You might also like
- Ashton Manual English PDFDocument58 pagesAshton Manual English PDFMalissa Bowen100% (2)
- Anatomy of The Coronary Arteries and VeinsDocument80 pagesAnatomy of The Coronary Arteries and Veinstreelife111No ratings yet
- Regional Nerve Blocks And Infiltration Therapy: Textbook and Color AtlasFrom EverandRegional Nerve Blocks And Infiltration Therapy: Textbook and Color AtlasDanilo JankovicNo ratings yet
- Comparison of Two Approaches ofDocument96 pagesComparison of Two Approaches ofJacob OrtizNo ratings yet
- Brain Calipers 2Document200 pagesBrain Calipers 2Patricio LopezNo ratings yet
- Atrial Septal Defect (ASD)Document35 pagesAtrial Septal Defect (ASD)Nur Arifah Astri100% (2)
- HVAC Design Manual For Hospitals & Clinics-2003 OrignalDocument6 pagesHVAC Design Manual For Hospitals & Clinics-2003 OrignalAlaa FaiqNo ratings yet
- Blood Transfusion Protocols in NeonatesDocument12 pagesBlood Transfusion Protocols in NeonatesSupriya M A SuppiNo ratings yet
- Unit Plan B.SC ComlpeteDocument148 pagesUnit Plan B.SC ComlpeteSunil Patel100% (1)
- New Clinical Rotation Balaji 2016 2017Document22 pagesNew Clinical Rotation Balaji 2016 2017rama joy100% (1)
- Erector Spinae Plane BlockDocument7 pagesErector Spinae Plane BlockyohannesNo ratings yet
- The Erector Spinae Plane Block: A Review of Current EvidenceDocument11 pagesThe Erector Spinae Plane Block: A Review of Current Evidencetnim.dsNo ratings yet
- 4 IndianJAnaesth617581-2226112 - 061101Document6 pages4 IndianJAnaesth617581-2226112 - 061101Mythology KingdomNo ratings yet
- 1 s2.0 S0007091223007377 MainDocument13 pages1 s2.0 S0007091223007377 MainDAMIAN MERCADO BENTNo ratings yet
- Peripheral Regional Anaesthesia and Outcome: Lessons Learned From The Last 10 YearsDocument14 pagesPeripheral Regional Anaesthesia and Outcome: Lessons Learned From The Last 10 YearsPrisky ChriselawatiNo ratings yet
- Bloqueosy AnatomiaDocument13 pagesBloqueosy AnatomiaRomielyBlancoRandNo ratings yet
- Koksal 2017Document1 pageKoksal 2017PaulHerreraNo ratings yet
- Adductor Canal Block Versus Femoral Canal Block For Total Knee Arthroplasty - A Meta-Analysis 3Document7 pagesAdductor Canal Block Versus Femoral Canal Block For Total Knee Arthroplasty - A Meta-Analysis 3angelama1783riosNo ratings yet
- Ultrasound-Guided Brachial Plexus BlockDocument7 pagesUltrasound-Guided Brachial Plexus BlockÇağdaş BaytarNo ratings yet
- The Evolution of Transcatheter Aortic Valve ReplacDocument2 pagesThe Evolution of Transcatheter Aortic Valve ReplacNicole TorresNo ratings yet
- Ija 64 49Document6 pagesIja 64 49rafiaNo ratings yet
- Ultrasound Reduces The Minimum Effective Local AnaDocument1 pageUltrasound Reduces The Minimum Effective Local AnaRENAULTNo ratings yet
- Review Article Intrathecal Drug Spread: G. Hocking and J. A. W. WildsmithDocument11 pagesReview Article Intrathecal Drug Spread: G. Hocking and J. A. W. WildsmithHalim SudonoNo ratings yet
- Transversus Abdominis Plane Block For Laparoscopic SurgeryDocument2 pagesTransversus Abdominis Plane Block For Laparoscopic SurgeryFitri Kasmita SariNo ratings yet
- Anaesthesia - 2021 - McLeod - Novel Approaches To Needle Tracking and Visualisation PDFDocument11 pagesAnaesthesia - 2021 - McLeod - Novel Approaches To Needle Tracking and Visualisation PDFeralp cevikkalpNo ratings yet
- Feedback CeaDocument1 pageFeedback CeaMahmood HamidiNo ratings yet
- Comparison Between Racemic Bupivacaine and Levobupivacaine Both Combined With Low Dose Fentanyl, Through Intrathecal Route For Transurethral Resection of ProstateDocument4 pagesComparison Between Racemic Bupivacaine and Levobupivacaine Both Combined With Low Dose Fentanyl, Through Intrathecal Route For Transurethral Resection of ProstateInternational Journal of Clinical and Biomedical Research (IJCBR)No ratings yet
- My Published Paper 6, AnesthesiaDocument5 pagesMy Published Paper 6, Anesthesiamir sahirNo ratings yet
- Calculating Ideal Body Weight: Keep It SimpleDocument2 pagesCalculating Ideal Body Weight: Keep It SimpleAntonio RodriguezNo ratings yet
- Transtracheal LidocaineDocument4 pagesTranstracheal LidocaineaksinuNo ratings yet
- Managing Anticoagulated Patients During Neuraxial AnaesthesiaDocument15 pagesManaging Anticoagulated Patients During Neuraxial AnaesthesiaAnil KumarNo ratings yet
- Ultrasound-Guided Regional Anesthesia and Analgesia: A Qualitative Systematic ReviewDocument14 pagesUltrasound-Guided Regional Anesthesia and Analgesia: A Qualitative Systematic ReviewJuliana ObandoNo ratings yet
- Editorial Stress-Only Myocardial Perfusion Imaging It IS Time For A Change!Document4 pagesEditorial Stress-Only Myocardial Perfusion Imaging It IS Time For A Change!Ala PavlovNo ratings yet
- Effect of Dexamethasone On The Duration of Interscalene Nerve Blocks With Ropivacaine or BupivacaineDocument8 pagesEffect of Dexamethasone On The Duration of Interscalene Nerve Blocks With Ropivacaine or BupivacaineIda KatarinaNo ratings yet
- Difficult Intubation and Anesthetic Management in An Adult Patient With Undiagnosed Congenital Tracheal Stenosis: A Case ReportDocument6 pagesDifficult Intubation and Anesthetic Management in An Adult Patient With Undiagnosed Congenital Tracheal Stenosis: A Case ReportBianca CaterinalisendraNo ratings yet
- Fneur 14 1138354Document14 pagesFneur 14 1138354diego.arancibianutNo ratings yet
- Pediatric Regional AnesthesiaDocument6 pagesPediatric Regional Anesthesiatq9prx5s5qNo ratings yet
- Comparison of Ultrasound-Guided Thoracic Paravertebral and Pectoralis Interfascial Plane Block For Modified Radical MastectomyDocument7 pagesComparison of Ultrasound-Guided Thoracic Paravertebral and Pectoralis Interfascial Plane Block For Modified Radical MastectomyIJAR JOURNALNo ratings yet
- Sari 2021Document10 pagesSari 2021KhalilSemlaliNo ratings yet
- What's New in Ophthalmic AnaesthesiaDocument6 pagesWhat's New in Ophthalmic AnaesthesiaRahmi Ami100% (1)
- Assessment of Spinal Anaesthetic Block: ReferencesDocument3 pagesAssessment of Spinal Anaesthetic Block: ReferencesAlyssa MadriagaNo ratings yet
- Bloqueios AnestesiaDocument56 pagesBloqueios AnestesiaFatimaHelenaNo ratings yet
- Anestesia Locoregional y AnticoagulantesDocument6 pagesAnestesia Locoregional y Anticoagulantesluis castro martinezNo ratings yet
- The Nerves of The Adductor Canal and The Innervation of The KneeDocument7 pagesThe Nerves of The Adductor Canal and The Innervation of The KneeRoman PopescuNo ratings yet
- Anesthesia For Advanced Bronchoscopic Procedures: State-of-the-Art ReviewDocument13 pagesAnesthesia For Advanced Bronchoscopic Procedures: State-of-the-Art ReviewRichard PhoNo ratings yet
- NeuroestimulacionDocument5 pagesNeuroestimulacionWALTER GARCÍA TERCERONo ratings yet
- Nerve-Sparing Radical Hysterectomy in Cervical CancerDocument6 pagesNerve-Sparing Radical Hysterectomy in Cervical CancerdenisdeniNo ratings yet
- Epidural Space Identification A Meta Analysis Of.45Document10 pagesEpidural Space Identification A Meta Analysis Of.45Palliative MedicineNo ratings yet
- ACB Vs FIN NoninDocument12 pagesACB Vs FIN NoninLêQuangPhongNo ratings yet
- Peripheral Nerve Stimulation For Painful Mononeuropathy Secondary To Leprosy: A 12-Month Follow-Up StudyDocument6 pagesPeripheral Nerve Stimulation For Painful Mononeuropathy Secondary To Leprosy: A 12-Month Follow-Up StudySartika Ayu NingsihNo ratings yet
- Jurnal KardioDocument5 pagesJurnal KardiomadeNo ratings yet
- Ultrasonography in Trauma: A Nation-Wide Cross-Sectional InvestigationDocument6 pagesUltrasonography in Trauma: A Nation-Wide Cross-Sectional InvestigationEdison HernandezNo ratings yet
- 1 s2.0 S0007091223001654 Main PDFDocument5 pages1 s2.0 S0007091223001654 Main PDFEdward ElBuenoNo ratings yet
- Transcaruncular Double Injection Technique For Peribulbar Anesthesia in Vitreoretinal SurgeryDocument5 pagesTranscaruncular Double Injection Technique For Peribulbar Anesthesia in Vitreoretinal SurgeryanxNo ratings yet
- Pap Athanasiou 2014Document48 pagesPap Athanasiou 2014Caio LeônidasNo ratings yet
- Baru &Document6 pagesBaru &Bianca CaterinalisendraNo ratings yet
- Patient's Cures His Snoring: The EditorDocument1 pagePatient's Cures His Snoring: The EditorDiegoNo ratings yet
- Comparing The Efficacy of 2 Techniques For PiriforDocument2 pagesComparing The Efficacy of 2 Techniques For PiriforWidya AriatyNo ratings yet
- LECTURADocument6 pagesLECTURAKaren VillegasNo ratings yet
- A Retrospective Study of Success, Failure, and Time Needed To Perform Awake IntubationDocument10 pagesA Retrospective Study of Success, Failure, and Time Needed To Perform Awake IntubationAinun RamadaniNo ratings yet
- Diaphragm Ultrasound As A New Method To Predict Extubation Outcome in Mechanically VentilaDocument7 pagesDiaphragm Ultrasound As A New Method To Predict Extubation Outcome in Mechanically VentilaSilvanaNo ratings yet
- Literatür 3Document4 pagesLiteratür 3Sinan Kadir AltunalNo ratings yet
- Comparing Erector Spinae Plane Block With Serratus Anterio - 2020 - British JourDocument9 pagesComparing Erector Spinae Plane Block With Serratus Anterio - 2020 - British JourtasyadelizaNo ratings yet
- Comparison of Transcutaneous Electrical Tibial Nervestimulation For The Treatment of Overactive Bladder-A Multi-Arm Randomized Controlled Trial With BlindedassessmentDocument6 pagesComparison of Transcutaneous Electrical Tibial Nervestimulation For The Treatment of Overactive Bladder-A Multi-Arm Randomized Controlled Trial With BlindedassessmentMUHAMMMAD FAKHRINo ratings yet
- 1063 FullDocument2 pages1063 FullJossue LopezNo ratings yet
- Ultrasound-Guided Interventional Procedures in Pain ManagementDocument4 pagesUltrasound-Guided Interventional Procedures in Pain ManagementAuliya SyismaNo ratings yet
- Anestesi Umum Dan Regional Untuk Operasi Fraktur Hip: Ameta-Analisis Uji Coba Secara AcakDocument13 pagesAnestesi Umum Dan Regional Untuk Operasi Fraktur Hip: Ameta-Analisis Uji Coba Secara AcakmardianaNo ratings yet
- Expression of The Nociceptin Precursor and NocicepDocument7 pagesExpression of The Nociceptin Precursor and NocicepRENAULTNo ratings yet
- Lack of Agreement Between Pulmonary Arterial ThermDocument7 pagesLack of Agreement Between Pulmonary Arterial ThermRENAULTNo ratings yet
- Efficacy of Pregabalin in Acute Postoperative PainDocument9 pagesEfficacy of Pregabalin in Acute Postoperative PainRENAULTNo ratings yet
- Difficulty of Establishing Preoperative CoagulatioDocument1 pageDifficulty of Establishing Preoperative CoagulatioRENAULTNo ratings yet
- Population Pharmacokinetics of Nalbuphine After SuDocument8 pagesPopulation Pharmacokinetics of Nalbuphine After SuRENAULTNo ratings yet
- 2019 2020 Health History ExamDocument2 pages2019 2020 Health History Examsaranya purushothamanNo ratings yet
- Clinical Group Study Case 1Document8 pagesClinical Group Study Case 1Olivia JagroopNo ratings yet
- Circulating Nurse in Divine Word Hospital, Tacloban CityDocument1 pageCirculating Nurse in Divine Word Hospital, Tacloban CityKenneth AbillarNo ratings yet
- Lab Flow SheetDocument2 pagesLab Flow SheetRyan LazatinNo ratings yet
- UntitledDocument8 pagesUntitledDaniel Angelo ArangoNo ratings yet
- An Evidence-Based Approach To Pediatric MelanonychiaDocument13 pagesAn Evidence-Based Approach To Pediatric MelanonychiaMarice QCNo ratings yet
- STRDocument179 pagesSTRJatin AnandNo ratings yet
- 3 - Harada Mori TechniqueDocument2 pages3 - Harada Mori TechniqueHONEYLYNNE DELA TORRENo ratings yet
- NCP Pedia WardDocument2 pagesNCP Pedia WardSyrelle GomezNo ratings yet
- Biodata Dr. P. Sirohi - 2021.06.16Document10 pagesBiodata Dr. P. Sirohi - 2021.06.16kvpy iisc bangloreNo ratings yet
- Blood Vessels QuestionsDocument7 pagesBlood Vessels QuestionsT-Jay Ellis-DaleNo ratings yet
- NCMA 219 RLE Laboratory Unit 11bDocument7 pagesNCMA 219 RLE Laboratory Unit 11bJeeduu frostNo ratings yet
- Antimicrobial Peptides From Scorpion Venoms PDFDocument23 pagesAntimicrobial Peptides From Scorpion Venoms PDFOrlando Pérez DelgadoNo ratings yet
- LBM 6 Blok 20 SGD 1Document8 pagesLBM 6 Blok 20 SGD 1Ani LabibahNo ratings yet
- D. Nursing Care Plan: Impaired Gas Exchange Related To Altered Oxygen Supply As Evidenced by Difficulty in BreathingDocument2 pagesD. Nursing Care Plan: Impaired Gas Exchange Related To Altered Oxygen Supply As Evidenced by Difficulty in BreathingReinette LastrillaNo ratings yet
- Exam 1 Outline Notes - Docx NewDocument4 pagesExam 1 Outline Notes - Docx NewHeather MoralesNo ratings yet
- Challenges of Mass Casualty Management at A RegionDocument5 pagesChallenges of Mass Casualty Management at A RegionEbuwa AmadasunNo ratings yet
- LAS HEALTH 6 Q4 Wk5 Cherlyn. RonquilloDocument4 pagesLAS HEALTH 6 Q4 Wk5 Cherlyn. RonquilloANGELINA RAMBOYONGNo ratings yet
- 3 Mic125Document8 pages3 Mic125nadiazkiNo ratings yet
- Argumentative Essay.Document2 pagesArgumentative Essay.jeffersonNo ratings yet
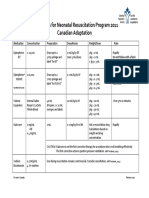
- Medications For Neonatal Resuscitation Program 2011 Canadian AdaptationDocument1 pageMedications For Neonatal Resuscitation Program 2011 Canadian AdaptationrubymayNo ratings yet
- Hema I Chapter 8 - DiffDocument67 pagesHema I Chapter 8 - DiffderibewNo ratings yet