You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Nursing Care Plan - Pericarditis PatientDocument2 pagesNursing Care Plan - Pericarditis Patientsandie_best78% (9)
- Week 4 DiscussionDocument1 pageWeek 4 DiscussionJacob YorgNo ratings yet
- Understanding Culture, Society, and Politics: Second QuarterDocument12 pagesUnderstanding Culture, Society, and Politics: Second QuarterRene Rey B. Sulapas85% (13)
- Recombinant Activated Factor VII Usage in Life Threatening Hemorrhage A Pediatric ExperienceDocument8 pagesRecombinant Activated Factor VII Usage in Life Threatening Hemorrhage A Pediatric ExperienceSyahrul HamidNo ratings yet
- Gastrointestinal Perforation Clinical and MDCT Clues For Identification of AetiologyDocument19 pagesGastrointestinal Perforation Clinical and MDCT Clues For Identification of AetiologySyahrul HamidNo ratings yet
- Urosepsis: Definition, Diagnosis and TreatmentDocument6 pagesUrosepsis: Definition, Diagnosis and TreatmentSyahrul HamidNo ratings yet
- Effects of Sleep Disorders On Hemoglobin A1c Levels in Type 2 Diabetic PatientsDocument6 pagesEffects of Sleep Disorders On Hemoglobin A1c Levels in Type 2 Diabetic PatientsSyahrul HamidNo ratings yet
- BMJ k4641 FullDocument10 pagesBMJ k4641 FullSyahrul HamidNo ratings yet
- DR Franciscus Ginting - Sepsis PIN PAPDI SurabayaDocument82 pagesDR Franciscus Ginting - Sepsis PIN PAPDI SurabayaSyahrul HamidNo ratings yet
- Sepsis 2018 Definitions and Guideline Changes PDFDocument9 pagesSepsis 2018 Definitions and Guideline Changes PDFSyahrul HamidNo ratings yet
- The Role of The Gut Microbiota in SepsisDocument9 pagesThe Role of The Gut Microbiota in SepsisSyahrul HamidNo ratings yet
- 9 - Maroney Et Al (2019) - Emergence of A Transnational LGBTI PsychologyDocument20 pages9 - Maroney Et Al (2019) - Emergence of A Transnational LGBTI PsychologyJean AraújoNo ratings yet
- DIASS Quarter1 Module 1Document24 pagesDIASS Quarter1 Module 1JoshNo ratings yet
- Amplitude-Oriented Exercise in Parkinson's Disease: A Randomized Study Comparing LSVT-BIG and A Short Training ProtocolDocument4 pagesAmplitude-Oriented Exercise in Parkinson's Disease: A Randomized Study Comparing LSVT-BIG and A Short Training ProtocolcaroNo ratings yet
- Module 6 Incentive ProgramDocument34 pagesModule 6 Incentive ProgramKavin RajNo ratings yet
- The National Academies Press: Risk Assessment of Proposed ARFF Standards (2011)Document105 pagesThe National Academies Press: Risk Assessment of Proposed ARFF Standards (2011)Marius BuysNo ratings yet
- MENTOR 13 Lionel Rammamurthy Oet For NursingDocument4 pagesMENTOR 13 Lionel Rammamurthy Oet For NursingAnjana Varghese0% (1)
- Lazard HealthcareDocument4 pagesLazard HealthcareMichael CabarloNo ratings yet
- Parents Consent FormDocument1 pageParents Consent FormPaz Calipes CayagoNo ratings yet
- Variation of PEFR With Height, Weight and Waist-Hip Ratio in Medical StudentsDocument6 pagesVariation of PEFR With Height, Weight and Waist-Hip Ratio in Medical StudentsInternational Medical PublisherNo ratings yet
- Nursing As A ProfessionDocument9 pagesNursing As A Professionvivian joy bulosanNo ratings yet
- MLA FormatDocument4 pagesMLA Formatkevin ochiengNo ratings yet
- IR 1Q2020 Prev-Min PDFDocument24 pagesIR 1Q2020 Prev-Min PDFSirc ElocinNo ratings yet
- HRM - Class TestDocument10 pagesHRM - Class TestArfreden DenNo ratings yet
- Employee Testing and Selection: Global Edition 12eDocument39 pagesEmployee Testing and Selection: Global Edition 12eMI2preciousNo ratings yet
- Safety Data Sheet: Masterseal CR 125Document10 pagesSafety Data Sheet: Masterseal CR 125Sam MalikNo ratings yet
- Trans-Radial Manufacturing GuidelinesDocument24 pagesTrans-Radial Manufacturing Guidelinesdilla fifiani nurhalifahNo ratings yet
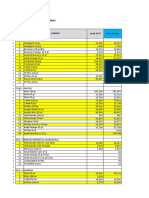
- Bahan Kemas - Selisih SO Vs Sistem FY2020 - 291220Document17 pagesBahan Kemas - Selisih SO Vs Sistem FY2020 - 291220Idan RidwanNo ratings yet
- Essay On The Pearl by John SteinbeckDocument6 pagesEssay On The Pearl by John Steinbeckafabittrf100% (2)
- 1958 FullDocument12 pages1958 FulldupitosariNo ratings yet
- WD 3-October ProjectsDocument2 pagesWD 3-October Projectsfake name100% (2)
- IELTS Speaking Task Sheets: Week 8: HealthDocument1 pageIELTS Speaking Task Sheets: Week 8: HealthÁnh ĐỗNo ratings yet
- Unit 1Document89 pagesUnit 1Rudra Sai SandeepNo ratings yet
- CASP - RCT - Efficacy of Ondansetron For Spinal Anesthesia During Cesarean Section A Metaanalysis of Randomized TrialsDocument4 pagesCASP - RCT - Efficacy of Ondansetron For Spinal Anesthesia During Cesarean Section A Metaanalysis of Randomized TrialsaltaikhsannurNo ratings yet
- The Masque of The Red Death: Annotation Column Literary TextDocument4 pagesThe Masque of The Red Death: Annotation Column Literary TextAda StachowskaNo ratings yet
- Notification - FMG Allotment - May - 2023Document1 pageNotification - FMG Allotment - May - 2023Elizabeth VargheseNo ratings yet
- SURESH Testing ProfileDocument3 pagesSURESH Testing Profilefreecharge momNo ratings yet