You might also like
- Psychosexual TheoryDocument27 pagesPsychosexual Theoryrejeneil100% (1)
- Auditory Training For Central Auditory Processing DisorderDocument17 pagesAuditory Training For Central Auditory Processing Disorderrinecujucenir100% (1)
- Alternative Sexual Identities ExpressionDocument180 pagesAlternative Sexual Identities ExpressionHarmoniq777No ratings yet
- ASR-3000 Service ManualDocument26 pagesASR-3000 Service ManualYoussry Elsayed MohamedNo ratings yet
- The Effects of Oral Motor Exercises On Diadochokinetic RatesDocument23 pagesThe Effects of Oral Motor Exercises On Diadochokinetic RatesNicole GrayNo ratings yet
- (Central) Auditory Processing DisordersDocument39 pages(Central) Auditory Processing DisordersKatterine RebolledoNo ratings yet
- Alteraciones Del PACDocument20 pagesAlteraciones Del PACdr.ib979No ratings yet
- Bell Is 2015Document20 pagesBell Is 2015Diego Eduardo'HurtadoNo ratings yet
- Debonis 2008Document17 pagesDebonis 2008waslacson17No ratings yet
- Alzheimer'S Dementia Recognition Through Spontaneous Speech: The Adress ChallengeDocument5 pagesAlzheimer'S Dementia Recognition Through Spontaneous Speech: The Adress ChallengeRamKrishna108No ratings yet
- Doc2 InglDocument18 pagesDoc2 InglmariaNo ratings yet
- Evolving The Concept of APD PDFDocument11 pagesEvolving The Concept of APD PDFAnthonyNo ratings yet
- Report Information From Proquest: October 15 2014 11:23Document30 pagesReport Information From Proquest: October 15 2014 11:23vastyNo ratings yet
- Bellis Crosmodal 2011Document10 pagesBellis Crosmodal 2011Letícia Amado PachecoNo ratings yet
- Augmentative & Alternative Communication Intervention in Neurogenic Disorders With Acquired Dysarthria (Pamela Mathy)Document9 pagesAugmentative & Alternative Communication Intervention in Neurogenic Disorders With Acquired Dysarthria (Pamela Mathy)Piyush MalviyaNo ratings yet
- Tipos de Perdida InglesDocument7 pagesTipos de Perdida InglesPesántez Franco GemaNo ratings yet
- Audiologic Management of AuditoryNeuropathy Spectrum Disorder in ChildrenA Systematic Review of The LiteratureDocument12 pagesAudiologic Management of AuditoryNeuropathy Spectrum Disorder in ChildrenA Systematic Review of The Literaturericardorojas2403No ratings yet
- Heine, 2015 CapdDocument8 pagesHeine, 2015 CapdRicardo Jose De LeonNo ratings yet
- CAPD Check ListDocument12 pagesCAPD Check ListCaio LeônidasNo ratings yet
- Cad TestDocument8 pagesCad TestSajjadAhmad_QMCNo ratings yet
- 4 Article 13Document10 pages4 Article 13Manisha ChoudhuryNo ratings yet
- Morgan, 2009Document8 pagesMorgan, 2009Pamela Vega AmpueroNo ratings yet
- Prevalence of Oropharyngeal Dysphagia in The Netherlands: A Telephone SurveyDocument7 pagesPrevalence of Oropharyngeal Dysphagia in The Netherlands: A Telephone SurveyClaudia Lorena MedinaNo ratings yet
- Berlin Lake Como Paper in ColorDocument6 pagesBerlin Lake Como Paper in Colorczeigler100% (1)
- Evaluacion Aparaxia PDFDocument35 pagesEvaluacion Aparaxia PDFdmgarciagaNo ratings yet
- Otology: Special Paper in Celebration of Prof. Yang'S 50 Years Career in MedicineDocument6 pagesOtology: Special Paper in Celebration of Prof. Yang'S 50 Years Career in Medicinechipta lestariNo ratings yet
- Assessment of Childhood Apraxia of Speech: A Review/Tutorial of Objective Measurement TechniquesDocument34 pagesAssessment of Childhood Apraxia of Speech: A Review/Tutorial of Objective Measurement TechniquesgemapesfNo ratings yet
- Human Brain Mapping - 2020 - Sun - Cortical Reorganization Following Auditory Deprivation Predicts Cochlear ImplantDocument12 pagesHuman Brain Mapping - 2020 - Sun - Cortical Reorganization Following Auditory Deprivation Predicts Cochlear ImplantXilena HerreraNo ratings yet
- AdosDocument11 pagesAdoseducacionchileNo ratings yet
- Telehealth Intervention and Childhood Apraxia of Speech: A Scoping ReviewDocument14 pagesTelehealth Intervention and Childhood Apraxia of Speech: A Scoping ReviewAtalita AzevedoNo ratings yet
- Protocolo de Amplificacion DSLDocument28 pagesProtocolo de Amplificacion DSLRosario Lartiga MazryNo ratings yet
- Kent - Et - Al Acoustic in SSDDocument22 pagesKent - Et - Al Acoustic in SSDBetül Özsoy TanrıkuluNo ratings yet
- A Systematic Review of Telehealth Applications in Audiology: OriginalDocument20 pagesA Systematic Review of Telehealth Applications in Audiology: OriginalRoberta VianaNo ratings yet
- Jack 2011Document6 pagesJack 2011chiquitaputriNo ratings yet
- DTSCH Arztebl Int-117 0690Document12 pagesDTSCH Arztebl Int-117 0690CoAsst MuhammadNuhAlhudawyNo ratings yet
- Journal AlzheimerDocument10 pagesJournal AlzheimerFaza KeumalasariNo ratings yet
- CDT en DeliriumDocument11 pagesCDT en DeliriumAntonieta Cuevas GarcinuñoNo ratings yet
- Apraxia - Diagnostic Criteria of Developmental Apraxia of Speech Used by Clinical Speech-Language Pathologists at The Medical DictionaryDocument6 pagesApraxia - Diagnostic Criteria of Developmental Apraxia of Speech Used by Clinical Speech-Language Pathologists at The Medical DictionarySwathi GeethaNo ratings yet
- Evaluation of The Bangor Dyslexia Test (BDT) For Use With AdultsDocument38 pagesEvaluation of The Bangor Dyslexia Test (BDT) For Use With AdultsFiza JahanzebNo ratings yet
- Berit Kertscher Review Bedside Screening To Detect Oropharyngeal Dysphagia in Patients With Neurological Disorders 2013Document9 pagesBerit Kertscher Review Bedside Screening To Detect Oropharyngeal Dysphagia in Patients With Neurological Disorders 2013Maria De Los AngelesNo ratings yet
- Liégeois2014 Article NeuralCorrelatesOfDevelopmentaDocument13 pagesLiégeois2014 Article NeuralCorrelatesOfDevelopmentaMilenaNo ratings yet
- Ham Berger 2021Document14 pagesHam Berger 2021marilyn san martinNo ratings yet
- ICF Hearing LossDocument7 pagesICF Hearing LossAnindira RustandiNo ratings yet
- Ceklis Manajemen LukaDocument5 pagesCeklis Manajemen LukaGladys OliviaNo ratings yet
- Provoked Confabulations in Alzheimer's Disease - ScienceDirectDocument6 pagesProvoked Confabulations in Alzheimer's Disease - ScienceDirectsaudepreventiva89No ratings yet
- Alzheimer's DiseaseDocument17 pagesAlzheimer's DiseaseFega ArabelaNo ratings yet
- Implantación Coclear en Poblaciones Pediátricas Únicas.Document11 pagesImplantación Coclear en Poblaciones Pediátricas Únicas.Montserrat AravenaNo ratings yet
- 2019 Terbandetal - Assessment of Childhood ApraxiaDocument34 pages2019 Terbandetal - Assessment of Childhood ApraxiagemapesfNo ratings yet
- Archives of Oral BiologyDocument11 pagesArchives of Oral BiologyJohamurillocNo ratings yet
- A Systematic Review of Speech Assessments For Children With Autism Spectrum Disorder: Recommendations For Best PracticeDocument20 pagesA Systematic Review of Speech Assessments For Children With Autism Spectrum Disorder: Recommendations For Best PracticezvfaczyyNo ratings yet
- A Systematic Review of Treatment OutcomeDocument19 pagesA Systematic Review of Treatment OutcomeDayna DamianiNo ratings yet
- J Intellect Disabil Res - 2023 - Alex - Assessing Eating and Swallowing in Adults Born With Intellectual and MotorDocument16 pagesJ Intellect Disabil Res - 2023 - Alex - Assessing Eating and Swallowing in Adults Born With Intellectual and MotorBastian espejoNo ratings yet
- 5 7. Dutta Et Al-2018-American Journal of Speech-Language PathologyDocument29 pages5 7. Dutta Et Al-2018-American Journal of Speech-Language PathologyDimas Ade MahendraNo ratings yet
- Otonomy OTO-413 Presentation (November 5, 2018)Document10 pagesOtonomy OTO-413 Presentation (November 5, 2018)medtechyNo ratings yet
- Article Down MCIDocument10 pagesArticle Down MCIPablo delgadoNo ratings yet
- Articulo Disartria y Paralisis CerebralDocument10 pagesArticulo Disartria y Paralisis CerebralHaizea MuñozNo ratings yet
- Evaluation of The Bangor Dyslexia Test (BDT) For Use With AdultsDocument38 pagesEvaluation of The Bangor Dyslexia Test (BDT) For Use With AdultsAashique AliNo ratings yet
- Speech Assessment in Children With ChildhoodDocument14 pagesSpeech Assessment in Children With ChildhoodMaria de fatima MFconfecçõesNo ratings yet
- AAC and Autism: Compelling Issues, Promising Practices and Future DirectionsDocument4 pagesAAC and Autism: Compelling Issues, Promising Practices and Future DirectionsvcuadrosvNo ratings yet
- 2017 Mcneil - Apraxia of SpeechDocument28 pages2017 Mcneil - Apraxia of SpeechgemapesfNo ratings yet
- Bag Uley 2006Document2 pagesBag Uley 2006Harshit AmbeshNo ratings yet
- Novel Speech Signal Processing Algorithms For High-Accuracy Classification of Parkinson's DiseaseDocument8 pagesNovel Speech Signal Processing Algorithms For High-Accuracy Classification of Parkinson's DiseaseAbhay BarageNo ratings yet
- Orthodontics in Obstructive Sleep Apnea Patients: A Guide to Diagnosis, Treatment Planning, and InterventionsFrom EverandOrthodontics in Obstructive Sleep Apnea Patients: A Guide to Diagnosis, Treatment Planning, and InterventionsSu-Jung KimNo ratings yet
- Input Data Sheet For E-Class Record: Region Division School Name School Id School YearDocument18 pagesInput Data Sheet For E-Class Record: Region Division School Name School Id School YearRonie DacubaNo ratings yet
- Cul5a - Lecture - Week 9 - Singaporean Cuisine PDFDocument14 pagesCul5a - Lecture - Week 9 - Singaporean Cuisine PDFJJ GRNo ratings yet
- Petroleum and Petrochemical Bulletin: Free Water Determination Bulletin 09-01 Rev. 0Document2 pagesPetroleum and Petrochemical Bulletin: Free Water Determination Bulletin 09-01 Rev. 0hesigu14No ratings yet
- HUBUNGAN STRUKTUR, Ikatan Kimia Dan Aktivitas Fisiologis CompleteDocument67 pagesHUBUNGAN STRUKTUR, Ikatan Kimia Dan Aktivitas Fisiologis Completedatin suhaellaNo ratings yet
- Application of Softener On 100% Cotton Dyed Fabric by Exhaust Method.Document4 pagesApplication of Softener On 100% Cotton Dyed Fabric by Exhaust Method.Naimul HasanNo ratings yet
- Lennox Aqualean Awc Application Manual 32Document32 pagesLennox Aqualean Awc Application Manual 32André FerreiraNo ratings yet
- Chapter 2 Multiple 200 300 PDFDocument17 pagesChapter 2 Multiple 200 300 PDFRajeswari Rajarammurthy R0% (1)
- Hearnshaw TSBE Conference Paper 2012Document8 pagesHearnshaw TSBE Conference Paper 2012FUCKUNo ratings yet
- Pengaruh Penerapan Strategi Pelaksanaan Keluarga Terhadap Kemampuan Keluarga Merawat Pasien Halusinasi Di Kota Jambi Tahun 2017Document8 pagesPengaruh Penerapan Strategi Pelaksanaan Keluarga Terhadap Kemampuan Keluarga Merawat Pasien Halusinasi Di Kota Jambi Tahun 2017novanNo ratings yet
- BECG Assignment 5th SeptDocument4 pagesBECG Assignment 5th Septpragya dhancholiaNo ratings yet
- Suicidal Ideation and Behavior in Adults - UpToDate PDFDocument36 pagesSuicidal Ideation and Behavior in Adults - UpToDate PDFLemuel ReyesNo ratings yet
- Company Industry Employee Count Country: Plastic OmniumDocument4 pagesCompany Industry Employee Count Country: Plastic OmniumA AlamNo ratings yet
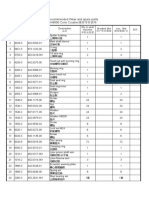
- Recommended Wear and spare parts H8800 Cone Crusher推荐零件清单Document3 pagesRecommended Wear and spare parts H8800 Cone Crusher推荐零件清单Lmf DanielNo ratings yet
- Rosen 20kw Hybrid Kit - 7hours Self ConsumptionDocument1 pageRosen 20kw Hybrid Kit - 7hours Self Consumptiongihan_maNo ratings yet
- Company Profile 2021Document18 pagesCompany Profile 2021Hamza FaheemNo ratings yet
- Types of Tissue - Nervous TissueDocument3 pagesTypes of Tissue - Nervous TissueFaye AquinoNo ratings yet
- SA Steam GenerationDocument6 pagesSA Steam GenerationRajagopalNo ratings yet
- SANRAYDocument39 pagesSANRAYgopinadh57No ratings yet
- Science: Quarter 1 - Module 2 Lesson 3: Changes in Matter and Its Effect in The EnvironmentDocument20 pagesScience: Quarter 1 - Module 2 Lesson 3: Changes in Matter and Its Effect in The EnvironmentTEAM KnightzNo ratings yet
- SOR Chave Tipo Boia-1550-Sor-1Document20 pagesSOR Chave Tipo Boia-1550-Sor-1Costa SimesNo ratings yet
- Electrodeposited Coatings of Rhodium For Engineering UseDocument5 pagesElectrodeposited Coatings of Rhodium For Engineering UsesamehNo ratings yet
- Declaration From Canadian MDs To Health Canada Re Safety Code 6Document3 pagesDeclaration From Canadian MDs To Health Canada Re Safety Code 6Seth BarrettNo ratings yet
- Event Safety Check List: Group NameDocument12 pagesEvent Safety Check List: Group NameUs Cosplay SpecialistNo ratings yet
- Arizona Community Foundation 2011 - Arizona Organizing Project Grant ApplicationDocument5 pagesArizona Community Foundation 2011 - Arizona Organizing Project Grant ApplicationElizabeth VenableNo ratings yet
- 1VDD006144 GB SafeRing - Plus - Air - April 2016Document74 pages1VDD006144 GB SafeRing - Plus - Air - April 2016Gary FortuinNo ratings yet
- Gsa PPDocument15 pagesGsa PPSheikh Sahil MobinNo ratings yet
- Class 9 Science Annual Paper 2 Prince Public SchoolDocument3 pagesClass 9 Science Annual Paper 2 Prince Public SchoolSHAURYA VARDHANNo ratings yet