You might also like
- Updated Containment Plan For Large Outbreaks: Novel Coronavirus Disease 2019 (COVID-19)Document23 pagesUpdated Containment Plan For Large Outbreaks: Novel Coronavirus Disease 2019 (COVID-19)Mahesh PethkarNo ratings yet
- Controlling the COVID-19 PandemicDocument3 pagesControlling the COVID-19 Pandemicjjmmaarrkk01No ratings yet
- Containment Plan: Novel Coronavirus Disease 2019 (COVID 19)Document22 pagesContainment Plan: Novel Coronavirus Disease 2019 (COVID 19)Mayank MishraNo ratings yet
- Updated Containment Plan For Large Outbreaks: Novel Coronavirus Disease 2019 (COVID-19)Document21 pagesUpdated Containment Plan For Large Outbreaks: Novel Coronavirus Disease 2019 (COVID-19)Soham SarangiNo ratings yet
- Pandemic Preparedness PlanDocument40 pagesPandemic Preparedness PlanMurali Vallipuranathan100% (2)
- Containment Plan For Large Outbreaks: Novel Coronavirus Disease 2019 (COVID-19)Document20 pagesContainment Plan For Large Outbreaks: Novel Coronavirus Disease 2019 (COVID-19)Vijay SharmaNo ratings yet
- SceirdDocument9 pagesSceirdGiaWay HsuNo ratings yet
- Covid 19: Scenarios Août 2022Document12 pagesCovid 19: Scenarios Août 2022Journal L'Indépendant100% (1)
- Mathematical Modelling of COVID-19 Transmission and Mitigation Strategies in The Population of Ontario, CanadaDocument9 pagesMathematical Modelling of COVID-19 Transmission and Mitigation Strategies in The Population of Ontario, CanadaGuillermo Rodriguez LopezNo ratings yet
- Burden of post-COVID-19 Syndrome and Implications For Healthcare Service Planning: A Population-Based Cohort StudyDocument19 pagesBurden of post-COVID-19 Syndrome and Implications For Healthcare Service Planning: A Population-Based Cohort StudyValentinaLobosNo ratings yet
- The Effectiveness of The Quarantine of Wuhan City Against TheDocument25 pagesThe Effectiveness of The Quarantine of Wuhan City Against ThejameiNo ratings yet
- Aime202005050 m200504Document7 pagesAime202005050 m200504Ramsha RumaanNo ratings yet
- Asia Covid EstrategiasDocument10 pagesAsia Covid EstrategiasJonell SanchezNo ratings yet
- Acop - Incubation Period of Covid-19Document7 pagesAcop - Incubation Period of Covid-19yorghiLNo ratings yet
- COVID-19 Scientific Advisory Group Rapid Response ReportDocument12 pagesCOVID-19 Scientific Advisory Group Rapid Response ReportSureshNo ratings yet
- Modelling Transmission and Control of The COVID-19 Pandemic in AustraliaDocument24 pagesModelling Transmission and Control of The COVID-19 Pandemic in AustraliafaithnicNo ratings yet
- The Incubation Period of Coronavirus Disease 2019 (COVID-19) From Publicly Reported Confirmed Cases Estimation and ApplicationDocument7 pagesThe Incubation Period of Coronavirus Disease 2019 (COVID-19) From Publicly Reported Confirmed Cases Estimation and ApplicationIsrael Parra-OrtegaNo ratings yet
- Critical Preparedness, Readiness and Response Actions For COVID-19Document12 pagesCritical Preparedness, Readiness and Response Actions For COVID-19JanNo ratings yet
- The Epidemiological Characteristics of The COVID-19 Pandemic in Europe: Focus On ItalyDocument14 pagesThe Epidemiological Characteristics of The COVID-19 Pandemic in Europe: Focus On ItalyAmbika SuwalNo ratings yet
- Critical Preparedness, Readiness and Response ActionsDocument13 pagesCritical Preparedness, Readiness and Response Actionssusikaran1981No ratings yet
- Technical Brief and Priority Action On OmicronDocument8 pagesTechnical Brief and Priority Action On OmicronABC Action NewsNo ratings yet
- Asymptotic Estimates of Sars-Cov-2 Infection Counts and Their Sensitivity To Stochastic PerturbationDocument11 pagesAsymptotic Estimates of Sars-Cov-2 Infection Counts and Their Sensitivity To Stochastic PerturbationenocsigalNo ratings yet
- COVID-19: Pathophysiology of Acute Disease 1: SeriesDocument21 pagesCOVID-19: Pathophysiology of Acute Disease 1: SeriesMyatnoe KhinNo ratings yet
- Tlrhwesternpacific D 21 00438 ReviewerDocument19 pagesTlrhwesternpacific D 21 00438 ReviewerMinh Quang NguyenNo ratings yet
- COVID-19: Pathophysiology of Acute Disease 1: SeriesDocument20 pagesCOVID-19: Pathophysiology of Acute Disease 1: SerieswiwiNo ratings yet
- Pi Is 0140673620326258Document2 pagesPi Is 0140673620326258Erjon DervishiNo ratings yet
- SEARO Technical Brief and Priority Action On Omicron V2.1Document8 pagesSEARO Technical Brief and Priority Action On Omicron V2.1Dewi PrabawatiNo ratings yet
- Covid 19Document10 pagesCovid 19Adi Alphena100% (6)
- Evidence For Pre-Symptomatic Transmission of Coronavirus Disease 2019 (COVID-19) in ChinaDocument8 pagesEvidence For Pre-Symptomatic Transmission of Coronavirus Disease 2019 (COVID-19) in ChinaFatrina Maha DewiNo ratings yet
- Coronavirus: Arm Yourself With Facts: Symptoms, Modes of Transmission, Prevention & TreatmentFrom EverandCoronavirus: Arm Yourself With Facts: Symptoms, Modes of Transmission, Prevention & TreatmentRating: 5 out of 5 stars5/5 (1)
- Concepts in Disaster MedicineDocument8 pagesConcepts in Disaster MedicinedaniaNo ratings yet
- Controlling The Transmission Dynamics of COVID-19Document13 pagesControlling The Transmission Dynamics of COVID-19Santos QuezadaNo ratings yet
- Journal Pone 0249090Document11 pagesJournal Pone 0249090Syed Rehan AghaNo ratings yet
- Public Health Criteria To Adjust Public Health and Social Measures in The Context of COVID-19Document4 pagesPublic Health Criteria To Adjust Public Health and Social Measures in The Context of COVID-19Diva CarissaNo ratings yet
- 2021 PSL CovidDocument10 pages2021 PSL CovidRalph Gerard SangalangNo ratings yet
- Corona Virus DiseaseDocument6 pagesCorona Virus DiseaseSAKET MEHTANo ratings yet
- One Health: COVID-19 and GlobalizationDocument4 pagesOne Health: COVID-19 and GlobalizationCarlos CanceladoNo ratings yet
- Journal Pre-Proof: Science of The Total EnvironmentDocument47 pagesJournal Pre-Proof: Science of The Total EnvironmentMohammed Shuaib AhmedNo ratings yet
- Strategies For The Surveillance of COVID-19: BackgroundDocument7 pagesStrategies For The Surveillance of COVID-19: BackgroundJovie Anne CabangalNo ratings yet
- Genetic Evidence For The Association Between COVID-19 Epidemic Severity and Timing of Non-Pharmaceutical InterventionsDocument7 pagesGenetic Evidence For The Association Between COVID-19 Epidemic Severity and Timing of Non-Pharmaceutical InterventionsLaurin LibudaNo ratings yet
- BernasDocument17 pagesBernasYezekael Sebastian QuintinusNo ratings yet
- Coronavirus: A Guide to Understanding the Virus and What is Known So FarFrom EverandCoronavirus: A Guide to Understanding the Virus and What is Known So FarNo ratings yet
- Fimmu 13 782198Document11 pagesFimmu 13 782198Suryati HusinNo ratings yet
- COVID-19 SIR Model Predicts Peak and Herd ImmunityDocument16 pagesCOVID-19 SIR Model Predicts Peak and Herd ImmunityAziz MissaouiNo ratings yet
- Epidemiological Screening - Covid 19Document9 pagesEpidemiological Screening - Covid 19Angela ReyesNo ratings yet
- Coronavirus (COVID-19) Outbreak: What The Department of Endoscopy Should KnowDocument6 pagesCoronavirus (COVID-19) Outbreak: What The Department of Endoscopy Should KnowswabrijNo ratings yet
- Science Abb4557 Full PDFDocument8 pagesScience Abb4557 Full PDFANANo ratings yet
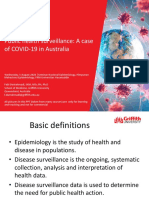
- Public health surveillance of Australia's first COVID-19 caseDocument31 pagesPublic health surveillance of Australia's first COVID-19 caseNurkhalisah HarisNo ratings yet
- Coronavirus Disease 2019 (COVID-19) - UpToDateDocument43 pagesCoronavirus Disease 2019 (COVID-19) - UpToDateGloria MiramontesNo ratings yet
- The Covid 19 Pandemic in EuropeDocument18 pagesThe Covid 19 Pandemic in EuropeMalcolm WillsNo ratings yet
- Guidance For Surveillance of Sars-Cov-2 VariantsDocument18 pagesGuidance For Surveillance of Sars-Cov-2 VariantsSelfa YunitaNo ratings yet
- Hysteroscopy in COVID-19 TimesDocument5 pagesHysteroscopy in COVID-19 TimesHernan PettorossiNo ratings yet
- Coronavirus Disease 2019 (COVID-19)Document27 pagesCoronavirus Disease 2019 (COVID-19)Mateus SchulzNo ratings yet
- 1268 2310 1 SMDocument6 pages1268 2310 1 SMHeru Sutanto KNo ratings yet
- Everything You Should Know About the Coronavirus: How it Spreads, Symptoms, Prevention & Treatment, What to Do if You are Sick, Travel InformationFrom EverandEverything You Should Know About the Coronavirus: How it Spreads, Symptoms, Prevention & Treatment, What to Do if You are Sick, Travel InformationNo ratings yet
- A Time-Dependent SIR Model For COVID-19 With Undetectable Infected PersonsDocument10 pagesA Time-Dependent SIR Model For COVID-19 With Undetectable Infected PersonsNkoda NkodeNo ratings yet
- Controlo Da Pandemia em Portugal Na Fase Da VacinaçãoDocument15 pagesControlo Da Pandemia em Portugal Na Fase Da VacinaçãopedromelaoNo ratings yet
- Transmission of SARS-CoV-2 Required Developments IDocument8 pagesTransmission of SARS-CoV-2 Required Developments IDANILO ROSA NUNESNo ratings yet
- Construction of Compartmental Models For COVID-19 With Quarantine, Lockdown and Vaccine InterventionsDocument16 pagesConstruction of Compartmental Models For COVID-19 With Quarantine, Lockdown and Vaccine InterventionsMahmoudAboAlSamenNo ratings yet
- Covid 19Document9 pagesCovid 19Dagi AbebawNo ratings yet
- 2020 Flu Prevention TipsDocument1 page2020 Flu Prevention TipsBobo RGVNo ratings yet
- 4 Seasons of Electrical Safety Activity ToolkitDocument14 pages4 Seasons of Electrical Safety Activity ToolkitBobo RGVNo ratings yet
- First Aid Manual: Occupational First Aid Module Code D20188 Qqi Fetac Level 5 Rob RoeDocument10 pagesFirst Aid Manual: Occupational First Aid Module Code D20188 Qqi Fetac Level 5 Rob RoeBobo RGVNo ratings yet
- Safe or Not Safe Activity SheetDocument1 pageSafe or Not Safe Activity SheetBobo RGVNo ratings yet
- Purtarea MastiiDocument7 pagesPurtarea MastiiBobo RGVNo ratings yet
- COVID-19 S.W.O.T. AnalysisDocument8 pagesCOVID-19 S.W.O.T. AnalysisBobo RGVNo ratings yet
- Strengths, Weaknesses, Opportunities and Threats (SWOT) Analysis of China's Prevention and Control Strategy For The COVID-19 EpidemicDocument17 pagesStrengths, Weaknesses, Opportunities and Threats (SWOT) Analysis of China's Prevention and Control Strategy For The COVID-19 EpidemicErik OliveiraNo ratings yet
- COVID-19 S.W.O.T. AnalysisDocument8 pagesCOVID-19 S.W.O.T. AnalysisBobo RGVNo ratings yet
- Sewing Safety ChecklistDocument1 pageSewing Safety ChecklistBobo RGVNo ratings yet
- Taller de Calor EstDocument2 pagesTaller de Calor EstDiegoMuñozNo ratings yet
- VCTA-S810 OnlineDocument3 pagesVCTA-S810 OnlineqwUENo ratings yet
- Olympian G60F1 G75F1 Spec SheetDocument6 pagesOlympian G60F1 G75F1 Spec Sheetkman548No ratings yet
- Races of HyruleDocument99 pagesRaces of HyruleScrindlemorpNo ratings yet
- LugeonDocument13 pagesLugeonRojan MaghsoodifarNo ratings yet
- InglesDocument6 pagesInglesyarilisNo ratings yet
- Mineral Resources: Earth ScienceDocument20 pagesMineral Resources: Earth ScienceRegina Mae Narciso NazarenoNo ratings yet
- Goody Anthropology of Sensess and Sensations LRF 2002 45 PDFDocument13 pagesGoody Anthropology of Sensess and Sensations LRF 2002 45 PDFAntroVirtualNo ratings yet
- RTC Invoice 2965 Gj29es2223100505Document1 pageRTC Invoice 2965 Gj29es2223100505Alok PandeyNo ratings yet
- Manual Liebert PSADocument12 pagesManual Liebert PSAMatthew CannonNo ratings yet
- Theme ParkDocument30 pagesTheme ParksassydhineNo ratings yet
- Telemecanique Integral 32 Motor StarterDocument52 pagesTelemecanique Integral 32 Motor StarterJaime IxtaNo ratings yet
- Postdoctoral Research Associate in Functional Organic MaterialsDocument6 pagesPostdoctoral Research Associate in Functional Organic MaterialsTheo GazisNo ratings yet
- 986.33 Mesofilos Aerobios-PetrifilmDocument1 page986.33 Mesofilos Aerobios-PetrifilmBleidy NieblesNo ratings yet
- Compact and Efficient: Rotary KilnsDocument4 pagesCompact and Efficient: Rotary KilnsNhaca100% (1)
- Cold Rolled Steel Sections - Specification: Kenya StandardDocument21 pagesCold Rolled Steel Sections - Specification: Kenya StandardPEng. Tech. Alvince KoreroNo ratings yet
- KGP HG-3Document2 pagesKGP HG-3Lau VillarrealNo ratings yet
- List of Osho's Complete Audio-Video DVD CollectionDocument15 pagesList of Osho's Complete Audio-Video DVD CollectionOsho Bengaluru100% (2)
- Technical Standards for Luxury HotelsDocument173 pagesTechnical Standards for Luxury HotelsHoangDung LeNo ratings yet
- Math10 Q2 Mod24 WritingtheEquationofaCircleandDeterminingtheCenterandRadiusofaCircle V3-1Document19 pagesMath10 Q2 Mod24 WritingtheEquationofaCircleandDeterminingtheCenterandRadiusofaCircle V3-1Bridget SaladagaNo ratings yet
- ClientleDocument1 pageClientleRaghvendra ManiNo ratings yet
- History of Nano FiltrationDocument42 pagesHistory of Nano FiltrationKieran Sexton100% (2)
- CAS circuit analysis simulationDocument9 pagesCAS circuit analysis simulationIan MejiaNo ratings yet
- Coraline: by Neil GaimanDocument5 pagesCoraline: by Neil Gaimanfeliz juevesNo ratings yet
- New Correlations For Predicting Two Phase Electrical SubmersibleDocument11 pagesNew Correlations For Predicting Two Phase Electrical SubmersibleNicolás Ruiz FuentesNo ratings yet
- BS SMP 7-8-9 Bab B. Inggris Sec. Text (Reading) (SB - Descriptive Text)Document5 pagesBS SMP 7-8-9 Bab B. Inggris Sec. Text (Reading) (SB - Descriptive Text)TeresaAvilla Ayuning BudiCayestuNo ratings yet
- Id Card SoftwareDocument6 pagesId Card SoftwareAlli RaniNo ratings yet
- Level 2 Repair: 7-1. Components On The Rear CaseDocument8 pagesLevel 2 Repair: 7-1. Components On The Rear CaseNguyễn Duy LinhNo ratings yet
- Quality Testing of Honey StandardsDocument33 pagesQuality Testing of Honey StandardsK. N RaoNo ratings yet
- Bai Tap Tieng Anh Lop 8 Unit 7 Environmental Protection Global SuccessDocument8 pagesBai Tap Tieng Anh Lop 8 Unit 7 Environmental Protection Global Successngtrmm1No ratings yet