You might also like
- Basic Pharmacology And Drug Calculations [Practice Questions And Answers]From EverandBasic Pharmacology And Drug Calculations [Practice Questions And Answers]Rating: 4 out of 5 stars4/5 (1)
- Xanax®: Reference ID: 2954409Document44 pagesXanax®: Reference ID: 2954409IrisNo ratings yet
- Xanax - FDADocument45 pagesXanax - FDAsanx19No ratings yet
- AlprazolamDocument10 pagesAlprazolamWen SilverNo ratings yet
- Chlorpheniramine MaleateDocument17 pagesChlorpheniramine MaleateMaria Abegail Gomez100% (1)
- Warnings: Clinical Worsening and Suicide Risk, Precautions: Information For Patients, and Precautions: Pediatric Use)Document19 pagesWarnings: Clinical Worsening and Suicide Risk, Precautions: Information For Patients, and Precautions: Pediatric Use)Zamin AhmedNo ratings yet
- NitrazepamDocument4 pagesNitrazepamJunilaNo ratings yet
- AlprazolamDocument16 pagesAlprazolamfachsyarNo ratings yet
- Alprazolam PoisoningDocument4 pagesAlprazolam PoisoningRahmat AkmalNo ratings yet
- Sinarest SyrupDocument9 pagesSinarest SyrupYidiv VidiyNo ratings yet
- Drug Class Review On BenzosDocument48 pagesDrug Class Review On BenzosRico RodriguezNo ratings yet
- Drugs Affecting The Central Nervous SystemDocument16 pagesDrugs Affecting The Central Nervous SystemShafaqNo ratings yet
- Drug Review-Tramadol.: Journal of The Institute of Medicine December 2006Document6 pagesDrug Review-Tramadol.: Journal of The Institute of Medicine December 2006NINDYA PRASTIWINo ratings yet
- Tugas Diskusi Farmakologi II (Senin, 12 Mei 2014)Document20 pagesTugas Diskusi Farmakologi II (Senin, 12 Mei 2014)ulyaNo ratings yet
- LorazepamDocument13 pagesLorazepamMariusNeicuNo ratings yet
- Tugas Farmasi Rumah Sakit Ringkasan Jurnal Alprazolam: OlehDocument8 pagesTugas Farmasi Rumah Sakit Ringkasan Jurnal Alprazolam: OlehMERINo ratings yet
- Schedule IVDocument40 pagesSchedule IVJeff Rey Casiño DalubatanNo ratings yet
- Drug StudyDocument4 pagesDrug StudyEmilyne Joy Mendoza CabayaNo ratings yet
- Sinarest Oral Drops Composition, Dosage and Clinical UseDocument5 pagesSinarest Oral Drops Composition, Dosage and Clinical UseHT Cooking ChannelNo ratings yet
- Anti Psychotics Odt'sDocument26 pagesAnti Psychotics Odt'ssaimanideepakNo ratings yet
- Alprazolam Uses, Dosage, Side EffectsDocument7 pagesAlprazolam Uses, Dosage, Side EffectspatgarettNo ratings yet
- Alprazolam Tablet Brands Compared by HPLC and TestsDocument12 pagesAlprazolam Tablet Brands Compared by HPLC and TestsLennin Rodriguez SaavedraNo ratings yet
- Prescribing information for Xanagis alprazolam tabletsDocument9 pagesPrescribing information for Xanagis alprazolam tabletsasdwasdNo ratings yet
- Untitlednf Fli DJ Ig Tu JDocument30 pagesUntitlednf Fli DJ Ig Tu JBEST OF BESTNo ratings yet
- A Guide To Psychotropic DrugsDocument16 pagesA Guide To Psychotropic DrugsNokz M. Raki-inNo ratings yet
- Side Effects.: Aripiprazole (Abilify)Document3 pagesSide Effects.: Aripiprazole (Abilify)Vera El Sammah SiagianNo ratings yet
- Salbutamol for Asthma and COPD ReliefDocument5 pagesSalbutamol for Asthma and COPD ReliefFildehl Janice Bomediano CatipayNo ratings yet
- 2022 11 07 14 18 42 Nursing AlprazolamDocument4 pages2022 11 07 14 18 42 Nursing Alprazolamninjatechnique10No ratings yet
- Paracetamol LeafletDocument3 pagesParacetamol LeafletJonathan AgnoyuNo ratings yet
- Parakol Tablet 500,60,2mg (Paracetamol,Pseudoephedrine,Dexchlorpheniramine) Duopharma (M) Sdn. Bhd. 19Jan2015 EngDocument4 pagesParakol Tablet 500,60,2mg (Paracetamol,Pseudoephedrine,Dexchlorpheniramine) Duopharma (M) Sdn. Bhd. 19Jan2015 EngTQINNo ratings yet
- DK H 0109 003 FinalPLDocument6 pagesDK H 0109 003 FinalPLAi BerlianNo ratings yet
- Panadol Sinus Relief Original Formula Tablets Product InformationDocument8 pagesPanadol Sinus Relief Original Formula Tablets Product Informationredof markzNo ratings yet
- Lorazepam - Wikipedia, The Free EncyclopediaDocument15 pagesLorazepam - Wikipedia, The Free Encyclopediaapi-18997839No ratings yet
- Chemistry ProjectDocument13 pagesChemistry ProjectMohammed AdnanNo ratings yet
- Paracetamol Use GuideDocument13 pagesParacetamol Use GuideShashiprakash KshatriyaNo ratings yet
- 10.1515 - Jom 1982 821114Document4 pages10.1515 - Jom 1982 821114realxsaloNo ratings yet
- Dextroamphetamine: Brand Name: DexedrineDocument23 pagesDextroamphetamine: Brand Name: DexedrineSharry Fe OasayNo ratings yet
- Dextroamphetamine: Brand Name: DexedrineDocument23 pagesDextroamphetamine: Brand Name: DexedrineSharry Fe OasayNo ratings yet
- Halcion Triazolam Tablets, USP CIV: DescriptionDocument14 pagesHalcion Triazolam Tablets, USP CIV: DescriptionAlberto JaramilloNo ratings yet
- Antispastics Emtyaz FDocument57 pagesAntispastics Emtyaz FMuhammed MuhsinNo ratings yet
- Acetaminophen, ParacetamolDocument2 pagesAcetaminophen, ParacetamolAubrey Unique Evangelista100% (2)
- Anti Anxiety AgentsDocument2 pagesAnti Anxiety Agentsapi-3712326No ratings yet
- Alfaxalone Vasg 05 11Document4 pagesAlfaxalone Vasg 05 11Cristian FloreaNo ratings yet
- Drug Study On EPINEPHRINEDocument6 pagesDrug Study On EPINEPHRINEshadow gonzalezNo ratings yet
- Types and Uses of Anti-Anxiety DrugsDocument39 pagesTypes and Uses of Anti-Anxiety DrugsArkene LevyNo ratings yet
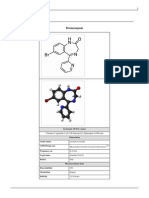
- BromazepamDocument6 pagesBromazepamMariusNeicuNo ratings yet
- ZolaxDocument2 pagesZolaxKhaled HasanNo ratings yet
- Ativan CIV Tablets: R OnlyDocument8 pagesAtivan CIV Tablets: R OnlyP KasikrishnarajaNo ratings yet
- Asthma Case Report: Overview of Drugs Used to Treat Acute Asthma AttackDocument23 pagesAsthma Case Report: Overview of Drugs Used to Treat Acute Asthma AttackFajar Al-HabibiNo ratings yet
- C C C CC C MMMM MMMMDocument10 pagesC C C CC C MMMM MMMMFerlyn PanchoNo ratings yet
- Lansoprazole 15mg, 30mg Gastro-Resistant Capsules: Package Leaflet: Information For The PatientDocument2 pagesLansoprazole 15mg, 30mg Gastro-Resistant Capsules: Package Leaflet: Information For The PatientResa Eni Santi WulandariNo ratings yet
- Pil 12339Document2 pagesPil 12339Manojit SarkarNo ratings yet
- Propranolol For Animals CatsDocument1 pagePropranolol For Animals CatsAkbar ShakoorNo ratings yet
- Antitussive Drugs-Noscapine & Others-08-04-2014Document19 pagesAntitussive Drugs-Noscapine & Others-08-04-2014Jumana hussainNo ratings yet
- Prescription Writing: Esha Ann FransonDocument9 pagesPrescription Writing: Esha Ann FransonAlosious JohnNo ratings yet
- 416697common Xanax Alprazolam RememberDocument2 pages416697common Xanax Alprazolam Rememberterlysq11cNo ratings yet
- Chemsitry Paracetamol ProjectDocument17 pagesChemsitry Paracetamol Projectjatinsinghal0808No ratings yet
- Pabron DM Syrup (Dextromethorphan,bromhexine) Hoe Pharmaceuticals 18Apr2014 Eng.pdfDocument2 pagesPabron DM Syrup (Dextromethorphan,bromhexine) Hoe Pharmaceuticals 18Apr2014 Eng.pdfTQINNo ratings yet
- Ans NursingDocument15 pagesAns Nursingwww.nikhilbabu123No ratings yet
- Definition / General: UlcerDocument2 pagesDefinition / General: UlcerShahzad AsifNo ratings yet
- Quinine Alkaloid from Cinchona BarkDocument1 pageQuinine Alkaloid from Cinchona BarkShahzad AsifNo ratings yet
- Quinine Alkaloid from Cinchona BarkDocument1 pageQuinine Alkaloid from Cinchona BarkShahzad AsifNo ratings yet
- Pharmacological Classification of Drugs First EditionDocument0 pagesPharmacological Classification of Drugs First EditionAmina BećiragićNo ratings yet
- Midterm MMMDocument2 pagesMidterm MMMasdfghjkl zxcvbnmNo ratings yet
- SGLGB Form 1 Barangay ProfileDocument3 pagesSGLGB Form 1 Barangay ProfileHELEN CASIANONo ratings yet
- Electrical Isolation Work PermitDocument2 pagesElectrical Isolation Work PermitGreg GenoveNo ratings yet
- Airworthiness Directives Record ControlDocument4 pagesAirworthiness Directives Record ControlJuan builesNo ratings yet
- Iocl Section 1 - Process SpecficationDocument73 pagesIocl Section 1 - Process SpecficationYogi173No ratings yet
- Barriers To Nurse - Patient Communication in Saudi Arabia: An Integrative ReviewDocument10 pagesBarriers To Nurse - Patient Communication in Saudi Arabia: An Integrative Reviewmark3dasaNo ratings yet
- MONO POWER AMPLIFIER SERVICE MANUALDocument34 pagesMONO POWER AMPLIFIER SERVICE MANUALAlexey OnishenkoNo ratings yet
- Crop RotationsDocument19 pagesCrop RotationsSarwar M. RasheedNo ratings yet
- MODULE 9: Personal Relationships: Albert Abarabar, Erica Soriano, Lloyd Sarandi, Julius Dela CruzDocument18 pagesMODULE 9: Personal Relationships: Albert Abarabar, Erica Soriano, Lloyd Sarandi, Julius Dela CruzMark Gil GuillermoNo ratings yet
- Working at Height PolicyDocument7 pagesWorking at Height PolicyAniekan AkpaidiokNo ratings yet
- Letter From Springfield Mayor Sarno To License Commission Re: Late Night Hours.Document12 pagesLetter From Springfield Mayor Sarno To License Commission Re: Late Night Hours.Patrick JohnsonNo ratings yet
- 1:21-cv-03674 Coomes, Williams, Slater & Tisbert vs. Centerra Group, LLCDocument16 pages1:21-cv-03674 Coomes, Williams, Slater & Tisbert vs. Centerra Group, LLCMichelle EdwardsNo ratings yet
- Refrac 2Document20 pagesRefrac 2PawanNo ratings yet
- S35MC Engine Layout and Load DiagramsDocument17 pagesS35MC Engine Layout and Load DiagramsMuhammad AlfaniNo ratings yet
- Aminacid MetabolismDocument84 pagesAminacid MetabolismAaronJose100% (1)
- Application Format For Child CustodyDocument2 pagesApplication Format For Child CustodyDHUP CHAND JAISWAL100% (3)
- Corporate Governance at HavellsDocument16 pagesCorporate Governance at HavellsVishal Pundir100% (1)
- Convey 1996Document8 pagesConvey 1996Moises Tinte100% (1)
- Thermo Fluids LabDocument23 pagesThermo Fluids LabMuket AgmasNo ratings yet
- Include The Following in Your RTI ApplicationDocument4 pagesInclude The Following in Your RTI ApplicationRam LoharNo ratings yet
- Practical-2 Simulation of ReactorsDocument2 pagesPractical-2 Simulation of ReactorsniralNo ratings yet
- Conversion Disorder in Childhood: James R. BrašićDocument8 pagesConversion Disorder in Childhood: James R. BrašićmasriffaNo ratings yet
- Mandaya: Presented By: Cutad, Ray Dag-Uman, Ely Mae Cortes, MaikoDocument24 pagesMandaya: Presented By: Cutad, Ray Dag-Uman, Ely Mae Cortes, MaikoAPPLE MAE AGOSTONo ratings yet
- Assessment Toolkit: Health InequalitiesDocument30 pagesAssessment Toolkit: Health InequalitiesAlejandro CardonaNo ratings yet
- Comparative Population Growth and Losses Cause by Beetle Trogoderama Granarium (Everts) To Selected Past and Present Wheat GenotypesDocument12 pagesComparative Population Growth and Losses Cause by Beetle Trogoderama Granarium (Everts) To Selected Past and Present Wheat GenotypesInternational Network For Natural SciencesNo ratings yet
- Quotes by Clarissa Pinkola Estés (Author of Women Who Run With The Wolves)Document1 pageQuotes by Clarissa Pinkola Estés (Author of Women Who Run With The Wolves)Nes GillNo ratings yet
- Physical ExaminationDocument7 pagesPhysical ExaminationCha CulveraNo ratings yet
- Anatomy of The PeriodontiumDocument46 pagesAnatomy of The PeriodontiumYunita Nitnot50% (2)
- State-wise list of 376 approved cold chain projectsDocument45 pagesState-wise list of 376 approved cold chain projectsUsha Hasini VelagapudiNo ratings yet
- Minaral and MetalDocument109 pagesMinaral and Metaldeva nesan100% (1)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Don't Panic: Taking Control of Anxiety AttacksFrom EverandDon't Panic: Taking Control of Anxiety AttacksRating: 4 out of 5 stars4/5 (12)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (38)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (140)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionFrom EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNo ratings yet
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaFrom EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaRating: 4.5 out of 5 stars4.5/5 (56)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (1)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreFrom EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreRating: 5 out of 5 stars5/5 (17)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveFrom EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveRating: 4 out of 5 stars4/5 (249)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesFrom EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesRating: 5 out of 5 stars5/5 (70)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- When Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionFrom EverandWhen Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionRating: 4 out of 5 stars4/5 (11)
- Fighting Words Devotional: 100 Days of Speaking Truth into the DarknessFrom EverandFighting Words Devotional: 100 Days of Speaking Truth into the DarknessRating: 5 out of 5 stars5/5 (6)
- Overcoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsFrom EverandOvercoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsRating: 4.5 out of 5 stars4.5/5 (48)
- BORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONFrom EverandBORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONRating: 4.5 out of 5 stars4.5/5 (24)
- Winning the War in Your Mind: Change Your Thinking, Change Your LifeFrom EverandWinning the War in Your Mind: Change Your Thinking, Change Your LifeRating: 5 out of 5 stars5/5 (558)
- Smart Phone Dumb Phone: Free Yourself from Digital AddictionFrom EverandSmart Phone Dumb Phone: Free Yourself from Digital AddictionRating: 5 out of 5 stars5/5 (11)
- Insecure in Love: How Anxious Attachment Can Make You Feel Jealous, Needy, and Worried and What You Can Do About ItFrom EverandInsecure in Love: How Anxious Attachment Can Make You Feel Jealous, Needy, and Worried and What You Can Do About ItRating: 4.5 out of 5 stars4.5/5 (84)
- Call of the Wild: How We Heal Trauma, Awaken Our Own Power, and Use It For GoodFrom EverandCall of the Wild: How We Heal Trauma, Awaken Our Own Power, and Use It For GoodNo ratings yet
- Binaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationFrom EverandBinaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationRating: 5 out of 5 stars5/5 (9)
- The Somatic Psychotherapy Toolbox: A Comprehensive Guide to Healing Trauma and StressFrom EverandThe Somatic Psychotherapy Toolbox: A Comprehensive Guide to Healing Trauma and StressNo ratings yet
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeFrom EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeRating: 4.5 out of 5 stars4.5/5 (49)
- Emotional Detox for Anxiety: 7 Steps to Release Anxiety and Energize JoyFrom EverandEmotional Detox for Anxiety: 7 Steps to Release Anxiety and Energize JoyRating: 5 out of 5 stars5/5 (6)
- The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk: Key Takeaways, Summary & AnalysisFrom EverandThe Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (2)
![Basic Pharmacology And Drug Calculations [Practice Questions And Answers]](https://imgv2-1-f.scribdassets.com/img/word_document/475660044/149x198/2c7fc45015/1691161640?v=1)