You might also like
- Operations and Supply Management Simulation Anita Souza Davenport University MGMT757Document22 pagesOperations and Supply Management Simulation Anita Souza Davenport University MGMT757Andrew Neuber90% (10)
- 10.1007/978 3 319 50343 1Document366 pages10.1007/978 3 319 50343 1Yi Sern ChuaNo ratings yet
- HEICS Complete ManualDocument273 pagesHEICS Complete ManualMisaiyaNo ratings yet
- MEPO For Petrel User Manual 101102Document21 pagesMEPO For Petrel User Manual 101102Kumar Landge0% (1)
- Capstone Math and Board Games Luc-Amrit ChaunyDocument51 pagesCapstone Math and Board Games Luc-Amrit Chaunyapi-284385959No ratings yet
- Work Immersion Experience at The Office of Barangay Hall of Poblacion Twelve Amadeo, CaviteDocument25 pagesWork Immersion Experience at The Office of Barangay Hall of Poblacion Twelve Amadeo, Cavitenoah villanueva73% (15)
- Introduction To Cost Estimation SoftwareDocument57 pagesIntroduction To Cost Estimation SoftwareGoutam Giri100% (4)
- 0 Comments: Disaster PreparednessDocument18 pages0 Comments: Disaster PreparednessCharis Paroginog100% (1)
- Simulation of Flows in Complex Geometries: New Meshing and SolutionDocument10 pagesSimulation of Flows in Complex Geometries: New Meshing and SolutionsangsharmaNo ratings yet
- TPM in The Connected FactoryDocument30 pagesTPM in The Connected Factoryss2mrattriNo ratings yet
- Chaos Theory and Disaster Response ManagementDocument22 pagesChaos Theory and Disaster Response Managementalina_terpuNo ratings yet
- What Disaster Response Management Can Learn From Chaos TheoryDocument14 pagesWhat Disaster Response Management Can Learn From Chaos TheorySteveNo ratings yet
- Berkes 2007Document13 pagesBerkes 2007Jose Francisco Sotelo LeyvaNo ratings yet
- MascalDocument28 pagesMascalPaul Andrew VioletaNo ratings yet
- A Stochastic Programming Approach For Shelter Location and Evacuation PlanningDocument27 pagesA Stochastic Programming Approach For Shelter Location and Evacuation PlanningSara SuarezNo ratings yet
- Scheffer Et Al 2012 Science Anticipating Critical TransitionsDocument6 pagesScheffer Et Al 2012 Science Anticipating Critical TransitionsMaggie FuentesNo ratings yet
- Design Principles For Critical Incident Response Systems: &) Æ R. Sharman Æ H. R. RaoDocument27 pagesDesign Principles For Critical Incident Response Systems: &) Æ R. Sharman Æ H. R. RaoSenait MebrahtuNo ratings yet
- 01 CCM 0000151063 85112 5aDocument9 pages01 CCM 0000151063 85112 5agarinda almadutaNo ratings yet
- What Disaster Response Management Can Learn From Chaos TheoryDocument23 pagesWhat Disaster Response Management Can Learn From Chaos TheoryHanna SyabrinaNo ratings yet
- Caso TeleconsultaDocument11 pagesCaso TeleconsultaNicolle CaroNo ratings yet
- ORMS Research in Disaster Operations ManagementDocument19 pagesORMS Research in Disaster Operations Managementmichael17ph2003No ratings yet
- A Review of Earthquake Statistics Fault and Seismicity-Based ModelsDocument22 pagesA Review of Earthquake Statistics Fault and Seismicity-Based ModelsHesty EmiliaNo ratings yet
- Chapter Thirteen: Organized For SuccessDocument22 pagesChapter Thirteen: Organized For SuccessCésar Rodríguez PeraltaNo ratings yet
- EMBLEM2: An Empirically Based Large Scale Evacuation Time Estimate ModelDocument15 pagesEMBLEM2: An Empirically Based Large Scale Evacuation Time Estimate ModelAMIR MUSINo ratings yet
- Environmental Catastrophes Under Time-Inconsistent Preferences (Tilburg University, 2013)Document40 pagesEnvironmental Catastrophes Under Time-Inconsistent Preferences (Tilburg University, 2013)Ferran Puig VilarNo ratings yet
- EtkinDocument32 pagesEtkinpreetiposwal123321No ratings yet
- What Makes Sammy-Samantha and Other Mammals Run? A First Round of ClosureDocument32 pagesWhat Makes Sammy-Samantha and Other Mammals Run? A First Round of Closureraramacha794222No ratings yet
- GPS For Early Warning System For DisastersDocument21 pagesGPS For Early Warning System For DisasterssirosiNo ratings yet
- Practical Applications of Cosmology To Human SocietyDocument35 pagesPractical Applications of Cosmology To Human Societyayush gargNo ratings yet
- Earthquake Literature ReviewDocument4 pagesEarthquake Literature Reviewafmzfxfaalkjcj100% (1)
- 5.1 A Typology of Evacuations: Timing of Evacuation Period of Evacuation Short Term Long TermDocument12 pages5.1 A Typology of Evacuations: Timing of Evacuation Period of Evacuation Short Term Long Termsrikanth5056No ratings yet
- Ecological Sustainability, Indicators and Climate Change: Robert CostanzaDocument34 pagesEcological Sustainability, Indicators and Climate Change: Robert CostanzaEnvsNo ratings yet
- Yohe and Dowlatabadi Risk and Uncertainties Analysis and EvaluationDocument46 pagesYohe and Dowlatabadi Risk and Uncertainties Analysis and EvaluationLordlennyxzie ArgentinaNo ratings yet
- Scheffer 2009 ADocument7 pagesScheffer 2009 AWilant GomariNo ratings yet
- Overview of Disasters in The Chemical Engineering Regime B Nikhil Rohan 2Document21 pagesOverview of Disasters in The Chemical Engineering Regime B Nikhil Rohan 2chandanjoy15No ratings yet
- Massive Casualty ManagementDocument48 pagesMassive Casualty Managementsuleiman adamuNo ratings yet
- 499 FullDocument13 pages499 FullMaimana AhmedNo ratings yet
- Emergency Health Services 1Document97 pagesEmergency Health Services 1aisa baladjiNo ratings yet
- HEMS Luxury or NecessityDocument3 pagesHEMS Luxury or NecessitykrisNo ratings yet
- Leadership FINAL NotesDocument9 pagesLeadership FINAL NotesMelinda RussellNo ratings yet
- Ems 6017 Nymc SPH Final Exam 2011Document9 pagesEms 6017 Nymc SPH Final Exam 2011splinky10No ratings yet
- Innis Lecture - Environmental Crises - PastDocument37 pagesInnis Lecture - Environmental Crises - PastMartha Huong LhcktNo ratings yet
- Effective Supply Chain Model For Disaster ManagementDocument22 pagesEffective Supply Chain Model For Disaster ManagementArka RockerNo ratings yet
- Disaster MedicineDocument38 pagesDisaster MedicineFazil KfNo ratings yet
- 2.11 Coping CapacityDocument6 pages2.11 Coping Capacityبلسم محمود شاكرNo ratings yet
- Crisis Plan On Mars Mathews MarkDocument9 pagesCrisis Plan On Mars Mathews Markapi-664106052No ratings yet
- The Social Psychology of Seismic Hazard Adjustment: Re-Evaluating The International LiteratureDocument15 pagesThe Social Psychology of Seismic Hazard Adjustment: Re-Evaluating The International LiteratureDixon Alexander Hernandez RiofrioNo ratings yet
- Bruneau Et Al 2003Document20 pagesBruneau Et Al 2003Taikhum VahanvatyNo ratings yet
- Nonlinear Dynamics, Chaos-Theory, and The "Sciences of Complexity": Their Relevance To The Study of The Interac-Tion Between Host and MicrofloraDocument17 pagesNonlinear Dynamics, Chaos-Theory, and The "Sciences of Complexity": Their Relevance To The Study of The Interac-Tion Between Host and MicroflorakrishnaNo ratings yet
- Chapter 6 - Hazard Vulnerability and Risk AnalysisDocument39 pagesChapter 6 - Hazard Vulnerability and Risk Analysisnotipu1100% (1)
- Or MS Research in Disaster Operations MaDocument20 pagesOr MS Research in Disaster Operations Manithish .aNo ratings yet
- ContrerasD - Shawd. 2016 DisasterManagementandResilienceinElectricPowersystems-ThecaseofChileDocument4 pagesContrerasD - Shawd. 2016 DisasterManagementandResilienceinElectricPowersystems-ThecaseofChileSorush SaeedyNo ratings yet
- Concept of Operations For A Regional TelemedicineDocument12 pagesConcept of Operations For A Regional TelemedicineDave SallaoNo ratings yet
- Decision Aid Models and Systems For Humanitarian Logistics. A SurveyDocument29 pagesDecision Aid Models and Systems For Humanitarian Logistics. A SurveyM3ph15t0No ratings yet
- Chapter 1: Basic Concept of Disaster and Disaster RiskDocument47 pagesChapter 1: Basic Concept of Disaster and Disaster RiskMiguel LigasNo ratings yet
- Special Issue KK Verma Part II 24 39 ArticlesDocument147 pagesSpecial Issue KK Verma Part II 24 39 ArticlesScribb DbircsNo ratings yet
- Decision Aid Models and Systems For Humanitarian Logistics. A SurveyDocument29 pagesDecision Aid Models and Systems For Humanitarian Logistics. A Surveymichael17ph2003No ratings yet
- Eichinger2021 Article ChallengesInThePREHOSPITALEmerDocument12 pagesEichinger2021 Article ChallengesInThePREHOSPITALEmerBarry TraceyNo ratings yet
- Resilience and Sustainable DevelopmentDocument11 pagesResilience and Sustainable DevelopmentMathiyazhagan KNo ratings yet
- Pages 411 418 51PEPA 03 A EmergencyDocument8 pagesPages 411 418 51PEPA 03 A Emergencyindri silvianiNo ratings yet
- WITH REF - Narrative Review Draft 1Document19 pagesWITH REF - Narrative Review Draft 1rajayasminNo ratings yet
- 2003 - Dennis M Woo - SociotechnicalsystemsriskmanagementandpublichealthDocument17 pages2003 - Dennis M Woo - SociotechnicalsystemsriskmanagementandpublichealthAbdulHakimZFNo ratings yet
- Revista Mexicana PDFDocument34 pagesRevista Mexicana PDFruddyferNo ratings yet
- R R: B U M: Esilience and Egions Uilding Nderstanding of The EtaphorDocument23 pagesR R: B U M: Esilience and Egions Uilding Nderstanding of The EtaphorIrin RiamandaNo ratings yet
- A Framework For Vulnerability Analysis in Sustainability ScienceDocument6 pagesA Framework For Vulnerability Analysis in Sustainability ScienceEvelise P. BarbozaNo ratings yet
- A Web-Based Decision Support System For Chronic Diseases: Chi-Chang ChangDocument11 pagesA Web-Based Decision Support System For Chronic Diseases: Chi-Chang ChangMucs Rabino LagadanNo ratings yet
- Brennan Center For Justice: Filibuster AbuseDocument36 pagesBrennan Center For Justice: Filibuster AbuseFixTheSenateNo ratings yet
- Kahneman Review Jel FinalDocument12 pagesKahneman Review Jel FinalpremohNo ratings yet
- Fractals and Path Dependent ProcessesDocument8 pagesFractals and Path Dependent ProcessesSteveNo ratings yet
- Nonfamily Abducted Children: National Estimates and CharacteristicsDocument16 pagesNonfamily Abducted Children: National Estimates and CharacteristicsThe Berlin Turnpike: A True Story of Human Trafficking in AmericaNo ratings yet
- Maps of Trends in Diabetes and ObesityDocument50 pagesMaps of Trends in Diabetes and ObesitySteveNo ratings yet
- Nonlinear Analysis of Disaster Response DataDocument7 pagesNonlinear Analysis of Disaster Response DataSteveNo ratings yet
- Self Organizing Processes in DisasterDocument1 pageSelf Organizing Processes in DisasterSteveNo ratings yet
- Disaster Responder's Perception of TimeDocument6 pagesDisaster Responder's Perception of TimeSteveNo ratings yet
- Summ 1016Document6 pagesSumm 1016SteveNo ratings yet
- JKJKDocument5 pagesJKJKFrancisca Cardenas OñateNo ratings yet
- Progression of Non-Cavitated Lesions in Dentin Through A Nonsurgical Approach - A Preliminary 12-Month Clinical ObservationDocument9 pagesProgression of Non-Cavitated Lesions in Dentin Through A Nonsurgical Approach - A Preliminary 12-Month Clinical ObservationSteveNo ratings yet
- Study Shows Gut Bacteria Byproduct Predicts Heart Attack and StrokeDocument2 pagesStudy Shows Gut Bacteria Byproduct Predicts Heart Attack and StrokeSteveNo ratings yet
- Digest - Disaster Responder's Perception of TimeDocument1 pageDigest - Disaster Responder's Perception of TimeSteveNo ratings yet
- Nonlinear Analysis of Disaster Response DataDocument7 pagesNonlinear Analysis of Disaster Response DataSteveNo ratings yet
- Citizens Without Proof Brennan CenterDocument3 pagesCitizens Without Proof Brennan Centerapi-349683833No ratings yet
- The Monastery of Carta Between The Ciste PDFDocument266 pagesThe Monastery of Carta Between The Ciste PDFSteve100% (1)
- Self Organizing Processes in DisasterDocument1 pageSelf Organizing Processes in DisasterSteveNo ratings yet
- Disaster Responder's Perception of TimeDocument6 pagesDisaster Responder's Perception of TimeSteveNo ratings yet
- NCCN Guidelines October 2018Document15 pagesNCCN Guidelines October 2018SteveNo ratings yet
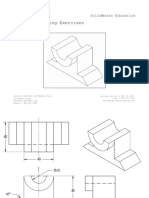
- Detailed Drawing Exercises: Solidworks EducationDocument51 pagesDetailed Drawing Exercises: Solidworks EducationLal Krrish MikeNo ratings yet
- AdsDocument16 pagesAdsSyed Masudur RahimNo ratings yet
- ReceivablesManagement - Whats New Viewer - SAP S4HANA 2021Document54 pagesReceivablesManagement - Whats New Viewer - SAP S4HANA 2021Даниела СтойковаNo ratings yet
- IEC Standards and Nonconventional Instrument TransformersDocument9 pagesIEC Standards and Nonconventional Instrument TransformersJonatan Costa BeberNo ratings yet
- Hardware-in-the-Loop Co-Simulation of Distribution Grid For Demand ResponseDocument9 pagesHardware-in-the-Loop Co-Simulation of Distribution Grid For Demand ResponsejorjijonNo ratings yet
- PV System Design NC IIIDocument68 pagesPV System Design NC IIIAngelo MichaelsNo ratings yet
- Input AnalysisDocument14 pagesInput AnalysisNovie Tyas Noegroho NingroemNo ratings yet
- Vibration Induced Low Backdisorders-Comparison of The Vibration Evaluation According To ISO 2631 With A Force-Related EvaluationDocument8 pagesVibration Induced Low Backdisorders-Comparison of The Vibration Evaluation According To ISO 2631 With A Force-Related EvaluationSedFarzamNo ratings yet
- MM MergedDocument541 pagesMM MergedAkash KumarNo ratings yet
- CFD-DEM Simulation To Predict The Critical Velocity of Slurry FlowsDocument8 pagesCFD-DEM Simulation To Predict The Critical Velocity of Slurry FlowsPrantik DasNo ratings yet
- Technical Note: Accelerate Design Cycles With Micron Simulation ModelsDocument6 pagesTechnical Note: Accelerate Design Cycles With Micron Simulation ModelsRamesh ChandrakasanNo ratings yet
- GT Simulator3: Operating ManualDocument178 pagesGT Simulator3: Operating Manualramontv032428No ratings yet
- HR Unit - IIIDocument77 pagesHR Unit - IIIPrabin ChaudharyNo ratings yet
- Acoustic and Respiratory Pressure Control in Brass PDFDocument232 pagesAcoustic and Respiratory Pressure Control in Brass PDFAndré QianNo ratings yet
- Calibration of Verley and Sotberg Soil Resistance Model For Pipelines Placed On Calcareous SoilsDocument9 pagesCalibration of Verley and Sotberg Soil Resistance Model For Pipelines Placed On Calcareous SoilsRyanPhillips50No ratings yet
- SV VCS UVM Design ChallengesDocument58 pagesSV VCS UVM Design ChallengesRed WhiteNo ratings yet
- Research On Ducted PropellersDocument47 pagesResearch On Ducted PropellersousmanNo ratings yet
- Application of Atp-Emtp in Determination of Optimal Settings For Differential Protection Ieds Under CT SaturationDocument6 pagesApplication of Atp-Emtp in Determination of Optimal Settings For Differential Protection Ieds Under CT SaturationgilbertomjcNo ratings yet
- Internship Report On Static Test Pad For Rocket Motor at Star - Space Technology and Aeronautical RocketryDocument17 pagesInternship Report On Static Test Pad For Rocket Motor at Star - Space Technology and Aeronautical RocketrySaheb BediNo ratings yet
- Active Front-End Rectifier Modelling Using Dynamic Phasors For More-Electric Aircraft Applications - IET - V5Document24 pagesActive Front-End Rectifier Modelling Using Dynamic Phasors For More-Electric Aircraft Applications - IET - V5Nuradin JemalNo ratings yet
- Traditional Teaching Methods vs. Teaching Through The Application of Information and Communication Technologies in The Accounting Field: Quo Vadis?Document30 pagesTraditional Teaching Methods vs. Teaching Through The Application of Information and Communication Technologies in The Accounting Field: Quo Vadis?Jhon Mark Miranda SantosNo ratings yet
- Article 19911Document13 pagesArticle 19911api-247795658No ratings yet
- Envisioning The Future of Transport and Mobility System For Debesmscat Using Futures ThinkingDocument26 pagesEnvisioning The Future of Transport and Mobility System For Debesmscat Using Futures ThinkingInternational Journal of Innovative Science and Research Technology100% (1)