You might also like
- Horse Anatomy, A Coloring AtlasDocument185 pagesHorse Anatomy, A Coloring AtlasMartyna MałżNo ratings yet
- BD Chaurasia's Human Anatomy, Volume 2 - Lower Limb, Abdoman and Pelvis, 6th Edition PDFDocument472 pagesBD Chaurasia's Human Anatomy, Volume 2 - Lower Limb, Abdoman and Pelvis, 6th Edition PDFYash Salunkhe86% (22)
- Draw It To Know It NotesDocument13 pagesDraw It To Know It Noteskat9210No ratings yet
- Neuroanatomy - Draw.it - To.know - It.2nd - Ed Parsamed - IrDocument476 pagesNeuroanatomy - Draw.it - To.know - It.2nd - Ed Parsamed - Irexibit1100% (21)
- Stroke: Physiotherapy Treatment ApproachesDocument92 pagesStroke: Physiotherapy Treatment ApproachesHimani Kaushik100% (1)
- Stroke RehabilitationDocument18 pagesStroke RehabilitationJayricDepalobos100% (4)
- (MicroB) Brainstem Lesions - Dr. Bravo (Nico Castillo)Document4 pages(MicroB) Brainstem Lesions - Dr. Bravo (Nico Castillo)miguel cuevasNo ratings yet
- Neurology Passmedicine & Onexamination Notes 2016Document158 pagesNeurology Passmedicine & Onexamination Notes 2016Muhammad Haneef100% (2)
- Localization of Brain Stem LesionsDocument35 pagesLocalization of Brain Stem LesionsHrishikesh Jha0% (1)
- Middle Cerebral ArteryDocument4 pagesMiddle Cerebral Arterykat9210No ratings yet
- Human Anatomy & Physiology Marieb Chapter 1Document6 pagesHuman Anatomy & Physiology Marieb Chapter 1JayjayNo ratings yet
- Intracranial HemorrhageDocument66 pagesIntracranial HemorrhageKaif Khan100% (1)
- Neurology Multiple Choice Questions With Explanations: Volume IIFrom EverandNeurology Multiple Choice Questions With Explanations: Volume IIRating: 5 out of 5 stars5/5 (2)
- Final Stroke MBDocument79 pagesFinal Stroke MBVanessa Yvonne GurtizaNo ratings yet
- SUBarachnoid HemorrhageDocument4 pagesSUBarachnoid Hemorrhagekhadzx100% (2)
- Stroke: Types of Stroke: Ischemic (80%) Hemorrhagic Strokes (20%) and Venous OcclusionsDocument57 pagesStroke: Types of Stroke: Ischemic (80%) Hemorrhagic Strokes (20%) and Venous Occlusionsdrchetanm100% (1)
- Stroke Syndromes (Etiology & Clinical Features)Document40 pagesStroke Syndromes (Etiology & Clinical Features)nisha_m_patel2006No ratings yet
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- Neurologic Emergencies Stroke & Tia: Devin R. Harris, MD MHSC CCFP (Em)Document10 pagesNeurologic Emergencies Stroke & Tia: Devin R. Harris, MD MHSC CCFP (Em)Samantha Lui100% (2)
- Neurology Multiple Choice Questions With Explanations: Volume IIIFrom EverandNeurology Multiple Choice Questions With Explanations: Volume IIIRating: 4.5 out of 5 stars4.5/5 (6)
- Thai Foot Reflexology for Health A Practical Manual คู่มือนวดเท้ากดจุดเพื่อสุขภาพDocument25 pagesThai Foot Reflexology for Health A Practical Manual คู่มือนวดเท้ากดจุดเพื่อสุขภาพศาสตรา คำมุลตรี100% (2)
- Tear Trough LigamentDocument11 pagesTear Trough LigamentSuc Khoe la VangNo ratings yet
- IB Singh - Textbook of Human Osteology, 3rd Edition PDFDocument350 pagesIB Singh - Textbook of Human Osteology, 3rd Edition PDFLi Faung80% (5)
- Seminar: Facial Nerve PalsyDocument166 pagesSeminar: Facial Nerve PalsyShouvik ChowdhuryNo ratings yet
- Filsafat IlmuDocument51 pagesFilsafat Ilmuwulandarimerry100% (1)
- Filsafat IlmuDocument51 pagesFilsafat Ilmuwulandarimerry100% (1)
- Neurology Multiple Choice Questions With Explanations: Volume IFrom EverandNeurology Multiple Choice Questions With Explanations: Volume IRating: 4 out of 5 stars4/5 (7)
- Anatomy and PhysiologyDocument26 pagesAnatomy and PhysiologyJay KennedyNo ratings yet
- Clinical Approach To Brainstem LesionsDocument10 pagesClinical Approach To Brainstem LesionsJosé SánchezNo ratings yet
- Bontrager 9 EdicaoDocument339 pagesBontrager 9 EdicaoGerson Lopes100% (7)
- Horner Syndrome - StatPearls - NCBI BookshelfDocument9 pagesHorner Syndrome - StatPearls - NCBI BookshelfShweh Fern LooNo ratings yet
- Vascular Disorders of The Posterior Circulation - An Anatomico-Clinical OverviewDocument3 pagesVascular Disorders of The Posterior Circulation - An Anatomico-Clinical OverviewSagar GopaniNo ratings yet
- Sindrom HornerDocument15 pagesSindrom HornervivinNo ratings yet
- Stroke Syndromes and Clinical ManagementDocument10 pagesStroke Syndromes and Clinical ManagementCarlos AlvaradoNo ratings yet
- Brainstem Stroke: Anatomy, Clinical and Radiological FindingsDocument11 pagesBrainstem Stroke: Anatomy, Clinical and Radiological FindingsMetta WitariNo ratings yet
- Review: Stroke Syndromes and Clinical ManagementDocument9 pagesReview: Stroke Syndromes and Clinical ManagementheruNo ratings yet
- Slide MusculoDocument19 pagesSlide MusculoStefan CandraNo ratings yet
- Medial Medullary Syndrome - WikipediaDocument8 pagesMedial Medullary Syndrome - WikipediaArun KumarNo ratings yet
- Jugular Foramen Syndrome - StatPearls - NCBI BookshelfDocument9 pagesJugular Foramen Syndrome - StatPearls - NCBI BookshelfJose ColinaNo ratings yet
- Brain TumorsDocument24 pagesBrain TumorsStevina TanuwijayaNo ratings yet
- Middle Cerebral Artery (MCA) Infarction: Jenis Stroke IskemikDocument7 pagesMiddle Cerebral Artery (MCA) Infarction: Jenis Stroke IskemiksarelriskyNo ratings yet
- Epilepsia Lobublo Temporal SND EtmDocument9 pagesEpilepsia Lobublo Temporal SND EtmAndres Rojas JerezNo ratings yet
- Cerebrovascular Disease Lipincott 24 10 2012 FinalDocument10 pagesCerebrovascular Disease Lipincott 24 10 2012 Finalرافت العواضيNo ratings yet
- Neurology Self Directed Learning Target1Document7 pagesNeurology Self Directed Learning Target1turpificatusNo ratings yet
- 10 1016@j Amjmed 2018 03 009Document17 pages10 1016@j Amjmed 2018 03 009pedoNo ratings yet
- Pathology of The Central Nervous System 2A2016Document63 pagesPathology of The Central Nervous System 2A2016Rose AnnNo ratings yet
- Multiple Cranial NeuropathyDocument13 pagesMultiple Cranial NeuropathyChaerani SalamNo ratings yet
- Lesion Del Tracto Cortico - Espinal InglesDocument14 pagesLesion Del Tracto Cortico - Espinal InglesCarolina Andrea Daza CharrisNo ratings yet
- Lecture 3 - Stroke - Highlights On Pathophysiology, Clinical PresentationDocument39 pagesLecture 3 - Stroke - Highlights On Pathophysiology, Clinical Presentationepic sound everNo ratings yet
- Spinal cord lesion (Transverse myelitis) د.رشاد عبدالغنيDocument33 pagesSpinal cord lesion (Transverse myelitis) د.رشاد عبدالغنيMohammad BelbahaithNo ratings yet
- Notes On SyncopeDocument8 pagesNotes On SyncopeViswa Giri100% (1)
- Stroke 1982 Heros 106 9Document5 pagesStroke 1982 Heros 106 9Rika FitriaNo ratings yet
- Giannopoulos PC - AlDocument54 pagesGiannopoulos PC - AlNikosNo ratings yet
- Neuromuscular Handout 2006Document12 pagesNeuromuscular Handout 2006Windy MentariiNo ratings yet
- InTech-Underlying Causes of ParesthesiaDocument21 pagesInTech-Underlying Causes of ParesthesiaPurnaNo ratings yet
- Horner's SyndromeDocument7 pagesHorner's SyndromeNastiti WidyariniNo ratings yet
- 58.stroke and Its Classification On The Basis ofDocument32 pages58.stroke and Its Classification On The Basis ofZeeshan AhmadNo ratings yet
- DD ParaparesisDocument9 pagesDD Paraparesishq_zhenNo ratings yet
- Brain TumorsDocument54 pagesBrain Tumorssrushtideokar0537No ratings yet
- Neuro FlashDocument54 pagesNeuro FlashrobertokutcherNo ratings yet
- Cavernous Sinus SyndromeDocument8 pagesCavernous Sinus SyndromeMuresan Ioana Catalina100% (1)
- Central Vertigo PDFDocument6 pagesCentral Vertigo PDFarlinieNo ratings yet
- Distinguishing Syncopal From Non-Syncopal Causes of Fall in Older PeopleDocument5 pagesDistinguishing Syncopal From Non-Syncopal Causes of Fall in Older PeopleCoco TamNo ratings yet
- Airways in Mediastinal Mass PDFDocument9 pagesAirways in Mediastinal Mass PDFHarish BhatNo ratings yet
- Cva 1Document42 pagesCva 1ياسر كوثر هانيNo ratings yet
- Anatomy and Physiology of Facial NerveDocument11 pagesAnatomy and Physiology of Facial NerveMohammed RahmathNo ratings yet
- BKO BOOK CHAPTER CH 33 Approach To A Patient With HemiparesisDocument8 pagesBKO BOOK CHAPTER CH 33 Approach To A Patient With HemiparesisBal Krishna OjhaNo ratings yet
- Definition of Stroke: 11/07/11 MUN FP Academic Half Day 1Document304 pagesDefinition of Stroke: 11/07/11 MUN FP Academic Half Day 1Deepthi TalasilaNo ratings yet
- Stroke:: Middle Cerebral Artery SyndromeDocument75 pagesStroke:: Middle Cerebral Artery SyndromeKapil LakhwaraNo ratings yet
- The Parts of SpeechDocument14 pagesThe Parts of SpeechiceNo ratings yet
- Welcome To English Grammar DomainDocument9 pagesWelcome To English Grammar DomainwulandarimerryNo ratings yet
- Ischemic Stroke Subtype Classification An Asian PDFDocument10 pagesIschemic Stroke Subtype Classification An Asian PDFNiluh ItaNo ratings yet
- Brainstem Stroke: Anatomy, Clinical and Radiological FindingsDocument11 pagesBrainstem Stroke: Anatomy, Clinical and Radiological FindingsMetta WitariNo ratings yet
- DOGMA PUSAT Biologi Molekuler: Replikasi DNA BaruDocument22 pagesDOGMA PUSAT Biologi Molekuler: Replikasi DNA BaruwulandarimerryNo ratings yet
- PNF Techniques in The Upper Extremity 2Document19 pagesPNF Techniques in The Upper Extremity 2sanalcrazyNo ratings yet
- Compartment Syndrome: - DiscussionDocument11 pagesCompartment Syndrome: - DiscussionatrisniaNo ratings yet
- Animal IIDocument15 pagesAnimal IIizabelaNo ratings yet
- ADocument8 pagesAMilagros Zevallos MelgarNo ratings yet
- Ptrs 06 113Document7 pagesPtrs 06 113ahmetrixNo ratings yet
- Surgical Handwashing Performance Checklist: Procedure 4 3 2 1Document1 pageSurgical Handwashing Performance Checklist: Procedure 4 3 2 1Charisse LuteroNo ratings yet
- Medgal Inventory OverallDocument1,313 pagesMedgal Inventory OverallTilz TilanzNo ratings yet
- Foundations of Structural Kinesiology: Lesson 1 PHED 349Document28 pagesFoundations of Structural Kinesiology: Lesson 1 PHED 349Rachel ChristensenNo ratings yet
- DR - Sundeep Jeten RajDocument32 pagesDR - Sundeep Jeten Rajselva3333No ratings yet
- Dwnload Full Foundations of Nursing 8th Edition Cooper Test Bank PDFDocument35 pagesDwnload Full Foundations of Nursing 8th Edition Cooper Test Bank PDFbologna.galleon7qhnrf100% (8)
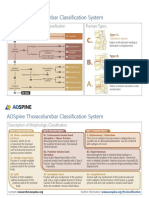
- AOSpine Thoracolumbar Classification System - Pocket CardDocument2 pagesAOSpine Thoracolumbar Classification System - Pocket CardFernanda Ahumada0% (1)
- Full Download Test Bank For Illustrated Anatomy of The Head and Neck 5th Edition by Fehrenbach PDF Full ChapterDocument36 pagesFull Download Test Bank For Illustrated Anatomy of The Head and Neck 5th Edition by Fehrenbach PDF Full Chapterstoredannage1uf100% (13)
- Current Concepts in Lower Extremity Reconstruction.36Document15 pagesCurrent Concepts in Lower Extremity Reconstruction.36Aura RivasNo ratings yet
- Hocevar 1981Document21 pagesHocevar 1981Aniket PotnisNo ratings yet
- Anaphy Lab ManualDocument9 pagesAnaphy Lab ManualKen KanekiNo ratings yet
- PJM NotesDocument26 pagesPJM NotesLeamy Reyes100% (1)
- Femoral Shaft FractureDocument5 pagesFemoral Shaft FracturePrimrose Gale ParingitNo ratings yet
- 10752-02 CH02 Final PDFDocument28 pages10752-02 CH02 Final PDFDejan MilenkovicNo ratings yet
- Ultrasound-Guided Lumbar Central Neuraxial Block 2016Document8 pagesUltrasound-Guided Lumbar Central Neuraxial Block 2016drkis20100% (1)
- Micron: ArticleinfoDocument12 pagesMicron: ArticleinfoSuhar TatiNo ratings yet
- Maya Chaudhary May 7Document11 pagesMaya Chaudhary May 7Dibyajyoti NathNo ratings yet