You might also like
- Vineland 3Document2 pagesVineland 3Teguh Lesmana71% (7)
- Questionnaire 3 Adult DIVA 5Document19 pagesQuestionnaire 3 Adult DIVA 5Maria Nistor100% (3)
- Parent Child Relationship InventoryDocument3 pagesParent Child Relationship InventoryAggelou Maya100% (1)
- Interview Questions 5Document5 pagesInterview Questions 5api-502274542No ratings yet
- Nur 420 - Policy Action Plan PaperDocument9 pagesNur 420 - Policy Action Plan Paperapi-375928224No ratings yet
- A Developmental Psychopathology Perspective On Child MaltreatmentDocument19 pagesA Developmental Psychopathology Perspective On Child Maltreatmentinessilvapereira249No ratings yet
- Child Development - 2011 - Lowell - A Randomized Controlled Trial of Child FIRST A Comprehensive Home Based InterventionDocument16 pagesChild Development - 2011 - Lowell - A Randomized Controlled Trial of Child FIRST A Comprehensive Home Based InterventionCláudia Isabel SilvaNo ratings yet
- 21323-Article Text-32143-2-10-20190221Document15 pages21323-Article Text-32143-2-10-20190221Meg JonesNo ratings yet
- TBRIArticle 1Document28 pagesTBRIArticle 1Ángela Maria TangarifeNo ratings yet
- Supporting Families Exposed To Adverse Childhood Experiences Within Child Care Settings: A Feasibility PilotDocument12 pagesSupporting Families Exposed To Adverse Childhood Experiences Within Child Care Settings: A Feasibility PilotKaren CárcamoNo ratings yet
- Pediatric Recent AdvancementDocument2 pagesPediatric Recent AdvancementAnonymous ceYk4p4No ratings yet
- Journal-Children Mental Health need-MOTIVATION Nihms143149Document24 pagesJournal-Children Mental Health need-MOTIVATION Nihms143149Fasihah LiewNo ratings yet
- CC - Health Care Assess To Children in Psychiatric FacilitiesDocument10 pagesCC - Health Care Assess To Children in Psychiatric Facilitiesapi-570349057No ratings yet
- Children and Youth Services ReviewDocument11 pagesChildren and Youth Services ReviewNadia Cenat CenutNo ratings yet
- SPHERU DevelopmentalHealth enDocument8 pagesSPHERU DevelopmentalHealth enkidSKAN DirectorNo ratings yet
- NIH Public Access: Author ManuscriptDocument24 pagesNIH Public Access: Author ManuscriptRicardo Vio LeonardiNo ratings yet
- Masia Warner2005 Article School BasedInterventionForAdoDocument16 pagesMasia Warner2005 Article School BasedInterventionForAdoKyle RossNo ratings yet
- Children and Youth Services Review: Jessica Dym Bartlett, Berenice RushovichDocument9 pagesChildren and Youth Services Review: Jessica Dym Bartlett, Berenice RushovichEduardo Arruda SautchukNo ratings yet
- Patrick Esposito MaltreatmentDocument5 pagesPatrick Esposito Maltreatmentapi-313736865No ratings yet
- Child Abuse Research Paper - Draft 20191020 PDFDocument5 pagesChild Abuse Research Paper - Draft 20191020 PDFJerry EspinosaNo ratings yet
- 1 s2.0 S0190740915000870 Main PDFDocument7 pages1 s2.0 S0190740915000870 Main PDFYusranNo ratings yet
- Child Welfare Watch: Baby StepsDocument28 pagesChild Welfare Watch: Baby StepsCenterNYCNo ratings yet
- The Prevention of Child Physical Abuse and NeglectDocument51 pagesThe Prevention of Child Physical Abuse and Neglectbach.nnhienNo ratings yet
- Lahti 2018Document12 pagesLahti 2018Yamil Ortega RiverosNo ratings yet
- The Bucharest Early Intervention Project - Adolescent Mental Health and Adaptation Following Early DeprivationDocument8 pagesThe Bucharest Early Intervention Project - Adolescent Mental Health and Adaptation Following Early DeprivationMerly JHNo ratings yet
- Prof Ed - Child and AdolescentDocument4 pagesProf Ed - Child and AdolescentLindesol SolivaNo ratings yet
- Vanderzee - Treatments For Early Childhood Trauma DecisionDocument14 pagesVanderzee - Treatments For Early Childhood Trauma DecisionClaudia Irma Portilla CamposNo ratings yet
- Ravy y Casoralo (2018) Childrens Exposure To IPV A Qualitative ReviewDocument14 pagesRavy y Casoralo (2018) Childrens Exposure To IPV A Qualitative ReviewCarlos ClavijoNo ratings yet
- Challenges in Building Child and Family Resilience After Disasters PDFDocument15 pagesChallenges in Building Child and Family Resilience After Disasters PDFEunice LimNo ratings yet
- LR EffectivenessDocument24 pagesLR Effectivenessapi-349022556No ratings yet
- Article 5Document9 pagesArticle 5Vanity TrimbleNo ratings yet
- Program Components of Psychosocial Interventions in Foster and Kinship Care: A Systematic ReviewDocument28 pagesProgram Components of Psychosocial Interventions in Foster and Kinship Care: A Systematic ReviewFLAVIAOLIVARESNo ratings yet
- Child Maltreatment Prevention Programs Research PaperDocument14 pagesChild Maltreatment Prevention Programs Research Paperapi-349307498No ratings yet
- Chapter 1 SheillaDocument46 pagesChapter 1 SheillaElla SheiNo ratings yet
- Chapter17 - Child and Adolescent Psychiatry InterventionsDocument26 pagesChapter17 - Child and Adolescent Psychiatry InterventionsteddyskinnerNo ratings yet
- ResiliencyDocument17 pagesResiliencyapi-662868701No ratings yet
- Child Development 1Document9 pagesChild Development 1KASANGA NEVILLE KITONYI BE100SEPT19No ratings yet
- Pgda WP 69Document19 pagesPgda WP 69tasya tazkia regita zahraNo ratings yet
- RESUMEN EJECUTIVO-Divulgación de La Práctica Basada en La Evidencia en Niños y adolescentes-APADocument11 pagesRESUMEN EJECUTIVO-Divulgación de La Práctica Basada en La Evidencia en Niños y adolescentes-APAjorgemelladoneurodesarrolloNo ratings yet
- Child Maltreatment Chapter RGDocument33 pagesChild Maltreatment Chapter RGapi-340372890No ratings yet
- Long Term Consequences of Child Abuse and NeglectDocument10 pagesLong Term Consequences of Child Abuse and NeglectEdward Rey Ubanan100% (1)
- Healthy Steps As A ModeratorDocument16 pagesHealthy Steps As A ModeratorFelipe José Aguilar de la MataNo ratings yet
- Resilience When Faced With Childhood Adversity FinalDocument17 pagesResilience When Faced With Childhood Adversity Finalapi-662868701No ratings yet
- 20.3 Noyes GrosserDocument20 pages20.3 Noyes GrosserRashidah Abd WahidNo ratings yet
- Transforming Practice With HOPE (Healthy Outcomes From Positive Experiences)Document6 pagesTransforming Practice With HOPE (Healthy Outcomes From Positive Experiences)Catarina GrandeNo ratings yet
- Childabuseandneglect: The Role of The Primary Care PediatricianDocument15 pagesChildabuseandneglect: The Role of The Primary Care PediatricianMilagros Saavedra RecharteNo ratings yet
- Ej 1218579afadfDocument19 pagesEj 1218579afadfMegumiAlbaNo ratings yet
- Childhood Trauma Exposure and Toxic StressDocument8 pagesChildhood Trauma Exposure and Toxic StressSan NuNo ratings yet
- Estimating The Prevalence ofDocument8 pagesEstimating The Prevalence ofKarel GuevaraNo ratings yet
- Lancet 2011 - Papers 1 and 2 PDFDocument31 pagesLancet 2011 - Papers 1 and 2 PDFpyeohhpyeNo ratings yet
- Attachment Styles in Alternative Care SLRDocument29 pagesAttachment Styles in Alternative Care SLRAlicia FuentesNo ratings yet
- Jcd-Playtherapy and AcesDocument12 pagesJcd-Playtherapy and AcesAndreia SilvaNo ratings yet
- TF CBTDocument12 pagesTF CBTBrittany Wright PruittNo ratings yet
- Long-Term Poverty and Child Development in The United States: Results From The NLSYDocument45 pagesLong-Term Poverty and Child Development in The United States: Results From The NLSYRabya AmjadNo ratings yet
- EP1 Example 5Document4 pagesEP1 Example 5jjj777jjjNo ratings yet
- Kafas 2009Document7 pagesKafas 2009Anonymous xgY5a6JBbNo ratings yet
- Child Welfare Group Care Literature ReviewDocument4 pagesChild Welfare Group Care Literature Reviewrpmvtcrif100% (1)
- Fowler2017 - Term Paper Shit PDFDocument6 pagesFowler2017 - Term Paper Shit PDFAnsalNo ratings yet
- Bartlett, 2018 - TFCBTDocument8 pagesBartlett, 2018 - TFCBTOlga MichailidouNo ratings yet
- Gastilo, Christy L - Summative Assessment TasksDocument22 pagesGastilo, Christy L - Summative Assessment TasksChristy Lordan GastiloNo ratings yet
- Evidence Set 4 - Understanding Complex Trauma and Out of Home CareDocument15 pagesEvidence Set 4 - Understanding Complex Trauma and Out of Home Careapi-479322627No ratings yet
- Incredible Years ProgramDocument11 pagesIncredible Years ProgramKallia KoufakiNo ratings yet
- Child Sexual Abuse: Current Evidence, Clinical Practice, and Policy DirectionsFrom EverandChild Sexual Abuse: Current Evidence, Clinical Practice, and Policy DirectionsNo ratings yet
- Holseniversensmith PDFDocument11 pagesHolseniversensmith PDFConyNo ratings yet
- Holseniversensmith PDFDocument11 pagesHolseniversensmith PDFConyNo ratings yet
- ContentServer PDFDocument14 pagesContentServer PDFConyNo ratings yet
- ContentServer PDFDocument5 pagesContentServer PDFConyNo ratings yet
- Educators Frequently Hear About Successful SEL Programs and Are Then Faced With Answering The Following QuestionsDocument3 pagesEducators Frequently Hear About Successful SEL Programs and Are Then Faced With Answering The Following QuestionsConyNo ratings yet
- ContentServer PDFDocument9 pagesContentServer PDFConyNo ratings yet
- Arënliu2020 Article EmpoweringThePeerGroupToPreven PDFDocument14 pagesArënliu2020 Article EmpoweringThePeerGroupToPreven PDFConyNo ratings yet
- Stephenie Rascol ResumeDocument2 pagesStephenie Rascol Resumeapi-335892001No ratings yet
- Early Language and Literacy FlyerDocument2 pagesEarly Language and Literacy Flyerapi-501003650No ratings yet
- Perdev ReportDocument30 pagesPerdev ReportJacey Bautista MargalloNo ratings yet
- Formulas For Ages: Important Concepts On Problems On AgesDocument31 pagesFormulas For Ages: Important Concepts On Problems On Agesdhivya mNo ratings yet
- ADVANCED Maternal AgeDocument6 pagesADVANCED Maternal AgeAbiodun AdeniranNo ratings yet
- Day 1 Session 5. Understanding Adolescence Puberty Fertility Awareness PPTX OrigDocument18 pagesDay 1 Session 5. Understanding Adolescence Puberty Fertility Awareness PPTX OrigRyoHaradaNo ratings yet
- 107 Quiz Preschoool Ado Schol AgeDocument3 pages107 Quiz Preschoool Ado Schol AgeMarifel Sombreno PeñarandaNo ratings yet
- Trauma For Parent Groups 10 - 10 - 19Document44 pagesTrauma For Parent Groups 10 - 10 - 19Htet HtinNo ratings yet
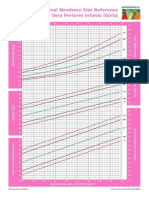
- Intergrowth21 Newborn Size Reference Charts (Girls)Document2 pagesIntergrowth21 Newborn Size Reference Charts (Girls)Anonymous MWd5UOUuiyNo ratings yet
- Emotional Dependence in Teenagers Essay1Document8 pagesEmotional Dependence in Teenagers Essay1Ricardo Alarcon PinoNo ratings yet
- 5-Child Guidance ClinicsDocument13 pages5-Child Guidance ClinicsSwati LalNo ratings yet
- Personality Test Center - IPIP NEO - The Five Factor Model of PersonalityDocument14 pagesPersonality Test Center - IPIP NEO - The Five Factor Model of PersonalityKATERYNA IVANYSHYNNo ratings yet
- J Paid 2005 02 004Document11 pagesJ Paid 2005 02 004habeeb UppinangadyNo ratings yet
- Baby Dumping in MalaysiaDocument49 pagesBaby Dumping in MalaysiaKamini KamalanNo ratings yet
- Advocacy LetterDocument5 pagesAdvocacy Letterapi-250895737No ratings yet
- Maya Maratun SholikhahDocument8 pagesMaya Maratun Sholikhahffarras.taqiNo ratings yet
- Pinaka Final Nani PistiDocument6 pagesPinaka Final Nani PistiBryan FielNo ratings yet
- Controversies Practice Changers in Ob-GynDocument57 pagesControversies Practice Changers in Ob-GynVirginia AbalosNo ratings yet
- Myself and My Family: Reproductive Health LawDocument6 pagesMyself and My Family: Reproductive Health LawSheena AmitNo ratings yet
- Resumeforportfolio 2Document2 pagesResumeforportfolio 2api-317153322No ratings yet
- NCP Problem 1Document3 pagesNCP Problem 1Simbo Ralph JulesNo ratings yet
- VED04 COURSE OUTLINE PSYCHOLOGICAL THEORIES OF VALUES EDUCATIONDocument4 pagesVED04 COURSE OUTLINE PSYCHOLOGICAL THEORIES OF VALUES EDUCATIONANJANETT BUENAVENTURANo ratings yet
- Childcare Reference FormDocument2 pagesChildcare Reference Formjimena sanchezNo ratings yet
- Reducing Teen PregnancyDocument10 pagesReducing Teen PregnancyANo ratings yet
- Esai Tentang Kebidanan Dalam Bahasa InggrisDocument3 pagesEsai Tentang Kebidanan Dalam Bahasa InggrisElysa WahyuNo ratings yet
- Talkiing With Children Conceived Through Donor Insemination, IVF With Egg Donor or SurrogacyDocument3 pagesTalkiing With Children Conceived Through Donor Insemination, IVF With Egg Donor or SurrogacyVeronica FerreyraNo ratings yet