You might also like
- The Qualitative Estimation of BCR-ABL Transcript: An In-Lab Procedural Study on Leukemia PatientsFrom EverandThe Qualitative Estimation of BCR-ABL Transcript: An In-Lab Procedural Study on Leukemia PatientsNo ratings yet
- Myeloproliferative DisorderDocument36 pagesMyeloproliferative DisorderKalpana ShahNo ratings yet
- Hematology Physiology 1Document6 pagesHematology Physiology 1Kyoheirwe vanessaNo ratings yet
- Acute Myeloid LeukaemiaDocument30 pagesAcute Myeloid Leukaemiajismi vallachiraNo ratings yet
- Top 5 Leukogram PatternsDocument3 pagesTop 5 Leukogram PatternsSandraHermosilloNo ratings yet
- Pathology Lecture 2nd CourseDocument128 pagesPathology Lecture 2nd CourseAbdullah EssaNo ratings yet
- Acute Lymphoid Leukemia (ALL) Develops Rapidly. The Symptoms Include AnemiaDocument5 pagesAcute Lymphoid Leukemia (ALL) Develops Rapidly. The Symptoms Include AnemiaSUTHANNo ratings yet
- Leukemia Lymphoma Skin Cancer - RubioDocument22 pagesLeukemia Lymphoma Skin Cancer - Rubiochristian pulmonesNo ratings yet
- Chronic Myeloid Leukemia DiagnosisDocument4 pagesChronic Myeloid Leukemia DiagnosisKarl Jimenez SeparaNo ratings yet
- Chronic Myeloid LeukaemiaDocument27 pagesChronic Myeloid Leukaemiaنواف الزهرانيNo ratings yet
- ML: AML Without Maturation M2: AML With Maturation M3: M4: M5: M6Document8 pagesML: AML Without Maturation M2: AML With Maturation M3: M4: M5: M6Isak ShatikaNo ratings yet
- CMLDocument8 pagesCMLRachel RiordanNo ratings yet
- 3 s2.0 B9780702066962000230 MainDocument14 pages3 s2.0 B9780702066962000230 MainKate ClarksonNo ratings yet
- Simulators of Malignancy in Bone MarrowDocument12 pagesSimulators of Malignancy in Bone Marrowlavisha.s.punjabiNo ratings yet
- Chronic Leukemia: Carlos Alfredo Cedeño RodríguezDocument24 pagesChronic Leukemia: Carlos Alfredo Cedeño RodríguezCarlos CedeñoNo ratings yet
- Leucocytic DisordersDocument142 pagesLeucocytic DisordersBahaa ShaabanNo ratings yet
- Nucleated Rbcs-Significance in The Peripheral Blood Film: H He em Ma at To Ol Lo Og Gy YDocument7 pagesNucleated Rbcs-Significance in The Peripheral Blood Film: H He em Ma at To Ol Lo Og Gy YFede0No ratings yet
- L-1-2Benign Leukocyte DisordersDocument60 pagesL-1-2Benign Leukocyte DisordersAbood dot netNo ratings yet
- ClassificationDocument16 pagesClassificationpieterinpretoria391No ratings yet
- Haematopathology 3:: Leucocytosis/LeucopeniaDocument113 pagesHaematopathology 3:: Leucocytosis/LeucopeniaarwaNo ratings yet
- Temelash Terefe TeshkolaDocument10 pagesTemelash Terefe TeshkolabirukNo ratings yet
- White Blood Cells (WBCS)Document31 pagesWhite Blood Cells (WBCS)T NNo ratings yet
- Acute Lymphoblastic Leukemia (ALL) TreatmentDocument10 pagesAcute Lymphoblastic Leukemia (ALL) TreatmentAndreea TudurachiNo ratings yet
- Chronic Myeloid LeukaemiaDocument30 pagesChronic Myeloid Leukaemiajismi vallachiraNo ratings yet
- Myeloproliferative Disorders (Bhs Inggris)Document57 pagesMyeloproliferative Disorders (Bhs Inggris)Denny DedenNo ratings yet
- Chronic Lymphocytic LeukemiaDocument2 pagesChronic Lymphocytic LeukemiashaguftaNo ratings yet
- Hyperleukocytosis and Leukostasis in Hematologic MalignanciesDocument9 pagesHyperleukocytosis and Leukostasis in Hematologic Malignanciessoclose1200No ratings yet
- The LeukemiasDocument52 pagesThe Leukemiasمصطفي خندقاوي100% (1)
- Sec6 2 PDFDocument2 pagesSec6 2 PDFIberisNo ratings yet
- Disorders of White Blood: CellsDocument2 pagesDisorders of White Blood: CellsIberisNo ratings yet
- Hema Patho Q&aDocument24 pagesHema Patho Q&akamaluNo ratings yet
- Hemostasis Disorders in LeukemiaDocument14 pagesHemostasis Disorders in LeukemiaNurul HidayahNo ratings yet
- Hyperleukocytosis and Leukostasis in Hematologic MalignanciesDocument17 pagesHyperleukocytosis and Leukostasis in Hematologic MalignanciesAna María Díaz MedinaNo ratings yet
- Patho of Hema Q&aDocument141 pagesPatho of Hema Q&akamaluNo ratings yet
- Non Neoplastic WBC DisordersDocument13 pagesNon Neoplastic WBC DisordersSheikh UzairNo ratings yet
- Leucemia Linfoblástica Aguda - ScienceDirectDocument33 pagesLeucemia Linfoblástica Aguda - ScienceDirectKarol CastroNo ratings yet
- Young Man with Bruising Diagnosed with Acute Lymphoblastic Leukaemia (ALLDocument4 pagesYoung Man with Bruising Diagnosed with Acute Lymphoblastic Leukaemia (ALLRayNo ratings yet
- Praktikum MDTDocument16 pagesPraktikum MDTnanda andhyka100% (1)
- Neutrophilic Leukocytosis, Neutropenia, Monocytosis, and MonocytopeniaDocument7 pagesNeutrophilic Leukocytosis, Neutropenia, Monocytosis, and MonocytopeniaRom ÁlvNo ratings yet
- AML & ALL PresentationDocument74 pagesAML & ALL Presentationkhadija Habib100% (1)
- Chronic Myeloid Leukemia (CML) Is A Form of Leukemia CharacterizedDocument4 pagesChronic Myeloid Leukemia (CML) Is A Form of Leukemia CharacterizedbassamhematolNo ratings yet
- MRCPCH Guide Heme: A Hypochromic MicrocyticDocument8 pagesMRCPCH Guide Heme: A Hypochromic MicrocyticRajiv KabadNo ratings yet
- Malignant or Benign Leukocytosis: Tracy I. GeorgeDocument10 pagesMalignant or Benign Leukocytosis: Tracy I. GeorgeirdinamarchsyaNo ratings yet
- Non Neoplastic WBC DisordersDocument17 pagesNon Neoplastic WBC Disordersdr100% (1)
- Hyperleukocytosis and leukostasis in hematologic malignanciesDocument13 pagesHyperleukocytosis and leukostasis in hematologic malignanciesIGD RSKDNo ratings yet
- Lab 1: The Hematopoietic System - Clinical CasesDocument6 pagesLab 1: The Hematopoietic System - Clinical Casesdr_4uNo ratings yet
- Anemi Aplastik Dan MielodisplasiaDocument34 pagesAnemi Aplastik Dan MielodisplasiaRoby KieranNo ratings yet
- Lecture 5 White Cell DisordersDocument17 pagesLecture 5 White Cell DisordersOsama MalikNo ratings yet
- 1st Lect in Hem-2021-Dr - HazimDocument5 pages1st Lect in Hem-2021-Dr - HazimAnmarNo ratings yet
- WBC BasicsDocument70 pagesWBC BasicsZoe ZillaNo ratings yet
- AML: Acute Myeloblastic LeukemiaDocument23 pagesAML: Acute Myeloblastic Leukemiaد. أمجد حسين عبد الرحمنNo ratings yet
- Chapter 4 - Hematological MalignanciesDocument99 pagesChapter 4 - Hematological MalignanciesAemro TadeleNo ratings yet
- leukemiaDocument13 pagesleukemiaBenjamin VanlaltlansangaNo ratings yet
- Acute Myeloid Leukemia-BookDocument15 pagesAcute Myeloid Leukemia-BookRhoda Lom-ocNo ratings yet
- Acute Leukemia RodaksDocument14 pagesAcute Leukemia RodaksLoiLoiChanNo ratings yet
- An Overview of Clinical PathologyDocument9 pagesAn Overview of Clinical PathologyaymenNo ratings yet
- Lab Le2 PortionDocument291 pagesLab Le2 PortionshreyanshNo ratings yet
- Chronic Lymphocytic LeukemiaFrom EverandChronic Lymphocytic LeukemiaMichael HallekNo ratings yet
- Impact Factor For 2017 Is 2.229 Journal Is Indexed With MED: Click Here To View Optimized Website For Mobile DevicesDocument8 pagesImpact Factor For 2017 Is 2.229 Journal Is Indexed With MED: Click Here To View Optimized Website For Mobile DevicesChaira Alkanzi DjeniNo ratings yet
- p1004 PDFDocument8 pagesp1004 PDFMarisa IzzaNo ratings yet
- DM Tipe 1 AnakDocument13 pagesDM Tipe 1 AnakChaira Alkanzi DjeniNo ratings yet
- Circulating Purine Compounds, Uric Acid, and Xanthine Oxidase PDFDocument6 pagesCirculating Purine Compounds, Uric Acid, and Xanthine Oxidase PDFAnonymous vCmWtNOsNo ratings yet
- MR 8 April 2018Document26 pagesMR 8 April 2018Chaira Alkanzi DjeniNo ratings yet
- Pneumonia or Sepsis in Adults Associated With Increased Risk of Cardiovascular Disease - ScienceDailyDocument3 pagesPneumonia or Sepsis in Adults Associated With Increased Risk of Cardiovascular Disease - ScienceDailyChaira Alkanzi DjeniNo ratings yet
- Oral Lichen Planus: An Overview of Potential Risk Factors, Biomarkers and TreatmentsDocument7 pagesOral Lichen Planus: An Overview of Potential Risk Factors, Biomarkers and Treatmentsdira firliandaNo ratings yet
- Swapan Kumar Nath Sanjay G Revankar Problem-Based PDFDocument1,163 pagesSwapan Kumar Nath Sanjay G Revankar Problem-Based PDFRestu100% (1)
- Communicable Disease SurveillanceDocument60 pagesCommunicable Disease SurveillanceAmeer MuhammadNo ratings yet
- Clinical Efficacy and Safety of Meropenem in The Treatment of Severe Neonatal Bacterial Infectious PneumoniaDocument6 pagesClinical Efficacy and Safety of Meropenem in The Treatment of Severe Neonatal Bacterial Infectious PneumoniaI Made AryanaNo ratings yet
- The Blood PoisonersDocument45 pagesThe Blood Poisonersgreatha marmalNo ratings yet
- Infectious Disease Causes, Transmission, and PreventionDocument15 pagesInfectious Disease Causes, Transmission, and Preventioncylon3No ratings yet
- Pandemic Preparedness PlanDocument40 pagesPandemic Preparedness PlanMurali Vallipuranathan100% (2)
- Reference 1. Satyanarayanajois, S., Stephanie, V., Liu, J., Go, M.L., 2009, Design, Synthesis, and Docking Studies ofDocument1 pageReference 1. Satyanarayanajois, S., Stephanie, V., Liu, J., Go, M.L., 2009, Design, Synthesis, and Docking Studies ofScholastika Palayukan100% (1)
- Infection Control in Burns PatietnsDocument41 pagesInfection Control in Burns Patietnstummalapalli venkateswara raoNo ratings yet
- Emailing DOC-20221210-WA0012.Document1 pageEmailing DOC-20221210-WA0012.JAHIR HASANNo ratings yet
- Predictors of Unfavorable Treatment Outcome Among Childhood Tuberculosis Patients in Ede Town Health Centers, Sub-District of Osun, NigeriaDocument10 pagesPredictors of Unfavorable Treatment Outcome Among Childhood Tuberculosis Patients in Ede Town Health Centers, Sub-District of Osun, NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- XN Series: Case InterpretationDocument41 pagesXN Series: Case InterpretationTanveerNo ratings yet
- Quiz MapehDocument15 pagesQuiz MapehCher ReignNo ratings yet
- Compartmental Model For Chlamydia, A Sexually Transmitted DiseaseDocument22 pagesCompartmental Model For Chlamydia, A Sexually Transmitted DiseaseInstituto de Investigaciones InterdisciplinariasNo ratings yet
- Provincial Disease Surveillance and Response Unit PDSRU - FELTP Quetta BalochistanDocument17 pagesProvincial Disease Surveillance and Response Unit PDSRU - FELTP Quetta BalochistanehsanlarikNo ratings yet
- Sexually Transmitted Infections or Diseases (Stis or STDS) : Last Updated: July 20, 2021Document28 pagesSexually Transmitted Infections or Diseases (Stis or STDS) : Last Updated: July 20, 2021RiteshNo ratings yet
- Melioidosis PDFDocument11 pagesMelioidosis PDFVictor AldeaNo ratings yet
- Examining Immune System ResponsesDocument18 pagesExamining Immune System Responseswhitewave25No ratings yet
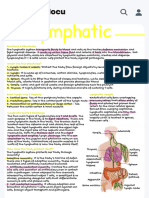
- Handwritten Lympathic - Functions & Structures The Lymphatic System Transports Fluids To Blood - StudocuDocument1 pageHandwritten Lympathic - Functions & Structures The Lymphatic System Transports Fluids To Blood - StudocuAllyssa MarieNo ratings yet
- Zanki MicroDocument584 pagesZanki MicrokikocornholioNo ratings yet
- Experiment 7: RH Typing (Tube Method) : Pre-Analytical PhaseDocument4 pagesExperiment 7: RH Typing (Tube Method) : Pre-Analytical PhasesummerNo ratings yet
- Laporan Harian Pasien Puskesmas JatinegaraDocument8 pagesLaporan Harian Pasien Puskesmas JatinegaraanggaNo ratings yet
- Summary of Recommendations For Adult Immunization: (Age 19 Years & Older)Document4 pagesSummary of Recommendations For Adult Immunization: (Age 19 Years & Older)enquzerNo ratings yet
- Syphilis Recognition Description and DiagnosisDocument138 pagesSyphilis Recognition Description and DiagnosisCelta Gómez TrejoNo ratings yet
- Emerging Infectious Diseases - Vol. 14Document167 pagesEmerging Infectious Diseases - Vol. 14rvcf100% (1)
- Immunology of Head and NeckDocument376 pagesImmunology of Head and NecksrisaivimalaNo ratings yet
- Idiopathic Thrombocytopenic PurpuraDocument10 pagesIdiopathic Thrombocytopenic PurpuramariakolandaNo ratings yet
- Complement SystemDocument4 pagesComplement SystemFait HeeNo ratings yet
- STIs: Common Types, Symptoms and PreventionDocument100 pagesSTIs: Common Types, Symptoms and PreventionEstrella M. Ramirez-Lawas100% (1)
- Neisseria Acinetobacter Baumanii: Moraxella CatarrhalisDocument39 pagesNeisseria Acinetobacter Baumanii: Moraxella Catarrhalissilvia_buruNo ratings yet