You might also like
- Dr. Anad's Guide to Urosepsis: Causes, Symptoms and TreatmentDocument23 pagesDr. Anad's Guide to Urosepsis: Causes, Symptoms and TreatmentJihad Anad100% (1)
- Septicaemia (Bacterial Sepsis) and TB Lymphadenitis: Prepared By: Dr. Zacharia J.Z. ToyiDocument29 pagesSepticaemia (Bacterial Sepsis) and TB Lymphadenitis: Prepared By: Dr. Zacharia J.Z. ToyiGideon HaburaNo ratings yet
- UrosepsaDocument2 pagesUrosepsaHazir AziriNo ratings yet
- Referat SepsisDocument18 pagesReferat SepsisImelva GirsangNo ratings yet
- Dr. Sana Bashir DPT, MS-CPPTDocument46 pagesDr. Sana Bashir DPT, MS-CPPTbkdfiesefll100% (1)
- Berkas Panum PonorogoDocument10 pagesBerkas Panum PonorogoDimas Novian SNo ratings yet
- GS 201-250Document19 pagesGS 201-250Sara Abdul RahmanNo ratings yet
- Causes of Drowsiness in This PatientDocument12 pagesCauses of Drowsiness in This PatientNu JoeNo ratings yet
- Delay in Diagnosis of Extra-Pulmonary Tuberculosis by Its Rare Manifestations: A Case ReportDocument5 pagesDelay in Diagnosis of Extra-Pulmonary Tuberculosis by Its Rare Manifestations: A Case ReportSneeze LouderNo ratings yet
- Urosepsis: Dr. Tameem Mohammed Department of Anesthesia and Intensive Care San Fernando General HospitalDocument22 pagesUrosepsis: Dr. Tameem Mohammed Department of Anesthesia and Intensive Care San Fernando General HospitalRicky AliNo ratings yet
- Sepsis and Septic Shock - Critical Care MedicineDocument2 pagesSepsis and Septic Shock - Critical Care MedicineMihaela MoraruNo ratings yet
- Sepsis Diagnosis and ManagementDocument12 pagesSepsis Diagnosis and ManagementYudhistira AdiNo ratings yet
- Matas 2020Document9 pagesMatas 2020Aubrey PerezNo ratings yet
- Pseudomonas Aeruginosa InfectionsDocument22 pagesPseudomonas Aeruginosa InfectionsMiguel RomeroNo ratings yet
- Bacteremia - Dan - Sepsis and ShockDocument232 pagesBacteremia - Dan - Sepsis and ShockKiki Luhita SariNo ratings yet
- PneumoniaDocument8 pagesPneumoniaCostescu ClaudiaNo ratings yet
- Management of Septic ShockDocument33 pagesManagement of Septic ShockswatisinghnigeriaNo ratings yet
- 8.3 Medicine - Tropical Infectious Diseases Leptospirosis 2014ADocument7 pages8.3 Medicine - Tropical Infectious Diseases Leptospirosis 2014ABhi-An BatobalonosNo ratings yet
- Infection in Critical CareDocument34 pagesInfection in Critical CareSuresh Kumar BansalNo ratings yet
- Superficial Infection and SepisDocument35 pagesSuperficial Infection and Sepissanjivdas100% (1)
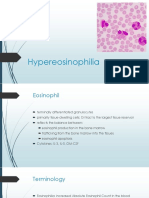
- Hypereosinophilia: DR Satya PrakashDocument19 pagesHypereosinophilia: DR Satya PrakashSatya PrakashNo ratings yet
- 1 Bacterial Fungal Infections of Blood PDFDocument54 pages1 Bacterial Fungal Infections of Blood PDFahmad mohammadNo ratings yet
- Eritema Nodoso UpdateDocument20 pagesEritema Nodoso UpdateAna Flavia BaptistaNo ratings yet
- Metod Terapiya Lechebnoe Delo Fakul'tet Inostranyx Studentov-006Document29 pagesMetod Terapiya Lechebnoe Delo Fakul'tet Inostranyx Studentov-006Nishani SatiyaseelanNo ratings yet
- Jurnal Bahasa InggrisDocument12 pagesJurnal Bahasa InggrisVanessa Angelica SitepuNo ratings yet
- Assessment of Splenic Function: ReviewDocument9 pagesAssessment of Splenic Function: Reviewjosias_aragao3527No ratings yet
- Understanding BronchiectasisDocument23 pagesUnderstanding BronchiectasisRamanda Cahya UmbarraNo ratings yet
- Capp&Dwe TomeldenfinalDocument74 pagesCapp&Dwe Tomeldenfinaltomeldenalyssa13No ratings yet
- Case 06Document5 pagesCase 06Chefera AgaNo ratings yet
- Eosinophilic Granulomatosis With Polyangiitis and Bowel Perforation: Case ReportDocument5 pagesEosinophilic Granulomatosis With Polyangiitis and Bowel Perforation: Case ReportSabrina JonesNo ratings yet
- Essential Update: CDC Expands Guidelines For Carbapenem-Resistant EnterobacteriaceaeDocument5 pagesEssential Update: CDC Expands Guidelines For Carbapenem-Resistant EnterobacteriaceaeRobertus HajaiNo ratings yet
- Approach To A Patient With Urosepsis: Om KalraDocument8 pagesApproach To A Patient With Urosepsis: Om KalraZulfahmi MusllimNo ratings yet
- Acute Poststreptococcal Glomerulonephritis (Apsgn) in ChildrenDocument22 pagesAcute Poststreptococcal Glomerulonephritis (Apsgn) in ChildrenOlivia PutriNo ratings yet
- Amjad Bani Hani: Sir S, Sep S Is, A N D ModsDocument67 pagesAmjad Bani Hani: Sir S, Sep S Is, A N D ModsRuffaeelJabrNo ratings yet
- Evaluation of The Febrile Patient A Case-Based Approach: Fevers and Fevers of Unknown OriginDocument97 pagesEvaluation of The Febrile Patient A Case-Based Approach: Fevers and Fevers of Unknown Originkrish vjNo ratings yet
- 1663503021Document23 pages1663503021lovekohli235No ratings yet
- Acute GlomerulonephritisDocument4 pagesAcute GlomerulonephritisJulliza Joy PandiNo ratings yet
- Septic ArthritisDocument32 pagesSeptic ArthritisDr. BosotovNo ratings yet
- Content SP HantavirusDocument7 pagesContent SP HantavirusGusti Ayu AdhipNo ratings yet
- Lepto Spiros IsDocument27 pagesLepto Spiros IscipacipaaNo ratings yet
- Infectious EndocarditisDocument19 pagesInfectious Endocarditisinyanji.barasaNo ratings yet
- Med KeywordsDocument67 pagesMed KeywordsSwisskelly1No ratings yet
- PleuritisDocument48 pagesPleuritisMuhammad FhaliqNo ratings yet
- Understanding Bronchiectasis: Causes, Symptoms and TreatmentDocument60 pagesUnderstanding Bronchiectasis: Causes, Symptoms and TreatmentArulNo ratings yet
- A Treacherous Course: Clinical Problem-SolvingDocument6 pagesA Treacherous Course: Clinical Problem-SolvingMorocco CandycatyNo ratings yet
- Pulmonary Miliary Tuberculosis Complicated With Tuberculous Spondylitis An Extraordinary Rare Association: A Case ReportDocument5 pagesPulmonary Miliary Tuberculosis Complicated With Tuberculous Spondylitis An Extraordinary Rare Association: A Case ReportIsmail Eko SaputraNo ratings yet
- Infective Endocarditis: Ainal Fadly Adigama PF Enny SuryantiDocument50 pagesInfective Endocarditis: Ainal Fadly Adigama PF Enny SuryantiFaisal Reza AdiebNo ratings yet
- Intern TicklerDocument10 pagesIntern TicklerRem AlfelorNo ratings yet
- Radiology Case Report - Splenic AbscessDocument6 pagesRadiology Case Report - Splenic AbscessAbeebNo ratings yet
- Clinical Presentation: by Dr. Raffiq AbbasDocument36 pagesClinical Presentation: by Dr. Raffiq AbbasKarthick UnleashNo ratings yet
- SepticshocknemwDocument26 pagesSepticshocknemwanrimalikaNo ratings yet
- Fulminant Hemophagocytic Lymphohistiocytosis Induced by Pandemic A (H1N1) Influenza: A Case ReportDocument4 pagesFulminant Hemophagocytic Lymphohistiocytosis Induced by Pandemic A (H1N1) Influenza: A Case ReportrahNo ratings yet
- Wegeners GranulomatosisDocument65 pagesWegeners GranulomatosisLily HaslinaNo ratings yet
- Pancytopenia Secondary To Bacterial SepsisDocument16 pagesPancytopenia Secondary To Bacterial Sepsisiamralph89No ratings yet
- Sepsis and Septic ShockDocument4 pagesSepsis and Septic Shockبو عقيل الشيخ حسينNo ratings yet
- The Presentation - Crohn's Disease - (3course)Document17 pagesThe Presentation - Crohn's Disease - (3course)Kashif KhandaNo ratings yet
- Bacterial Uropathogenic Factors & Host DefensesDocument7 pagesBacterial Uropathogenic Factors & Host DefensesAtma AdiatmaNo ratings yet
- Pharmacotherapy of PneumoniaDocument56 pagesPharmacotherapy of Pneumoniahoneylemon.co100% (1)
- Jurnal 1 PDFDocument10 pagesJurnal 1 PDFrina feraNo ratings yet
- Recombinant Activated Factor VII Usage in Life Threatening Hemorrhage A Pediatric ExperienceDocument8 pagesRecombinant Activated Factor VII Usage in Life Threatening Hemorrhage A Pediatric ExperienceSyahrul HamidNo ratings yet
- AyoylulysluslyslaylgaDocument208 pagesAyoylulysluslyslaylgaRifqiNo ratings yet
- Expert Consensus on Assessment and Management of Agitation in PsychiatryDocument44 pagesExpert Consensus on Assessment and Management of Agitation in PsychiatryAmi Septia HardiyantiNo ratings yet
- Fecal Incontinence After Posterior Sagittal Anorectoplasty Foranorectal Malformation A Single-Center StudyDocument4 pagesFecal Incontinence After Posterior Sagittal Anorectoplasty Foranorectal Malformation A Single-Center StudySyahrul HamidNo ratings yet
- Delayed Intrathoracic Gastric Perforation After Obesity Surgery A Severe ComplicationDocument2 pagesDelayed Intrathoracic Gastric Perforation After Obesity Surgery A Severe ComplicationSyahrul HamidNo ratings yet
- Gastrointestinal Perforation Clinical and MDCT Clues For Identification of AetiologyDocument19 pagesGastrointestinal Perforation Clinical and MDCT Clues For Identification of AetiologySyahrul HamidNo ratings yet
- 383 2010 Article 2688Document7 pages383 2010 Article 2688Thallita Rahma ZiharviardyNo ratings yet
- Management and Associated Factors of Delayed Perforation After Gastric Endoscopic Submucosal DissectionDocument10 pagesManagement and Associated Factors of Delayed Perforation After Gastric Endoscopic Submucosal DissectionSyahrul HamidNo ratings yet
- BMJ k4641 FullDocument10 pagesBMJ k4641 FullSyahrul HamidNo ratings yet
- 9517 18923 1 SMDocument5 pages9517 18923 1 SMMheymi YantiNo ratings yet
- Sleep and Obesity PDFDocument18 pagesSleep and Obesity PDFAnnida NdaNo ratings yet
- Effects of Sleep Disorders On Hemoglobin A1c Levels in Type 2 Diabetic PatientsDocument6 pagesEffects of Sleep Disorders On Hemoglobin A1c Levels in Type 2 Diabetic PatientsSyahrul HamidNo ratings yet
- Antenatal CareDocument12 pagesAntenatal CarefiramnNo ratings yet
- 08 Oa Sleep and Type 2Document6 pages08 Oa Sleep and Type 2Rika FitriaNo ratings yet
- Management Sepsis TerkiniDocument82 pagesManagement Sepsis TerkiniSyahrul HamidNo ratings yet
- Sepsis 2018 Definitions and Guideline Changes PDFDocument9 pagesSepsis 2018 Definitions and Guideline Changes PDFSyahrul HamidNo ratings yet
- NSF Sleep Quality IndicatorsDocument14 pagesNSF Sleep Quality IndicatorsSyahrul HamidNo ratings yet
- The Immunopathology of Sepsis and Potential Therapeutic Targets PDFDocument14 pagesThe Immunopathology of Sepsis and Potential Therapeutic Targets PDFSyahrul HamidNo ratings yet
- Abdominal Sepsis.15Document8 pagesAbdominal Sepsis.15Dario Xavier Achachi MelendezNo ratings yet
- Review Sepsi LancetDocument13 pagesReview Sepsi LancetMr. LNo ratings yet
- The Role of The Gut Microbiota in SepsisDocument9 pagesThe Role of The Gut Microbiota in SepsisSyahrul HamidNo ratings yet
- Accomplishment Target For The Month of October C.Y. 2020Document16 pagesAccomplishment Target For The Month of October C.Y. 2020jamesdigolNo ratings yet
- Assisting DeliveryDocument2 pagesAssisting DeliveryKate Gabrielle Donal De GuzmanNo ratings yet
- Columbia-Suicide Severity Rating Scale (C-SSRS) : Past 3 Months LifetimeDocument1 pageColumbia-Suicide Severity Rating Scale (C-SSRS) : Past 3 Months LifetimeIzabel EstevamNo ratings yet
- Soc 3480 Final Research Paper 1Document25 pagesSoc 3480 Final Research Paper 1api-516694258No ratings yet
- AF Catheter AblationDocument37 pagesAF Catheter AblationSnehal JayaramNo ratings yet
- Lac NL - Spring 2021Document8 pagesLac NL - Spring 2021Ghassan NajmNo ratings yet
- Muscle and Bone Activities for a Strong BodyDocument13 pagesMuscle and Bone Activities for a Strong BodyAlex ValdecañasNo ratings yet
- 2020 International Society of Hypertension Global Hypertension Practice GuidelinesDocument15 pages2020 International Society of Hypertension Global Hypertension Practice GuidelinesIntan PermatasariNo ratings yet
- Two REBT Therapists and One Client: Ellis TranscriptDocument12 pagesTwo REBT Therapists and One Client: Ellis TranscriptJoaquin OlivaresNo ratings yet
- AugustDocument6 pagesAugustchathurika dulanjaliNo ratings yet
- Differences and similarities among the three dopamine receptor partial agonistsDocument10 pagesDifferences and similarities among the three dopamine receptor partial agonistsolivukovic100% (1)
- Assessment of the Skin, Hair and NailsDocument19 pagesAssessment of the Skin, Hair and NailsBaniwas Marie AgnesNo ratings yet
- Junal 1Document6 pagesJunal 1indadzi arsyNo ratings yet
- TAROSANAN-Sub-Project-Completion-Report Dec. 20, 2023Document16 pagesTAROSANAN-Sub-Project-Completion-Report Dec. 20, 2023Mara Kenia BarcelonNo ratings yet
- Long-Term Abstinence Following Holotropic Breathwork As Adjunctive Treatment of Substance Use Disorders and Related Psychiatric ComorbidityDocument7 pagesLong-Term Abstinence Following Holotropic Breathwork As Adjunctive Treatment of Substance Use Disorders and Related Psychiatric ComorbiditymghuesoNo ratings yet
- Uts ReadingDocument7 pagesUts ReadingLaisah IdrNo ratings yet
- How To Sleep BetterDocument9 pagesHow To Sleep BetterMariaNo ratings yet
- Health and Environmental Impacts of Cleaning AgentsDocument8 pagesHealth and Environmental Impacts of Cleaning AgentsZafira Nurul FizaNo ratings yet
- Get Shredded PDFDocument40 pagesGet Shredded PDFLisandro Cacciatore100% (3)
- Behaviorist Learning TheoryDocument2 pagesBehaviorist Learning TheoryBadine De LeonNo ratings yet
- The Best Lifts For Real World Strength & Strongman CompetitionDocument3 pagesThe Best Lifts For Real World Strength & Strongman CompetitionIlijaNo ratings yet
- SPTL Ohs&e 40 Ohse MPR AbrarDocument22 pagesSPTL Ohs&e 40 Ohse MPR AbrarRanjeet Kumar SinghNo ratings yet
- Biology 2 Macromolecules and NutrientsDocument16 pagesBiology 2 Macromolecules and NutrientsMwendalubi ChiholyongaNo ratings yet
- Fate of Manganese Associated With The Inhalation of Welding Fumes: Potential Neurological EffectsDocument7 pagesFate of Manganese Associated With The Inhalation of Welding Fumes: Potential Neurological EffectsAndrea Carolina Salas LalindeNo ratings yet
- Planning ProcessDocument9 pagesPlanning ProcessSimran JosanNo ratings yet
- Medical Certificate: Healthservices@lnu - Edu.phDocument3 pagesMedical Certificate: Healthservices@lnu - Edu.phNiko ChavezNo ratings yet
- ItDocument4 pagesItNguyễn Duy HuânNo ratings yet
- Flooding in Pakistan: Overview and Issues For Congress: K. Alan Kronstadt, CoordinatorDocument33 pagesFlooding in Pakistan: Overview and Issues For Congress: K. Alan Kronstadt, Coordinatorahmed shakeelNo ratings yet
- H2S Monitor Manual - Tango TX1Document50 pagesH2S Monitor Manual - Tango TX1MattNo ratings yet
- Instability of The Distal Radioulnar JointDocument12 pagesInstability of The Distal Radioulnar JointOryza SatriaNo ratings yet