You might also like
- Roadmap to Sustainable Textiles and Clothing: Environmental and Social Aspects of Textiles and Clothing Supply ChainFrom EverandRoadmap to Sustainable Textiles and Clothing: Environmental and Social Aspects of Textiles and Clothing Supply ChainNo ratings yet
- Evaluation of Cloth Masks and Modified Procedure Masks As Personal Protective Equipment For The PubliDocument18 pagesEvaluation of Cloth Masks and Modified Procedure Masks As Personal Protective Equipment For The Publiharaldd5No ratings yet
- 1 s2.0 S0048969721060307 MainDocument10 pages1 s2.0 S0048969721060307 MaincutdianNo ratings yet
- Measuring Breathability and Bacterial Filtration Efficiency ...Document14 pagesMeasuring Breathability and Bacterial Filtration Efficiency ...MarisolNo ratings yet
- Bacterial Profile of Multiple-Used Covid 19 Compliant N-95 Non-Surgical Face MaskDocument5 pagesBacterial Profile of Multiple-Used Covid 19 Compliant N-95 Non-Surgical Face MaskInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Reusable Mask For Coronavirus Disease 2019 (COVID-19) : OpinionDocument3 pagesA Reusable Mask For Coronavirus Disease 2019 (COVID-19) : OpinionBryan Panchana TorresNo ratings yet
- Association of American Physicians and SurgeonsDocument6 pagesAssociation of American Physicians and SurgeonsDavidNo ratings yet
- Virus Particles Are Transmissable From Presymptomatic Paucisymptomatic and Asymptomatic CarriersDocument5 pagesVirus Particles Are Transmissable From Presymptomatic Paucisymptomatic and Asymptomatic Carrierstim taulke johnsonNo ratings yet
- E!ectiveness of Cloth Masks For Protection Against Severe Acute Respiratory Syndrome Coronavirus 2Document9 pagesE!ectiveness of Cloth Masks For Protection Against Severe Acute Respiratory Syndrome Coronavirus 2nur hasbie ulfahNo ratings yet
- Covid-19 Face Masks A Potential Source of Microplastic Fibers in The EnvironmentDocument4 pagesCovid-19 Face Masks A Potential Source of Microplastic Fibers in The EnvironmentDevita AmeliaNo ratings yet
- Low-Cost Measurement of Facemask Efficacy For Filtering Expelled Droplets During SpeechDocument11 pagesLow-Cost Measurement of Facemask Efficacy For Filtering Expelled Droplets During SpeechJacob ObboNo ratings yet
- Sciadv Abd3083 Full PDFDocument11 pagesSciadv Abd3083 Full PDFjudith retanaNo ratings yet
- PIIS0140673620311831Document2 pagesPIIS0140673620311831kayegi8666No ratings yet
- Disposable Over Reusable Face Masks: Public Safety or Environmental Disaster?Document10 pagesDisposable Over Reusable Face Masks: Public Safety or Environmental Disaster?Yaya HizmiNo ratings yet
- Disposable Over Reusable Face Masks: Public Safety or Environmental Disaster?Document10 pagesDisposable Over Reusable Face Masks: Public Safety or Environmental Disaster?Damelys Evelyn Fernandez PeñaNo ratings yet
- Face MasksDocument11 pagesFace MaskspeterNo ratings yet
- Face Mask For Covid-19: A Social Responsibility: Sirisha Deepthi Sornapudi & Meenu SrivastavaDocument6 pagesFace Mask For Covid-19: A Social Responsibility: Sirisha Deepthi Sornapudi & Meenu SrivastavaTJPRC PublicationsNo ratings yet
- Liu 2020 IOP Conf. Ser. Earth Environ. Sci. 531 012034Document7 pagesLiu 2020 IOP Conf. Ser. Earth Environ. Sci. 531 012034letslearn procurementNo ratings yet
- Can Masks Be Reused After Hot Water Decontamination During The COVID 19 PandemicDocument7 pagesCan Masks Be Reused After Hot Water Decontamination During The COVID 19 PandemicNovela Sari, SKM, M.KesNo ratings yet
- Maximized Mask Fit CDCDocument4 pagesMaximized Mask Fit CDCputri.SpANo ratings yet
- Journal Article MaSK qUANTIDocument6 pagesJournal Article MaSK qUANTIEmerald James ZabalaNo ratings yet
- Heliyon: Abdul-Hakeem Alomari, Omer Aga, Lola El Sahmarany, Mariam Hegazi, Latifah AlmullaDocument8 pagesHeliyon: Abdul-Hakeem Alomari, Omer Aga, Lola El Sahmarany, Mariam Hegazi, Latifah AlmullaNovela Sari, SKM, M.KesNo ratings yet
- Are Cloth Masks A Substitute To Medical Masks in RDocument17 pagesAre Cloth Masks A Substitute To Medical Masks in RMaymayNo ratings yet
- Journal Pre-Proof: AJIC: American Journal of Infection ControlDocument18 pagesJournal Pre-Proof: AJIC: American Journal of Infection ControlKalpanaNo ratings yet
- Extended Abstract Fikar 2021Document10 pagesExtended Abstract Fikar 2021Dani Puji UtomoNo ratings yet
- Masks Don't Work - A Review of Science Relevant To COVID-19 Social Policy - River Cities' ReaderDocument17 pagesMasks Don't Work - A Review of Science Relevant To COVID-19 Social Policy - River Cities' ReadersalomaodomingosNo ratings yet
- What Are Good Ways To Address The Shortage of Face Masks by Anesthesiologists?Document9 pagesWhat Are Good Ways To Address The Shortage of Face Masks by Anesthesiologists?Sandra AraujoNo ratings yet
- Can Face Masks Offer Protection From Airborne Sneeze and Cough Droplets in Close-Up, Face-To-Face Human Interactions? - A Quantitative StudyDocument7 pagesCan Face Masks Offer Protection From Airborne Sneeze and Cough Droplets in Close-Up, Face-To-Face Human Interactions? - A Quantitative StudyStepan81No ratings yet
- Covid19 Research Links To Doctors, Scientists Includes Research Papers, Videos and EbooksDocument10 pagesCovid19 Research Links To Doctors, Scientists Includes Research Papers, Videos and EbooksrabidhunterNo ratings yet
- The Effectiveness of Face Masks To Prevent Sars Cov-2 Transmission: A Summary of The Peer-Review ScienceDocument5 pagesThe Effectiveness of Face Masks To Prevent Sars Cov-2 Transmission: A Summary of The Peer-Review ScienceKenNo ratings yet
- COVID-19 - What We Know So Far About Wearing Masks in PublicDocument14 pagesCOVID-19 - What We Know So Far About Wearing Masks in PublicElyk Dwi MumpuningtiasNo ratings yet
- Masks FinalDocument8 pagesMasks FinalTim100% (1)
- A Cluster Randomised Trial of Cloth Masks Compared With Medical Masks in Healthcare WorkersDocument13 pagesA Cluster Randomised Trial of Cloth Masks Compared With Medical Masks in Healthcare WorkersnafisahNo ratings yet
- International Journal of Nursing Studies AdvancesDocument29 pagesInternational Journal of Nursing Studies AdvancesNoNo ratings yet
- Fmed 07 594269Document14 pagesFmed 07 594269valmasci group 6No ratings yet
- TR - Mask Ppe EBM v1.2 3 25 2020Document9 pagesTR - Mask Ppe EBM v1.2 3 25 2020Yıldırım SütlüoğluNo ratings yet
- Research Capsule - UP StudentsDocument2 pagesResearch Capsule - UP StudentsKarra CasañaresNo ratings yet
- Dbouk, Talib & Drikakis, Dimitris - On Respiratory Droplets and Face Masks (2020) - Physics of Fluids 32, 063303 - 5.0015044Document12 pagesDbouk, Talib & Drikakis, Dimitris - On Respiratory Droplets and Face Masks (2020) - Physics of Fluids 32, 063303 - 5.0015044cbtext1sNo ratings yet
- Rubio Romero 2020 Disposable Masks Disinfection and SDocument11 pagesRubio Romero 2020 Disposable Masks Disinfection and SdaruNo ratings yet
- Science of The Total Environment: Broto Widya Hartanto, Dyah Samti MayasariDocument8 pagesScience of The Total Environment: Broto Widya Hartanto, Dyah Samti MayasariAden Dhana RizkitaNo ratings yet
- Sustainability 13 04948Document26 pagesSustainability 13 04948Olefile Mark MolokoNo ratings yet
- n95 Mask DataDocument8 pagesn95 Mask DatatrebajumiknjigeNo ratings yet
- Face Covering Revisi FinalDocument14 pagesFace Covering Revisi FinalLovelin TaniaNo ratings yet
- Applsci 12 09360 v2Document12 pagesApplsci 12 09360 v2davideNo ratings yet
- A Review On Recent Trends of Antiviral Nanoparticles and Airborne Flters - Special Insight On COVID 19 VirusDocument14 pagesA Review On Recent Trends of Antiviral Nanoparticles and Airborne Flters - Special Insight On COVID 19 Virusox1c14x16b2fx1d84x16a53xab9eNo ratings yet
- N95DECON UV Technicalreport v1.2 FinalDocument8 pagesN95DECON UV Technicalreport v1.2 FinalBrandonRojasNo ratings yet
- Bambuseaeco Mask: The Newly Enhanced Face Mask For Stem Students in The University of San Jose-RecoletosDocument22 pagesBambuseaeco Mask: The Newly Enhanced Face Mask For Stem Students in The University of San Jose-RecoletosEjay VillaverNo ratings yet
- Medical TextilesDocument128 pagesMedical Textilesirc.indusNo ratings yet
- Characteristics and Influencing Factors of Airborne Microplastics in Nail SalonsDocument9 pagesCharacteristics and Influencing Factors of Airborne Microplastics in Nail SalonsJhomara PalominoNo ratings yet
- An Alternative Application of Tissue Paper YmjdDocument1 pageAn Alternative Application of Tissue Paper Ymjdnadya aliviaNo ratings yet
- 1 s2.0 S0195670120303479 MainDocument7 pages1 s2.0 S0195670120303479 Mainalfredoongarogmail.comNo ratings yet
- Decontamination and Reuse of Surgical Masks and N95 Filtering Facepiece Respirators During The COVID-19 Pandemic: A Systematic ReviewDocument6 pagesDecontamination and Reuse of Surgical Masks and N95 Filtering Facepiece Respirators During The COVID-19 Pandemic: A Systematic ReviewKarinaayu SerinNo ratings yet
- Penggunaan APDDocument9 pagesPenggunaan APDNurulfitrahhafidNo ratings yet
- Maskd UpDocument10 pagesMaskd Upapi-590743757No ratings yet
- Ppe 16Document6 pagesPpe 16Sajin AlexanderNo ratings yet
- Effectiveness of Surgical KF94 and N95 Respirator Masks in Blocking SARS CoV 2 A Controlled Comparison in 7 PatientsDocument6 pagesEffectiveness of Surgical KF94 and N95 Respirator Masks in Blocking SARS CoV 2 A Controlled Comparison in 7 Patientsdr. EndahNo ratings yet
- Face Mask First RespondersDocument1 pageFace Mask First RespondersAlberto Caban-MartinezNo ratings yet
- Face Mask Detection Using Deep Learning An Approach 2021 Journal of BiomediDocument12 pagesFace Mask Detection Using Deep Learning An Approach 2021 Journal of BiomediOmkar VermaNo ratings yet
- Public Extent of Knowledge of The Nature From Which Face Masks Are Made During Covid-19 in The Libyan CommunityDocument9 pagesPublic Extent of Knowledge of The Nature From Which Face Masks Are Made During Covid-19 in The Libyan CommunityIJAR JOURNALNo ratings yet
- 1 s2.0 S019567012030178X MainDocument2 pages1 s2.0 S019567012030178X Mainanugraha GanendraNo ratings yet
- Half Masks (7700 & 5500) Series Data Sheet Eng-Rev-00Document2 pagesHalf Masks (7700 & 5500) Series Data Sheet Eng-Rev-00asesor2.ctgnaNo ratings yet
- Artigo 1 - Naked SurgeonDocument15 pagesArtigo 1 - Naked SurgeonLuan NunesNo ratings yet
- GP Catalog PDFDocument28 pagesGP Catalog PDFiMusic hshaNo ratings yet
- Surgical MasksDocument2 pagesSurgical MasksSparsh SharmaNo ratings yet
- Covid-19 Research ?Document414 pagesCovid-19 Research ?Zach Rigby100% (2)
- Sme ManufacturersDocument23 pagesSme ManufacturersWorking Capital100% (2)
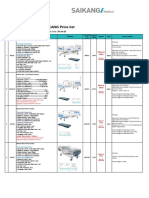
- SAIKANG Price List: Icu BedDocument7 pagesSAIKANG Price List: Icu BedAdrian Saul J RNo ratings yet
- Partial/Incomplete List of Qualified Examinees For The JULY 16 & 17, 2022 IN PRC CAR (Baguio City) Master Plumbers Licensure ExaminationDocument63 pagesPartial/Incomplete List of Qualified Examinees For The JULY 16 & 17, 2022 IN PRC CAR (Baguio City) Master Plumbers Licensure ExaminationPRC BaguioNo ratings yet
- Dead Bodies PDFDocument24 pagesDead Bodies PDFRj Concepcion RrtNo ratings yet
- Amended Complaint and Attachments Health Freedom Defense Fund Inc. Et Al v. Biden Et AlDocument58 pagesAmended Complaint and Attachments Health Freedom Defense Fund Inc. Et Al v. Biden Et AlDavid FoleyNo ratings yet
- Masks FinalDocument8 pagesMasks FinalTim100% (1)
- Tab 002 - Injury Illness Prevention PlanDocument23 pagesTab 002 - Injury Illness Prevention PlanGarret CraigNo ratings yet
- TLE 9-10 Nail Care M6 For PrintingDocument22 pagesTLE 9-10 Nail Care M6 For Printingveronica relenteNo ratings yet
- Mask - Material - Challenges - and - Virucidal - Properties - Nanoselulosa Dan GrapheneDocument14 pagesMask - Material - Challenges - and - Virucidal - Properties - Nanoselulosa Dan GrapheneAnnisa AvivahNo ratings yet
- PAFP Clinical Pathway For The Diagnosis and Management of Patients With COVID 19 in Family Practice PDFDocument35 pagesPAFP Clinical Pathway For The Diagnosis and Management of Patients With COVID 19 in Family Practice PDFZaqueo Gutierrez FajardoNo ratings yet
- Informed Consent Form (Annex A1) - KoronadalDocument3 pagesInformed Consent Form (Annex A1) - KoronadalJephte MantalabaNo ratings yet
- National Infection Control Guidelines - 2016 Draft For ConsultationDocument341 pagesNational Infection Control Guidelines - 2016 Draft For Consultationlimiya vargheseNo ratings yet
- Banana (Pseudo-Stem) As Eco-Friendly Alternative To Disposable Face MaskDocument10 pagesBanana (Pseudo-Stem) As Eco-Friendly Alternative To Disposable Face Maskkarleth angelNo ratings yet
- The Covid Lies UpdatedDocument31 pagesThe Covid Lies UpdatedSabinaNo ratings yet
- Tentative List of Qualified Examinees For The January 21 & 23, 2022 Architects Licensure Examination in Baguio CityDocument46 pagesTentative List of Qualified Examinees For The January 21 & 23, 2022 Architects Licensure Examination in Baguio CityPRC BaguioNo ratings yet
- Assessment of Knowledge, Attitudes, and Perception of Health Care Workers Regarding COVID-19Document10 pagesAssessment of Knowledge, Attitudes, and Perception of Health Care Workers Regarding COVID-19andris mejia alvarezNo ratings yet
- Prepare Necessary Equipment and Supplies. To Do The Appropriate Procedure. 2. Wash Your Hands. To Prevent The Spread of AnyDocument4 pagesPrepare Necessary Equipment and Supplies. To Do The Appropriate Procedure. 2. Wash Your Hands. To Prevent The Spread of AnyAlyssa Ashley A. ImamNo ratings yet
- Blaylock Face Masks Pose Serious Risks To The HealthyDocument8 pagesBlaylock Face Masks Pose Serious Risks To The HealthyDonnaveo ShermanNo ratings yet
- Donning Doffing of PPE ChecklistDocument5 pagesDonning Doffing of PPE ChecklistNoorwashilaNo ratings yet
- COVID-19: Master Circular On LockdownDocument32 pagesCOVID-19: Master Circular On LockdownShantanu BhardwajNo ratings yet
- February 2023 PROGRAM OF THE MPLEDocument8 pagesFebruary 2023 PROGRAM OF THE MPLEDale Iverson LacastreNo ratings yet
- Eng & Soc Finalised-RevisedDocument24 pagesEng & Soc Finalised-RevisedPriya Daccu KanasonNo ratings yet
- Tentative List of Qualified Examinees For The February 8 & 9, 2022 Psychometricians Licensure Examination in Baguio CityDocument48 pagesTentative List of Qualified Examinees For The February 8 & 9, 2022 Psychometricians Licensure Examination in Baguio CityPRC Baguio75% (4)
- Cultivating Quality Implementing Surgical Smoke.31Document5 pagesCultivating Quality Implementing Surgical Smoke.31Dedi Landani GintingNo ratings yet
- Leadership Letter 1.21.2022Document11 pagesLeadership Letter 1.21.2022Helen Bennett100% (1)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipFrom EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipRating: 4.5 out of 5 stars4.5/5 (1135)
- Breaking the Habit of Being YourselfFrom EverandBreaking the Habit of Being YourselfRating: 4.5 out of 5 stars4.5/5 (1461)
- Roxane Gay & Everand Originals Presents: Good Girl: Notes on Dog RescueFrom EverandRoxane Gay & Everand Originals Presents: Good Girl: Notes on Dog RescueRating: 4.5 out of 5 stars4.5/5 (31)
- Roxane Gay & Everand Originals Presents: Good Girl: Notes on Dog RescueFrom EverandRoxane Gay & Everand Originals Presents: Good Girl: Notes on Dog RescueRating: 5 out of 5 stars5/5 (4)
- Peaceful Sleep Hypnosis: Meditate & RelaxFrom EverandPeaceful Sleep Hypnosis: Meditate & RelaxRating: 4.5 out of 5 stars4.5/5 (144)
- Allen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductFrom EverandAllen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductRating: 5 out of 5 stars5/5 (31)
- Love Yourself, Heal Your Life Workbook (Insight Guide)From EverandLove Yourself, Heal Your Life Workbook (Insight Guide)Rating: 5 out of 5 stars5/5 (40)
- Find Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeFrom EverandFind Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeRating: 4 out of 5 stars4/5 (3)
- Deep Sleep Hypnosis: Guided Meditation For Sleep & HealingFrom EverandDeep Sleep Hypnosis: Guided Meditation For Sleep & HealingRating: 4.5 out of 5 stars4.5/5 (104)
- The Noom Kitchen: 100 Healthy, Delicious, Flexible Recipes for Every DayFrom EverandThe Noom Kitchen: 100 Healthy, Delicious, Flexible Recipes for Every DayNo ratings yet
- Summary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissFrom EverandSummary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissRating: 4.5 out of 5 stars4.5/5 (82)
- Alex & Me: How a Scientist and a Parrot Discovered a Hidden World of Animal Intelligence—and Formed a Deep Bond in the ProcessFrom EverandAlex & Me: How a Scientist and a Parrot Discovered a Hidden World of Animal Intelligence—and Formed a Deep Bond in the ProcessNo ratings yet
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Forever Strong: A New, Science-Based Strategy for Aging WellFrom EverandForever Strong: A New, Science-Based Strategy for Aging WellNo ratings yet
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerFrom EverandThe Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerRating: 4.5 out of 5 stars4.5/5 (58)
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeFrom EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeRating: 3.5 out of 5 stars3.5/5 (13)
- Aging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayFrom EverandAging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayNo ratings yet
- The Self-Care Solution: A Year of Becoming Happier, Healthier, and Fitter—One Month at a TimeFrom EverandThe Self-Care Solution: A Year of Becoming Happier, Healthier, and Fitter—One Month at a TimeRating: 3 out of 5 stars3/5 (5)
- Glucose Revolution: The Life-Changing Power of Balancing Your Blood SugarFrom EverandGlucose Revolution: The Life-Changing Power of Balancing Your Blood SugarRating: 5 out of 5 stars5/5 (352)
- What to Expect When You’re Expecting (5th Edition)From EverandWhat to Expect When You’re Expecting (5th Edition)Rating: 5 out of 5 stars5/5 (1)
- Chair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouFrom EverandChair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouRating: 3.5 out of 5 stars3.5/5 (5)
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomFrom EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomRating: 4 out of 5 stars4/5 (1)