You might also like
- Pediatric Pain and Symptom Management Guidelines: Dana Farber Cancer Institute/Boston Children's HospitalDocument27 pagesPediatric Pain and Symptom Management Guidelines: Dana Farber Cancer Institute/Boston Children's HospitalDaeng Anggit AdirahmanNo ratings yet
- Buprenorphine/Suboxone Micro-Initionation Induction While Using Fentanyl (Burnese Method)Document23 pagesBuprenorphine/Suboxone Micro-Initionation Induction While Using Fentanyl (Burnese Method)Hunter J. WadeNo ratings yet
- Pain Provider AcutePainProviderEducationalGuide IB10998Document28 pagesPain Provider AcutePainProviderEducationalGuide IB10998melawatiNo ratings yet
- Adult Pocket Opioid PrescribingDocument19 pagesAdult Pocket Opioid PrescribingAmisha VastaniNo ratings yet
- Principles of Opioid Management: Symptom GuidelinesDocument45 pagesPrinciples of Opioid Management: Symptom GuidelinesTheresia Avila KurniaNo ratings yet
- Adapted From CDC Guideline: Assess Pain & FunctionDocument2 pagesAdapted From CDC Guideline: Assess Pain & FunctionSolomon Seth SallforsNo ratings yet
- Pharmacy Bulletin HSS 2-2018Document9 pagesPharmacy Bulletin HSS 2-2018Ridzuan AsmiraNo ratings yet
- PocketGuide FINAL6 PDFDocument2 pagesPocketGuide FINAL6 PDFSolomon Seth SallforsNo ratings yet
- Managing Opioid Withdrawal With BuprenorphineDocument7 pagesManaging Opioid Withdrawal With BuprenorphineAgata KurniawatyNo ratings yet
- Treatment of Common Mental DisordersDocument77 pagesTreatment of Common Mental DisordersnelsonNo ratings yet
- Edited: DR - Dairion Gatot M.Ked SP - PD-KHOMDocument57 pagesEdited: DR - Dairion Gatot M.Ked SP - PD-KHOMayuhati siregarNo ratings yet
- Symptom Control and Caring For The Dying Patient 4th EditionDocument26 pagesSymptom Control and Caring For The Dying Patient 4th EditionLaurencia LenyNo ratings yet
- Opioid Topic DiscussionDocument22 pagesOpioid Topic Discussionapi-587439953No ratings yet
- Polypharmacy and Drug-Drug InteractionsDocument28 pagesPolypharmacy and Drug-Drug Interactionsapi-583778137No ratings yet
- Pain - Opioids Combined PDFDocument26 pagesPain - Opioids Combined PDFJenna DantNo ratings yet
- Opioid Toxicity: Nathaniel Katz, MD Harvard Medical School Boston, MADocument26 pagesOpioid Toxicity: Nathaniel Katz, MD Harvard Medical School Boston, MARoman Al MamunNo ratings yet
- 1PainAssessment - Pharmokinetics - 2018 Jeannies EditDocument54 pages1PainAssessment - Pharmokinetics - 2018 Jeannies EditApostolos T.No ratings yet
- Drug Re L Ated Pro B LemsDocument33 pagesDrug Re L Ated Pro B LemsChie ZhumieNo ratings yet
- Review WHOPainLadder OpioidsandNonOpioidsDocument13 pagesReview WHOPainLadder OpioidsandNonOpioidsamajida fadia rNo ratings yet
- Clinical Pharmacy: By: Narendar KumarDocument14 pagesClinical Pharmacy: By: Narendar KumarAlee Iz HarNo ratings yet
- Pain Patho Physiology Opioid UseDocument52 pagesPain Patho Physiology Opioid UseshokoNo ratings yet
- Clinical Practice Guidelines For OSTDocument77 pagesClinical Practice Guidelines For OSTHaris AhmedNo ratings yet
- Opiates 2008Document102 pagesOpiates 2008drdavemcdowellNo ratings yet
- WS 4 - Risani Andalasia Putri, M.Farm., Apt - PAIN MANAGEMENTDocument66 pagesWS 4 - Risani Andalasia Putri, M.Farm., Apt - PAIN MANAGEMENTMuhammad HabibieNo ratings yet
- ChoosePT - Electrotherapy, Effective Alternative For Opioid Reduction? (PDFDrive)Document118 pagesChoosePT - Electrotherapy, Effective Alternative For Opioid Reduction? (PDFDrive)kk2483697No ratings yet
- III. Antipsychotic DrugsDocument31 pagesIII. Antipsychotic DrugsDanica AbarquezNo ratings yet
- Integrated Therapeutics IiiDocument67 pagesIntegrated Therapeutics IiiSalahadinNo ratings yet
- AntipsychoticsDocument51 pagesAntipsychoticsShailja SharmaNo ratings yet
- Final Product 2Document4 pagesFinal Product 2api-601265441No ratings yet
- Protocol 010Document12 pagesProtocol 010hatem newishyNo ratings yet
- Opioid PharmacologyDocument47 pagesOpioid PharmacologyEva K. Al KaryNo ratings yet
- Art of PolypharmacyDocument21 pagesArt of Polypharmacytanu sharmaNo ratings yet
- 8-Page Version - HHS Guidance For Dosage Reduction or Discontinuation of OpioidsDocument8 pages8-Page Version - HHS Guidance For Dosage Reduction or Discontinuation of OpioidsAnonymous YsPsAHLNo ratings yet
- Basics of Opioid Prescribing - Part II: Pain Management and OpioidsDocument8 pagesBasics of Opioid Prescribing - Part II: Pain Management and Opioidsga_boxNo ratings yet
- 01.EMMS - General Pharmacology 1Document32 pages01.EMMS - General Pharmacology 1Faisal FahadNo ratings yet
- ADPTBDocument41 pagesADPTBHarlinda myraNo ratings yet
- 2reconsidering Opioid Therapy Mar 2013Document6 pages2reconsidering Opioid Therapy Mar 2013Anonymous 4txA8N8etNo ratings yet
- GHFHGFGFHFGHFHGDocument12 pagesGHFHGFGFHFGHFHGsarascrNo ratings yet
- Schizophrenia: Nur SyazwaniDocument30 pagesSchizophrenia: Nur SyazwanibyteNo ratings yet
- Acep Equal Opiod Wave IiDocument43 pagesAcep Equal Opiod Wave IiJesse M. MassieNo ratings yet
- NCM 106 NarcoticsDocument25 pagesNCM 106 NarcoticsMelchizedek Tagarino TorioNo ratings yet
- NCM 106 NarcoticsDocument25 pagesNCM 106 NarcoticsMelchizedek Tagarino TorioNo ratings yet
- Cancer Pain Management: Opioid Analgesics, Part 2Document20 pagesCancer Pain Management: Opioid Analgesics, Part 2azkiel fikrieNo ratings yet
- Checklist For Prescribing Opioids For Chronic Pain: When CONSIDERING Long-Term Opioid TherapyDocument1 pageChecklist For Prescribing Opioids For Chronic Pain: When CONSIDERING Long-Term Opioid TherapyMarcelo UGNo ratings yet
- B. DepressionDocument7 pagesB. Depressionチャン フィラNo ratings yet
- Pharma Day1Document184 pagesPharma Day1Nhelia Santos BañagaNo ratings yet
- Unit 1Document15 pagesUnit 1kunalNo ratings yet
- Drug Study:: Bipolar I DisorderDocument4 pagesDrug Study:: Bipolar I DisorderSolsona Natl HS MaanantengNo ratings yet
- Template For Meds: Respiratory DepressionDocument2 pagesTemplate For Meds: Respiratory DepressionSusan Powell-ProctorNo ratings yet
- Key Points: Balanced Anesthesia in Small Animal Patients: Incorporating Cri'SDocument2 pagesKey Points: Balanced Anesthesia in Small Animal Patients: Incorporating Cri'SAlejandro Estrada RiosNo ratings yet
- Opioids: Addiction and TreatmentsDocument20 pagesOpioids: Addiction and TreatmentsrinaviadrinririnNo ratings yet
- General and Local AnesthesiaDocument139 pagesGeneral and Local AnesthesiaJonathan KipropNo ratings yet
- Smoking Cessation AGU UpdatedDocument33 pagesSmoking Cessation AGU UpdatedRahaf AlhubailNo ratings yet
- Drug Abuse and MisuseDocument29 pagesDrug Abuse and MisuseDilawar AheerNo ratings yet
- Mount Carmel Medication Management Pocket GuideDocument2 pagesMount Carmel Medication Management Pocket GuideWOSU100% (1)
- Pain Management Clinical Guidelinesv2 PDFDocument15 pagesPain Management Clinical Guidelinesv2 PDFErwin Novia Rachmawati100% (1)
- PrednisoneDocument3 pagesPrednisoneShaira TanNo ratings yet
- Opioid Toxicity: Nathaniel Katz, MD Harvard Medical School Boston, MADocument26 pagesOpioid Toxicity: Nathaniel Katz, MD Harvard Medical School Boston, MAYohanes FirmansyahNo ratings yet
- Ppolypharmacy 2020 ENsDocument26 pagesPpolypharmacy 2020 ENsRegina PunNo ratings yet
- Patient Roadmap - Adult Dec 2019Document4 pagesPatient Roadmap - Adult Dec 2019M Naeem Arham100% (1)
- Common Office Billing CodesDocument3 pagesCommon Office Billing CodesM Naeem ArhamNo ratings yet
- Approved Prescription Products For Menopausal Symptoms in The United States and CanadaDocument7 pagesApproved Prescription Products For Menopausal Symptoms in The United States and CanadaM Naeem ArhamNo ratings yet
- Preparing For A Virtual Appointment BCCFP InfographicDocument1 pagePreparing For A Virtual Appointment BCCFP InfographicM Naeem ArhamNo ratings yet
- AF Gui 2018 PG EN WebDocument36 pagesAF Gui 2018 PG EN WebM Naeem ArhamNo ratings yet
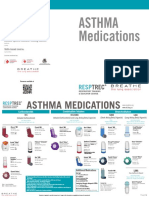
- Courses Offered:: Asthma MedicationsDocument2 pagesCourses Offered:: Asthma MedicationsM Naeem ArhamNo ratings yet
- Overview of Tool and Key Points: Section A: HistoryDocument4 pagesOverview of Tool and Key Points: Section A: HistoryM Naeem ArhamNo ratings yet
- What's New?: Canadian Recommendations For The Management of HypertensionDocument9 pagesWhat's New?: Canadian Recommendations For The Management of HypertensionM Naeem ArhamNo ratings yet
- Risk DM 2Document6 pagesRisk DM 2PraveenNo ratings yet
- Alberti 2004Document14 pagesAlberti 2004Messias FilhoNo ratings yet
- Ulcerative Colitis Homeopathic Treatment PDFDocument3 pagesUlcerative Colitis Homeopathic Treatment PDFhomeo pathyNo ratings yet
- Mechanisms of Diabetic ComplicatioDocument52 pagesMechanisms of Diabetic ComplicatioRaffaharianggaraNo ratings yet
- Star Group Health InsuranceDocument22 pagesStar Group Health InsurancePREM NATHNo ratings yet
- Food Quality and Food Safety: Learning ObjectivesDocument24 pagesFood Quality and Food Safety: Learning ObjectivesShanti Swaroop Chauhan shanti.chauhanNo ratings yet
- Cambridge IGCSE: BIOLOGY 0610/42Document20 pagesCambridge IGCSE: BIOLOGY 0610/42rachitNo ratings yet
- DR - Azad A Haleem AL - Brefkani: University of Duhok Faculty of Medical Science School of Medicine Pediatrics DepartmentDocument58 pagesDR - Azad A Haleem AL - Brefkani: University of Duhok Faculty of Medical Science School of Medicine Pediatrics DepartmentGomathi ShankarNo ratings yet
- Cardiac Cycle: BY: Makkawi .A.A. Osman B.SC, M.SC Department of Physiology Session NoDocument27 pagesCardiac Cycle: BY: Makkawi .A.A. Osman B.SC, M.SC Department of Physiology Session NoHomed OpriNo ratings yet
- Nursing Care For Patients With LungDocument14 pagesNursing Care For Patients With LungAyu RahayuniNo ratings yet
- Benign Essential Blepharospasm Information Page - National Institute of Neurological Disorders and StrokeDocument2 pagesBenign Essential Blepharospasm Information Page - National Institute of Neurological Disorders and StrokeJP OmerNo ratings yet
- Complete Head To Toe AssessmentDocument11 pagesComplete Head To Toe AssessmentKathleen Daban Ragudo100% (1)
- Five Machine Learning Supervised Algorithms For The Analysis and The Prediction of ObesityDocument9 pagesFive Machine Learning Supervised Algorithms For The Analysis and The Prediction of ObesityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Guide For Stop Using MethDocument16 pagesGuide For Stop Using MethDaniel Waluyo Sejati100% (2)
- Karen Clarke - BSDH PresentationDocument28 pagesKaren Clarke - BSDH PresentationWaheed UllahNo ratings yet
- Atheter Omenclature: R Freed A Urdaneta R Darflinger G VatakencherryDocument1 pageAtheter Omenclature: R Freed A Urdaneta R Darflinger G Vatakencherryamchoong100% (3)
- IN Trends and Issues in The Social Sciences: Tacloban CityDocument6 pagesIN Trends and Issues in The Social Sciences: Tacloban CityJhoefiel ParantarNo ratings yet
- Askep HivDocument17 pagesAskep Hivputri d dianiNo ratings yet
- MS4 Midterm NCLEX BurnsDocument5 pagesMS4 Midterm NCLEX BurnsDebbie Dela Cruz100% (5)
- Adoption MethodDocument18 pagesAdoption Methodsuchismita pandaNo ratings yet
- Nosocomial Infection. BPTDocument44 pagesNosocomial Infection. BPTAanchal GuptaNo ratings yet
- Neural Tube DefectDocument21 pagesNeural Tube Defectmariam bassemNo ratings yet
- The Impact of Social Media On Youth Mental Health:: Challenges and OpportunitiesDocument6 pagesThe Impact of Social Media On Youth Mental Health:: Challenges and OpportunitiesSajal HasinurNo ratings yet
- Patient Assesment 1Document23 pagesPatient Assesment 1luckyNo ratings yet
- Review of LiteratureDocument7 pagesReview of Literaturearjun singhaNo ratings yet
- Nursing Science Journal (NSJ) : e-ISSN: 2722-5054Document5 pagesNursing Science Journal (NSJ) : e-ISSN: 2722-5054Iskandar PakayaNo ratings yet
- Module 3 - Assessing and Diagnosing AbnormalityDocument33 pagesModule 3 - Assessing and Diagnosing Abnormalityxyryl ann mae capiliNo ratings yet
- Unit Plan Adult Health Nursing Unit IIDocument7 pagesUnit Plan Adult Health Nursing Unit IIDelphy Varghese100% (1)
- Rapid Assessment of Viral Hepatitis Testing and Quality AssuranceDocument18 pagesRapid Assessment of Viral Hepatitis Testing and Quality AssuranceCHELSIE KAITLYN DE GUZMANNo ratings yet
- Fascial SpacesDocument17 pagesFascial SpacesAlaa MoradNo ratings yet