1ZC0K 6041793 enRuben Hernandez TrejoNo ratings yet
- Malabsorption and Elimination DisordersDocument120 pagesMalabsorption and Elimination DisordersBeBs jai SelasorNo ratings yet
- VDR G4 Manual Steinsohn PDFDocument185 pagesVDR G4 Manual Steinsohn PDFVariya Dharmesh100% (1)
- Rustom Shams PDFDocument48 pagesRustom Shams PDFmtaha85No ratings yet
- Frequently Asked Questions About Ailunce HD1: Where Can Find HD1 Software & Firmware?Document5 pagesFrequently Asked Questions About Ailunce HD1: Where Can Find HD1 Software & Firmware?Eric Contra Color0% (1)
- Setup LogDocument77 pagesSetup Loganon-261766No ratings yet
- Hotel Engineering Facilities: A Case Study of Maintenance PerformanceDocument7 pagesHotel Engineering Facilities: A Case Study of Maintenance PerformanceHoh Pui KeiNo ratings yet
- Inner Unit EstimateDocument35 pagesInner Unit EstimateMir MoNo ratings yet
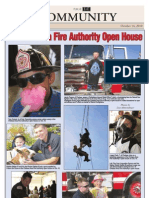
- CAFA Open House HighlightsDocument1 pageCAFA Open House HighlightsDaniel LaiNo ratings yet
- Hunk 150Document2 pagesHunk 150Brayan Torres04No ratings yet
- Mla 8 Mla Citation PageDocument4 pagesMla 8 Mla Citation Pageapi-458274061No ratings yet
- Kidney, bladder & prostate pathology slides explainedDocument20 pagesKidney, bladder & prostate pathology slides explainedNisrina Nur AzisahNo ratings yet
- BOOK-Deva-Oracle MaterialDocument177 pagesBOOK-Deva-Oracle MaterialPAVANN TNo ratings yet
- Ventilator Modes - WEANINGDocument3 pagesVentilator Modes - WEANINGAlaa OmarNo ratings yet
- Cheat Codes SkyrimDocument13 pagesCheat Codes SkyrimDerry RahmaNo ratings yet
- 2 Integrated MarketingDocument13 pages2 Integrated MarketingPaula Marin CrespoNo ratings yet
- 2020.07.31 Marchese Declaration With ExhibitsDocument103 pages2020.07.31 Marchese Declaration With Exhibitsheather valenzuelaNo ratings yet
- The Beggar's Opera by Gay, John, 1685-1732Document50 pagesThe Beggar's Opera by Gay, John, 1685-1732Gutenberg.orgNo ratings yet
- Altered Ventilatory Function Assessment at Pamantasan ng CabuyaoDocument27 pagesAltered Ventilatory Function Assessment at Pamantasan ng Cabuyaomirai desuNo ratings yet
- DOJ OIG Issues 'Fast and Furious' ReportDocument512 pagesDOJ OIG Issues 'Fast and Furious' ReportFoxNewsInsiderNo ratings yet
- Clock Al Ghadeer Setup GuideDocument4 pagesClock Al Ghadeer Setup Guideakberbinshowkat100% (2)
- ASIA IVALUE Business ProfileDocument9 pagesASIA IVALUE Business ProfileDidiek PriambudiNo ratings yet
- COR2-03 Admist The Mists and Coldest Frost PDFDocument16 pagesCOR2-03 Admist The Mists and Coldest Frost PDFLouis BachNo ratings yet
- Manual PDFDocument9 pagesManual PDFRuth ResuelloNo ratings yet
- Unit 2 Water Treatment Ce3303Document18 pagesUnit 2 Water Treatment Ce3303shivaNo ratings yet
- MMME 21 1st Long Exam Lecture NotesDocument74 pagesMMME 21 1st Long Exam Lecture NotesGraver lumiousNo ratings yet