You might also like
- Falagas 2013 (CRE)Document11 pagesFalagas 2013 (CRE)Nattawat TeerawattanapongNo ratings yet
- Ofac 034Document6 pagesOfac 034Imene FlNo ratings yet
- Hrabak 2014Document15 pagesHrabak 2014Ignacio Velasquez MiñoNo ratings yet
- Tamma Et Al., 2015Document7 pagesTamma Et Al., 2015Caio Bonfim MottaNo ratings yet
- Carbapenem Resistant Enterobacteriaceae - StatPearls - NCBI BookshelfDocument9 pagesCarbapenem Resistant Enterobacteriaceae - StatPearls - NCBI BookshelfOG3 PolizuNo ratings yet
- Research Paper BelgiumDocument10 pagesResearch Paper Belgiumyogesh kumarNo ratings yet
- Journal 8Document7 pagesJournal 8margareth silaenNo ratings yet
- Oral Cephalosporin and B-Lactamase Inhibitor Combinations For ESBL-producing Enterobacteriaceae Urinary Tract InfectionsDocument13 pagesOral Cephalosporin and B-Lactamase Inhibitor Combinations For ESBL-producing Enterobacteriaceae Urinary Tract InfectionsJosaphat NuñezNo ratings yet
- Neonatal Infections With Multidrugresistant ESBL-producing E. Cloacae and K. Pneumoniae in Neonatal Units of Two Different Hospitals in Antananarivo, MadagascarDocument10 pagesNeonatal Infections With Multidrugresistant ESBL-producing E. Cloacae and K. Pneumoniae in Neonatal Units of Two Different Hospitals in Antananarivo, MadagascarJulie Jubane TiuNo ratings yet
- Rood 2017Document19 pagesRood 2017Estefany HurtadoNo ratings yet
- Resist Ncia Enterobact Rias PatersonDocument9 pagesResist Ncia Enterobact Rias PatersonDrashua AshuaNo ratings yet
- Carbapenem-Resistant EnterobacteriaceaeDocument16 pagesCarbapenem-Resistant EnterobacteriaceaeOG3 PolizuNo ratings yet
- Carbapenem Resistant EnterobacteriaceaeDocument15 pagesCarbapenem Resistant Enterobacteriaceaeja_sam_radivoje3093No ratings yet
- Antibiotic Resistance Profile and Random AmplificationDocument10 pagesAntibiotic Resistance Profile and Random Amplificationdanish.mahaitNo ratings yet
- Symposium On Antimicrobial Therapy: Souha S. MD, and MDDocument11 pagesSymposium On Antimicrobial Therapy: Souha S. MD, and MDCarolina SalgueroNo ratings yet
- The "Old" and The "New" Antibiotics For MDR Gram-Negative Pathogens: For Whom, When, and HowDocument25 pagesThe "Old" and The "New" Antibiotics For MDR Gram-Negative Pathogens: For Whom, When, and HowntnquynhproNo ratings yet
- Molecular Characterisation of An Acinetobacter Baumannii OutbreakDocument9 pagesMolecular Characterisation of An Acinetobacter Baumannii OutbreakRamón RicardoNo ratings yet
- Emergency Department Urinary Tract InfectionsDocument8 pagesEmergency Department Urinary Tract InfectionsPrimasari DiahNo ratings yet
- Ben Ami ESBL in Community Risk FactorsDocument9 pagesBen Ami ESBL in Community Risk FactorsSIUSANTO HadiNo ratings yet
- Cephalosporin Resistance in Enterobacteriaceae: ESBL DetectionDocument4 pagesCephalosporin Resistance in Enterobacteriaceae: ESBL DetectionGIST (Gujarat Institute of Science & Technology)No ratings yet
- Expert Review of Carbapenem-Sparing Options for ESBL-Producing EnterobacteriaceaeDocument29 pagesExpert Review of Carbapenem-Sparing Options for ESBL-Producing EnterobacteriaceaeCaio Bonfim MottaNo ratings yet
- Perspectives: Antibiotic Resistance Breakers: Can Repurposed Drugs Fill The Antibiotic Discovery Void?Document13 pagesPerspectives: Antibiotic Resistance Breakers: Can Repurposed Drugs Fill The Antibiotic Discovery Void?MedranoReyesLuisinNo ratings yet
- Antibiotic Resistance and Extended Spectrum Beta-Lactamases: Types, Epidemiology and TreatmentDocument35 pagesAntibiotic Resistance and Extended Spectrum Beta-Lactamases: Types, Epidemiology and TreatmentRoby Aditya SuryaNo ratings yet
- Enterobacter Cloacae: Carbapenem-Resistant in Patients From The US Veterans Health Administration, 2006-2015Document3 pagesEnterobacter Cloacae: Carbapenem-Resistant in Patients From The US Veterans Health Administration, 2006-2015Mayang WulanNo ratings yet
- Sheu Et Al., 2018Document15 pagesSheu Et Al., 2018Caio Bonfim MottaNo ratings yet
- Colistina 2Document9 pagesColistina 2Sherly CharleneNo ratings yet
- Antibiotic-resistance-profile-and-random-amplification-typing-of-lactamaseproducing-Enterobacteriaceae-from-the-local-area-of-AlTaif-and-nearby-cities-in-Saudi-Arabia (1)Document10 pagesAntibiotic-resistance-profile-and-random-amplification-typing-of-lactamaseproducing-Enterobacteriaceae-from-the-local-area-of-AlTaif-and-nearby-cities-in-Saudi-Arabia (1)NRR GamingNo ratings yet
- Paterson Et Al., 2021Document3 pagesPaterson Et Al., 2021Caio Bonfim MottaNo ratings yet
- Trabajo 2Document7 pagesTrabajo 2Juan Martín VargasNo ratings yet
- Resistance Mechanisms - United States, 2006-2017: Vital Signs: Containment of Novel Multidrug-Resistant Organisms andDocument6 pagesResistance Mechanisms - United States, 2006-2017: Vital Signs: Containment of Novel Multidrug-Resistant Organisms andKenny HaNo ratings yet
- Global Antimicrobial Resistance in Gram-NegativeDocument7 pagesGlobal Antimicrobial Resistance in Gram-NegativerafaNo ratings yet
- BBRC Vol 14 No 04 2021-69Document7 pagesBBRC Vol 14 No 04 2021-69Dr Sharique AliNo ratings yet
- Ceftobiprole, A Broad-Spectrum Cephalosporin With Activity Against Methicillin-Resistant Staphylococcus Aureus (MRSA)Document7 pagesCeftobiprole, A Broad-Spectrum Cephalosporin With Activity Against Methicillin-Resistant Staphylococcus Aureus (MRSA)Esther TobingNo ratings yet
- Antimicrobial Peptides From Scorpion Venoms PDFDocument23 pagesAntimicrobial Peptides From Scorpion Venoms PDFOrlando Pérez DelgadoNo ratings yet
- Trabajo 2Document7 pagesTrabajo 2Juan Martín VargasNo ratings yet
- 2JMAA-8-12 - 2015sharma PDFDocument5 pages2JMAA-8-12 - 2015sharma PDFAMBS ABMS JMAANo ratings yet
- Jurnal Kesekian Ga Tau BilangDocument10 pagesJurnal Kesekian Ga Tau BilangHalwa Huriya WandaNo ratings yet
- Prevalence of ESBL-Producing Enterobacteriaceae in Saudi HospitalDocument4 pagesPrevalence of ESBL-Producing Enterobacteriaceae in Saudi HospitalMohammad K AlshomraniNo ratings yet
- 480-Article Text-852-1-10-20181031Document15 pages480-Article Text-852-1-10-20181031lalaNo ratings yet
- Karakteristik Resistensi Yang Resisten Karbapenem Pada Beberapa Rumah Sakit Di Indonesia Dan Pemeriksaan LaboratoriumDocument15 pagesKarakteristik Resistensi Yang Resisten Karbapenem Pada Beberapa Rumah Sakit Di Indonesia Dan Pemeriksaan Laboratoriumhikmah sammangNo ratings yet
- Treatment Options For Carbapenem-Resistant Gram-Negative Bacterial InfectionsDocument11 pagesTreatment Options For Carbapenem-Resistant Gram-Negative Bacterial InfectionsCesar Augusto Cardona OspinaNo ratings yet
- 3 Saritanayak EtalDocument7 pages3 Saritanayak EtaleditorijmrhsNo ratings yet
- Xin 2016, Pfge&MlstDocument8 pagesXin 2016, Pfge&MlstSarah KKCNo ratings yet
- Hawkey 2012Document7 pagesHawkey 2012Kavyarani RathodNo ratings yet
- TX Carbapenem Resistent MoDocument11 pagesTX Carbapenem Resistent MoInes MendonçaNo ratings yet
- Detection of ESBLs and NDM-1 genes among urinary Escherichia coli and Klebsiella pneumoniae from healthy students in Niger Delta University, Amassoma, Bayelsa State, NigeriaDocument16 pagesDetection of ESBLs and NDM-1 genes among urinary Escherichia coli and Klebsiella pneumoniae from healthy students in Niger Delta University, Amassoma, Bayelsa State, NigeriaTunde OdetoyinNo ratings yet
- CeftolozaneTazobactam A New Option in The TreatmenDocument7 pagesCeftolozaneTazobactam A New Option in The TreatmenAisyah RohieNo ratings yet
- 1 Isolation and Phenotypic Characterization of Marine PhageDocument40 pages1 Isolation and Phenotypic Characterization of Marine PhageJanine Kate DavidNo ratings yet
- Nrmicro 1789Document13 pagesNrmicro 1789Enrique Aburto ArreguínNo ratings yet
- Bacteremia Due To Bacteroides Fragilis Group: Distribution of Species, - Lactamase Production, and Antimicrobial Susceptibility PatternsDocument6 pagesBacteremia Due To Bacteroides Fragilis Group: Distribution of Species, - Lactamase Production, and Antimicrobial Susceptibility PatternsDdn RmaNo ratings yet
- Daptomycin For The Treatment of Bacteraemia Du - 2014 - International Journal ofDocument9 pagesDaptomycin For The Treatment of Bacteraemia Du - 2014 - International Journal ofPatricio Suazo SotoNo ratings yet
- Antimicrobial Resistance and Molecular Characterization of Gene Cassettes From Class 1 Integrons in Pseudomonas Aeruginosa S PDFDocument7 pagesAntimicrobial Resistance and Molecular Characterization of Gene Cassettes From Class 1 Integrons in Pseudomonas Aeruginosa S PDFValentina RondonNo ratings yet
- Fosfomycin and Comparator Activity Against Select Enterobacteriaceae, Pseudomonas, and Enterococcus Urinary Tract InfectionDocument11 pagesFosfomycin and Comparator Activity Against Select Enterobacteriaceae, Pseudomonas, and Enterococcus Urinary Tract InfectionNawwal NaeemNo ratings yet
- Idr 13 00039Document7 pagesIdr 13 00039siti muthoharohNo ratings yet
- Present and Future of Carbapenem-ResistantDocument16 pagesPresent and Future of Carbapenem-ResistantKenny HaNo ratings yet
- Journal 3Document11 pagesJournal 3margareth silaenNo ratings yet
- Prevalence of Extended Spectrum β-Lactamases in Multi-drug Resistant Pseudomonas aeruginosa from Diabetic Foot PatientsDocument6 pagesPrevalence of Extended Spectrum β-Lactamases in Multi-drug Resistant Pseudomonas aeruginosa from Diabetic Foot Patientskhurry testNo ratings yet
- Current Trends in the Identification and Development of Antimicrobial AgentsFrom EverandCurrent Trends in the Identification and Development of Antimicrobial AgentsNo ratings yet
- 2018 Corticosteroids For The Prevention of BPDDocument7 pages2018 Corticosteroids For The Prevention of BPDmariangelNo ratings yet
- Theuseofcardiotonic Drugsinneonates: Eugene Dempsey,, Heike RabeDocument18 pagesTheuseofcardiotonic Drugsinneonates: Eugene Dempsey,, Heike RabePaty JuárezNo ratings yet
- Referencia Rápida - Control y Seguimiento de LaDocument16 pagesReferencia Rápida - Control y Seguimiento de LaIvan BurgosNo ratings yet
- SFNM Jun 2018 Soul2018Document8 pagesSFNM Jun 2018 Soul2018mariangelNo ratings yet
- Renal Consequences of Therapeutic Interventions in Premature NeonatesDocument8 pagesRenal Consequences of Therapeutic Interventions in Premature NeonatesmariangelNo ratings yet
- Referencia Rápida - Control y Seguimiento de LaDocument16 pagesReferencia Rápida - Control y Seguimiento de LaIvan BurgosNo ratings yet
- SFNM Jun 2018 Soul2018Document8 pagesSFNM Jun 2018 Soul2018mariangelNo ratings yet
- Diabetes 2013Document7 pagesDiabetes 2013jerdhal3515No ratings yet
- Diagnosis and Classification of Diabetes 2013Document8 pagesDiagnosis and Classification of Diabetes 2013Armando ATNo ratings yet
- Renal Consequences of Therapeutic Interventions in Premature NeonatesDocument8 pagesRenal Consequences of Therapeutic Interventions in Premature NeonatesmariangelNo ratings yet
- ADA Standards of Medical Care in Diabetes 2013 PDFDocument56 pagesADA Standards of Medical Care in Diabetes 2013 PDFPatricio Moncayo DonosoNo ratings yet
- DiabetesDocument2 pagesDiabetesRoberto Arteaga-AriasNo ratings yet
- FDAR For Urinary Tract InfectionDocument2 pagesFDAR For Urinary Tract InfectionElle Monge100% (1)
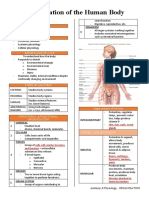
- Organization of the Human BodyDocument8 pagesOrganization of the Human BodyAly HannahNo ratings yet
- Med-Surg Exam #2 Study GuideDocument33 pagesMed-Surg Exam #2 Study GuideCaitlyn BilbaoNo ratings yet
- A Case Study In:: Hirschsprung DiseaseDocument18 pagesA Case Study In:: Hirschsprung DiseaseJaimie La PenaNo ratings yet
- Morphology, Pathogenesis and Lab Diagnosis of Polio VirusDocument12 pagesMorphology, Pathogenesis and Lab Diagnosis of Polio VirusSalu kSNo ratings yet
- GCSE History Britain: Health and The People, C1000-Present DayDocument30 pagesGCSE History Britain: Health and The People, C1000-Present DayAniqah ShujaatNo ratings yet
- Foundations in Microbiology: The Gram-Positive Bacilli of Medical Importance TalaroDocument70 pagesFoundations in Microbiology: The Gram-Positive Bacilli of Medical Importance TalaroAgathaNo ratings yet
- Crystal Violet: Material Safety Data SheetDocument10 pagesCrystal Violet: Material Safety Data SheetIolanda VeronicaNo ratings yet
- Pterygium - EyeWikiDocument1 pagePterygium - EyeWikiPaudel SujanNo ratings yet
- International Journal of Health Sciences and Research: Fetal Umbilical Cord Circumference Measurement and Birth WeightDocument6 pagesInternational Journal of Health Sciences and Research: Fetal Umbilical Cord Circumference Measurement and Birth WeightFatma ElzaytNo ratings yet
- 19 04 2020 Mumbai PDFDocument33 pages19 04 2020 Mumbai PDFShaji VkNo ratings yet
- Ventilasi MekanikDocument47 pagesVentilasi MekanikzahrahNo ratings yet
- Radiobiology For The Radiologist 8th Edition Ebook PDFDocument61 pagesRadiobiology For The Radiologist 8th Edition Ebook PDFroy.mula622100% (40)
- MICROORGANISMS Class 8Document2 pagesMICROORGANISMS Class 8AyushNo ratings yet
- Joseph Murphy Book ReviewsDocument54 pagesJoseph Murphy Book ReviewsDr. Peter Fritz Walter100% (4)
- Bab Vii Daftar PustakaDocument5 pagesBab Vii Daftar Pustaka19 110 Setya Maharani KadirNo ratings yet
- Cardiac Myocytes CultureDocument6 pagesCardiac Myocytes CultureÉmerson MoreiraNo ratings yet
- Oral CandidiasisDocument4 pagesOral CandidiasisAnish RajNo ratings yet
- LEGIT 62 Ako 1RST Quarter Exam PDEV 111 1Document23 pagesLEGIT 62 Ako 1RST Quarter Exam PDEV 111 1Mylen Noel Elgincolin Manlapaz50% (2)
- MolnupiravirDocument7 pagesMolnupiravirConcepStore PyNo ratings yet
- Witches HerbsDocument3 pagesWitches HerbsAM PNo ratings yet
- Final Oxygen Therapy and Monitoring Devices FM CommentedDocument56 pagesFinal Oxygen Therapy and Monitoring Devices FM CommentedDesalegnNo ratings yet
- Perioperative nursing considerationsDocument9 pagesPerioperative nursing considerationsKoleen Kirsten100% (1)
- MPPC Health Indeminity FormDocument2 pagesMPPC Health Indeminity FormmichaelforkcsNo ratings yet
- (Neurology Now Books) Lynne P. Taylor, Alyx B. Porter Umphrey, Diane Richard - Navigating Life With A Brain Tumor-Oxford University Press, USA (2012) PDFDocument214 pages(Neurology Now Books) Lynne P. Taylor, Alyx B. Porter Umphrey, Diane Richard - Navigating Life With A Brain Tumor-Oxford University Press, USA (2012) PDFYutasya TeresaNo ratings yet
- Detection of Cardiac Disorder Using MATLAB BasedDocument4 pagesDetection of Cardiac Disorder Using MATLAB BasedSeira LoyardNo ratings yet
- Zubiaga, R-Jeane S. - BSN 3 - For PlagscanDocument41 pagesZubiaga, R-Jeane S. - BSN 3 - For PlagscanR-Jeane ZubiagaNo ratings yet
- Office Hygiene British English Upper Intermediate Advanced GroupDocument3 pagesOffice Hygiene British English Upper Intermediate Advanced GroupPablo Tejedor LópezNo ratings yet
- Pain Management in Palliative Care: Ns. Dwi Yunita Haryanti, S.Kep., M.KesDocument17 pagesPain Management in Palliative Care: Ns. Dwi Yunita Haryanti, S.Kep., M.Kesiqbal yudo5No ratings yet
- Fall Health & Wellness (October 2022)Document20 pagesFall Health & Wellness (October 2022)Watertown Daily TimesNo ratings yet