You might also like
- Control of Dynamic Stall Over A NACA 0015 Airfoil Using Plasma ActuatorsDocument13 pagesControl of Dynamic Stall Over A NACA 0015 Airfoil Using Plasma ActuatorsAli AlaviNo ratings yet
- Convergence Acceleration of Fluid Dynamics Solvers Using A Reduced-Order ModelDocument14 pagesConvergence Acceleration of Fluid Dynamics Solvers Using A Reduced-Order ModelAli AlaviNo ratings yet
- Determination of Acoustic Impedance For Helmholtz Resonators Through Incompressible Unsteady Flow SimulationsDocument10 pagesDetermination of Acoustic Impedance For Helmholtz Resonators Through Incompressible Unsteady Flow SimulationsAli AlaviNo ratings yet
- 1 s2.0 S0022534714029450 MainDocument7 pages1 s2.0 S0022534714029450 MainAli AlaviNo ratings yet
- Journal of Infection: Letter To The EditorDocument4 pagesJournal of Infection: Letter To The EditorAli AlaviNo ratings yet
- Journal of Virological MethodsDocument6 pagesJournal of Virological MethodsAli AlaviNo ratings yet
- American Journal of Infection Control: Practice ForumDocument5 pagesAmerican Journal of Infection Control: Practice ForumAli AlaviNo ratings yet
- Evaluating The Relevance of Aeroallergen Sensitization in Atopic Eczema With The Atopy Patch Test: A Randomized, Double-Blind Multicenter StudyDocument7 pagesEvaluating The Relevance of Aeroallergen Sensitization in Atopic Eczema With The Atopy Patch Test: A Randomized, Double-Blind Multicenter StudyAli AlaviNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailssumandeepNo ratings yet
- The New Jersey Freedom of Reproductive Choice ActDocument5 pagesThe New Jersey Freedom of Reproductive Choice ActKristina KoppeserNo ratings yet
- Sample Induction Ceremony ProgramDocument2 pagesSample Induction Ceremony ProgramCalebhe1No ratings yet
- Understanding OsteoporosisDocument6 pagesUnderstanding OsteoporosisPriyank GuptaNo ratings yet
- Smoking and The Skin: Review ArticleDocument12 pagesSmoking and The Skin: Review ArticleAngie BecerraNo ratings yet
- Iodine ParasitesDocument11 pagesIodine Parasitesemilyjdavies1880No ratings yet
- Protocols For High-Risk Pregnancies - 2010 - Queenan - Appendix B Laboratory Values in Normal PregnancyDocument9 pagesProtocols For High-Risk Pregnancies - 2010 - Queenan - Appendix B Laboratory Values in Normal PregnancyHenry VillarosaNo ratings yet
- Hip Rotator ReleasesDocument6 pagesHip Rotator ReleasesAryan KarkiNo ratings yet
- Esthetic Dentistry: Developments inDocument19 pagesEsthetic Dentistry: Developments inAli FaridiNo ratings yet
- Home Exercise Program: Supine Hip Abduction - Elastic Band Clams - ClamshellDocument2 pagesHome Exercise Program: Supine Hip Abduction - Elastic Band Clams - ClamshellkhushmitNo ratings yet
- Final ResearchDocument14 pagesFinal ResearchClarixcNo ratings yet
- Syllabus For Medical MicrobiologyDocument5 pagesSyllabus For Medical MicrobiologyShaik Gouse BashaNo ratings yet
- List of Accredited Hospital and Healthcare Consultant OrganizationsDocument4 pagesList of Accredited Hospital and Healthcare Consultant OrganizationsRafikul RahemanNo ratings yet
- CHAPTER 2 Thesis FileDocument4 pagesCHAPTER 2 Thesis FileArveeh AvilesNo ratings yet
- How To Use This Competency - Based Learning MaterialDocument11 pagesHow To Use This Competency - Based Learning MaterialEmelson VertucioNo ratings yet
- Below Limit Options Are Per Person in AED: Family Care Product #N/ADocument4 pagesBelow Limit Options Are Per Person in AED: Family Care Product #N/AcmthebossNo ratings yet
- CG 501 CH 5 Human Development TheoriesDocument12 pagesCG 501 CH 5 Human Development TheoriesHonshuNo ratings yet
- 16 Early Signs of Autismx16 Months ChecklistDocument1 page16 Early Signs of Autismx16 Months ChecklistGtd Cdis CcsnNo ratings yet
- New Indus Pro21 - 071130Document30 pagesNew Indus Pro21 - 071130Rj GamingNo ratings yet
- What Is An Accident and Why Should It Be Investigated?Document10 pagesWhat Is An Accident and Why Should It Be Investigated?Nanang RizalNo ratings yet
- P.E 3A Learning Activity Sheet WEEK 5 6Document7 pagesP.E 3A Learning Activity Sheet WEEK 5 6Ris CorreaNo ratings yet
- 2014 Edwards Schemas in Clinical PracticeDocument5 pages2014 Edwards Schemas in Clinical PracticeDavid EdwardsNo ratings yet
- Flavonoid Antioxidants: Chemistry, Metabolism and Structure-Activity Relationships. J. Nutr. Biochem. 13: 572-584Document14 pagesFlavonoid Antioxidants: Chemistry, Metabolism and Structure-Activity Relationships. J. Nutr. Biochem. 13: 572-584Stefania CristinaNo ratings yet
- McAndrew, Leske 2019Document17 pagesMcAndrew, Leske 2019Adriana SerratoNo ratings yet
- FIFA Session Plan Grassroots 046Document3 pagesFIFA Session Plan Grassroots 046Mr. Yaasiin IssimdarNo ratings yet
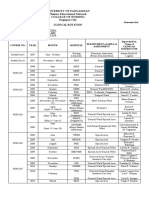
- UPang-PEN CN New Clinical RotationDocument4 pagesUPang-PEN CN New Clinical Rotationbernpastoral7351No ratings yet
- Developing An Effective PlanDocument158 pagesDeveloping An Effective PlanAlex BullandayNo ratings yet
- Can't Eat, Won't EatDocument2 pagesCan't Eat, Won't EatMark HayesNo ratings yet
- Coordination Abilities in Volleyball Coordination Abilities in VolleyballDocument88 pagesCoordination Abilities in Volleyball Coordination Abilities in VolleyballKlgo. Fernando HuertaNo ratings yet
- A Technical Guide - Cannabis, Related Products and Control MechanismsDocument46 pagesA Technical Guide - Cannabis, Related Products and Control MechanismsSteffen JenterNo ratings yet